Article Text

Abstract
Background: In primary Sjögren’s syndrome (pSS), extraglandular involvement might result from more intense stimulation of autoreactive B cells. Thus markers of B cell activation could be useful in the clinical assessment of this disease.
Objective: To investigate the association of serum B lymphocyte stimulator (BLyS) and β2 microglobulin with autoantibody production and extraglandular involvement in pSS.
Methods: Serum concentrations of BLyS and β2 microglobulin were analysed in 177 patients with pSS according to the American–European consensus group criteria. Serum β2 microglobulin was determined serially in 25 patients.
Results: Autoantibody secretion (presence of anti-SSA antibody alone or of both anti-SSA and anti-SSB) was associated with increased serum BLyS and β2 microglobulin. No correlation was found between BLyS and β2 microglobulin levels (p = 0.36). Serum concentrations of β2 microglobulin and C reactive protein and positive anti-SSB antibody results were associated with extraglandular involvement on univariate analysis (p<10−4, p = 0.003, and p = 0.004, respectively). Serum β2 microglobulin was also significantly increased in patients with extraglandular involvement without autoantibodies (mean (SD): 1.75 (0.7) v 1.39 (0.5) mg/l, p = 0.039). Multivariate analysis showed that extraglandular involvement was associated only with increased serum β2 microglobulin (p = 0.035, odds ratio = 2.78 (95% confidence interval, 1.07 to 7.22)). Among the 25 patients who had serial determinations of serum β2 microglobulin, the concentrations were increased in all those with disease flare and decreased in three following treatment. Serum BLyS, gamma globulin, IgG, and rheumatoid factor levels were not associated with features of systemic involvement.
Conclusions: Serum β2 microglobulin and BLyS reflect B cell activation in different ways in pSS. Serum β2 microglobulin assessment could be helpful as an activity marker in pSS.
- BLyS, B lymphocyte stimulator
- PSS, primary Sjögren’s syndrome
- SJC, swollen joint count
- SSA/SSB, Sjögren’s syndrome antigen A or B
- β2 microglobulin
- BLyS
- anti-SSA/SSB
- primary Sjögren’s syndrome
Statistics from Altmetric.com
- BLyS, B lymphocyte stimulator
- PSS, primary Sjögren’s syndrome
- SJC, swollen joint count
- SSA/SSB, Sjögren’s syndrome antigen A or B
Primary Sjögren’s syndrome (pSS) is an autoimmune disorder characterised by lymphocytic infiltration of the salivary and lachrymal glands leading to xerostomia and xerophthalmia. Polyclonal B cell activation and systemic production of autoantibodies are the hallmarks of the disease.1 Patients with pSS are at increased risk for the development of B cell non-Hodgkin’s lymphoma.2,3 Some evidence suggests that such lymphomas could arise from autoreactive B cells.4 Other systemic complications may occur, such as synovitis, myositis, vasculitis, renal, lung, or neurological involvement, and purpura. Patients with positive results for anti-SSA antibody or anti-SSA and anti-SSB antibodies have more frequent extraglandular complications than those with negative results.5 This higher frequency of extraglandular involvement may be a result of more intense stimulation of autoreactive B cells. Thus quantitative B cell activation markers, such as serum β2 microglobulin and B lymphocyte stimulator (BLyS; also known as BAFF, TALL-1, THANK, zTNF4, or TNFS13B), could be used clinically to assess disease activity.
β2 Microglobulin is the invariant chain of the major histocompatibility complex (MHC) class I molecules.6 The serum level of β2 microglobulin is increased in patients with renal insufficiency,7 plasmocytic and lymphocytic monoclonal proliferation (multiple myeloma and lymphoma,8,9,10 and HIV infection,11,12 being correlated with disease outcome and prognosis. In previous studies, β2 microglobulin was found to be raised in serum, saliva, and synovial fluid in patients with pSS.13–16
BLyS, a recently described member of the tumour necrosis factor (TNF)–ligand family,17,18 is essential for the control of B cell maturation and survival.19 Transgenic BLyS mice have large numbers of B cells in the peripheral blood, high levels of serum autoantibodies, and systemic lupus erythematosus (SLE)-like symptoms. In addition, lymphocytic infiltrates, similar to those observed in pSS patients, develop in these mice.20 In human autoimmune diseases, serum BLyS levels have been found to be increased in patients with SLE21 and pSS,22 and are correlated with serum autoantibody titres.
Clinicians need clinically relevant biological markers of pSS which could also be used in clinical trials of new drugs. Thus we investigated whether the serum levels of biological markers of B cell activation were correlated with autoantibody secretion and extraglandular involvement.
METHODS
Patients
Blood samples were collected from 177 white patients (170 female and seven male, mean (SD) age 56.6 (13.5) years) with pSS, as defined by the American–European consensus group criteria (including a focus score ⩾1 on labial salivary gland, or the presence of anti-SSA or anti-SSB antibodies),23 who consecutively attended the Departments of Rheumatology at the Hôpital de Bicêtre, Le Kremlin Bicêtre, and the Hôpital de Hautepierre, Strasbourg, France. Clinical and immunological features of the population studied are summarised in table 1. Extraglandular involvement was defined as the presence or confirmed records of purpura, lung and neurological involvement, synovitis, myositis, vasculitis, lymphadenopathy, enlarged spleen, or lymphoma during the evolution of the disease. Raynaud’s phenomenon was not included among the extraglandular manifestations. Because β2 microglobulin level can be modified in patients with impaired renal function, we decided not to include any with proven interstitial kidney disease. Extraglandular involvement was present in 73 patients (41.2%): 57 had extraglandular involvement at the time of the blood tests, and 16 had confirmed records of systemic involvement. Seventeen patients had two or more clinical features of systemic involvement.
Clinical and immunological features of 177 patients with primary Sjögren’s syndrome
Laboratory analysis
In all patients, antinuclear antibodies were detected by indirect immunofluorescence with the HEp-2000 substrate, which consists of HEp-2 cells transfected with Ro60-kd complementary DNA (Immunoconcepts, Sacramento, California, USA). Rheumatoid factor and serum IgA, IgG, and IgM values were determined by nephelometry. Serum levels of C3 and C4 were determined by nephelometry (Prospec nephelometer, Dade Behring, Manburg, Germany) in 146 patients. Normal values were 0.68 to 1.32 g/l for C3 and 0.14 to 0.33 g/l for C4. Anti-SSA and anti-SSB antibody levels were determined by commercial enzyme linked immunosorbent assay (ELISA) in all patients. The commercial Varelisa Ro antibody test (a recombinant SSA ELISA; Pharmacia-Upjohn, Freiburg, Germany) uses baculovirus expressed recombinant Ro52 and Ro60 coated in an unspecified ratio. The commercial Varelisa La antibody test (Pharmacia-Upjohn) uses recombinant La (48 kDa). All the positive anti-SSA/SSB results obtained by ELISA were confirmed by counterimmunoelectrophoresis with purified antigens obtained from rabbit and rat thymus powder (Pel Freez, Arkansas, USA) or from human spleen extract (Laboratoire d’Immuno-Pathologie, Hôpital Saint-Louis, Paris, France) and reference sera. Of the 177 patients, 111 (62.7%) had anti-SSA antibody, 58 (32.8%) also having anti-SSB antibody (table 1). No patient had anti-SSB antibodies without anti-SSA antibodies.
The serum β2 microglobulin level was determined using nephelometry (Array 360 system, Beckman Coulter Inc, Fullerton, California, USA). The diagnostic ranges had been established by the manufacturer in order to include 100% of a reference population of 136 healthy controls. A serum β2 microglobulin value of 2.11 or more was considered increased, according to the manufacturer’s recommendations. Patients with impaired renal function (serum creatinine ⩾120 μmol/l), previous lymphoma, or multiple myeloma were excluded from the β2 microglobulin analysis, as these conditions are known to be associated with increased serum β2 microglobulin. The serum β2 microglobulin level was analysed in 154 patients. Serial determinations were carried out in 25 patients.
A sandwich ELISA for measuring the soluble form of BLyS™ was used, with modifications of previously described procedures, in 137 patients. All serum samples were successively stored at −70°C and sent to the Division of Clinical Immunology and Rheumatology, University of Alabama (Birmingham, Alabama, USA) for serum BLyS assessment. Briefly, 96-well plates were coated with 2 µg/ml purified murine anti-BLyS monoclonal antibody (clone 3D4, mIgG1) in phosphate buffered saline (PBS) at 4°C overnight and blocked with 1% bovine serum albumin (BSA)/PBS. All specimens were diluted 1:10 in 3% BSA/PBS and incubated on the ELISA plate at 37°C for four hours. After being washed, the plate was incubated first with 0.2 µg/ml biotin conjugated polyclonal anti-BLyS antibody and then with 1:30 000 diluted horseradish peroxidase conjugated streptavidin (Southern Biotechnology, Birmingham, Alabama, USA). To avoid the confounding effect of rheumatoid factor activity, an mIgG1 isotype was used as a background control for the capture antibody with each specimen. The reaction was developed with trimethylbenzidine substrate (Sigma, St Louis, Missouri, USA), and read in an E-Max plate reader (Molecular Devices, Sunnyvale, California, USA). The absorbance values in the mIgG1 control wells were subtracted from the corresponding anti-BLyS capture wells and were typically less than 10% of total absorbance. The values obtained with parallel serum and plasma samples did not differ. A standard curve of serial dilutions of recombinant BLyS was incorporated into each assay. Normal BLyS values had been determined previously in 47 healthy volunteers using the same ELISA in the same laboratory (median serum BLyS level of 2.49 ng/ml (25th to 75th centile range, 1.96 to 2.96)).22 The serum values of both β2 microglobulin and BLyS were available in 114 patients.
Statistical analysis
We used χ2 tests (with Yates’s correction when appropriate) to assess the differences in frequencies for qualitative values. Analysis of variance (ANOVA) was used to analyse the associations between serum β2 microglobulin, BLyS, and gamma globulin, IgG, IgA, and IgM levels and extraglandular involvement. The results were validated by checking normality of the residues for each test. The Holm’s sequential Bonferroni procedure for multiple tests was used to correct p values according to the number of tests done in each series of comparisons.24 Multivariate analysis was undertaken with the use of logistic regression, which included significant risk factors of extraglandular involvement according to the results of the univariate analysis. Statistical analysis involved use of the SPSS 11.5 program.
RESULTS
Association between autoantibody production and serum β2 microglobulin and BLyS
Serum β2 microglobulin concentration was increased in 56 patients (36.4%). The serum β2 microglobulin value was significantly higher in patients with anti-SSA and anti-SSB antibodies (mean (SD), 2.43 (0.9) mg/l) than in those with anti-SSA antibody alone (1.82 (0.9) mg/l) or those without autoantibodies (1.5 (0.6) mg/l) (p<10−4; fig 1, table 2). In addition, serum β2 microglobulin was significantly correlated with serum rheumatoid factor (r = 0.33, p = 0.001), gamma globulin (r = 0.41, p = 0.001), IgG (r = 0.42, p = 0.001), C4 (r = −0.3, p = 0.001), and erythrocyte sedimentation rate (ESR) (r = 0.39, p = 0.001).
Values for relevant serum markers in patients with primary Sjögren’s syndrome according to the presence of anti-SSA or anti-SSB antibodies

Serum β2 microglobulin (β2m) and B lymphocyte stimulator (BLys) concentrations according to the presence of anti-SSA/SSB antibodies.
The mean BLyS serum level was higher in patients with anti-SSA antibody alone or with anti-SSA and anti-SSB antibodies (6.6 (8.8) and 5.9 (6.0) ng/ml, respectively) than in patients without autoantibodies (4.2 (6.8) ng/ml) (p = 0.05; fig 1, table 2), although this did not reach significance after statistical correction for multiple tests. In addition, serum BLyS was highly correlated with rheumatoid factor (r = 0.58, p = 0.001), IgM (r = 0.39, p = 0.001), and gamma globulin (r = 0.37, p = 0.002) but not IgG.
Although serum concentrations of β2 microglobulin and BLyS were both associated with the presence of anti-SSA or anti-SSB antibodies, no correlation was observed between β2 microglobulin and BLyS (r = 0.08, p = 0.36).
C3 and C4 levels were assessed in 146 patients and were decreased in 12 (12.9%) and 32 (21.9%), respectively. A decreased C4 level was significantly associated with autoantibody secretion (5.8% in patients without autoantibody, 25.6% in patients with anti-SSA alone, 35.2% in patients with anti-SSB, p = 0.001) (table 2). A decreased C4 level was also more common in patients with positive rheumatoid factor (30.1% v 11.9% in patients without rheumatoid factor, p = 0.02) or in patients with cryoglobulinaemia (100% v 20% in patients without cryoglobulinaemia, p = 0.004).
Association between β2 microglobulin and BLyS levels and extraglandular involvement
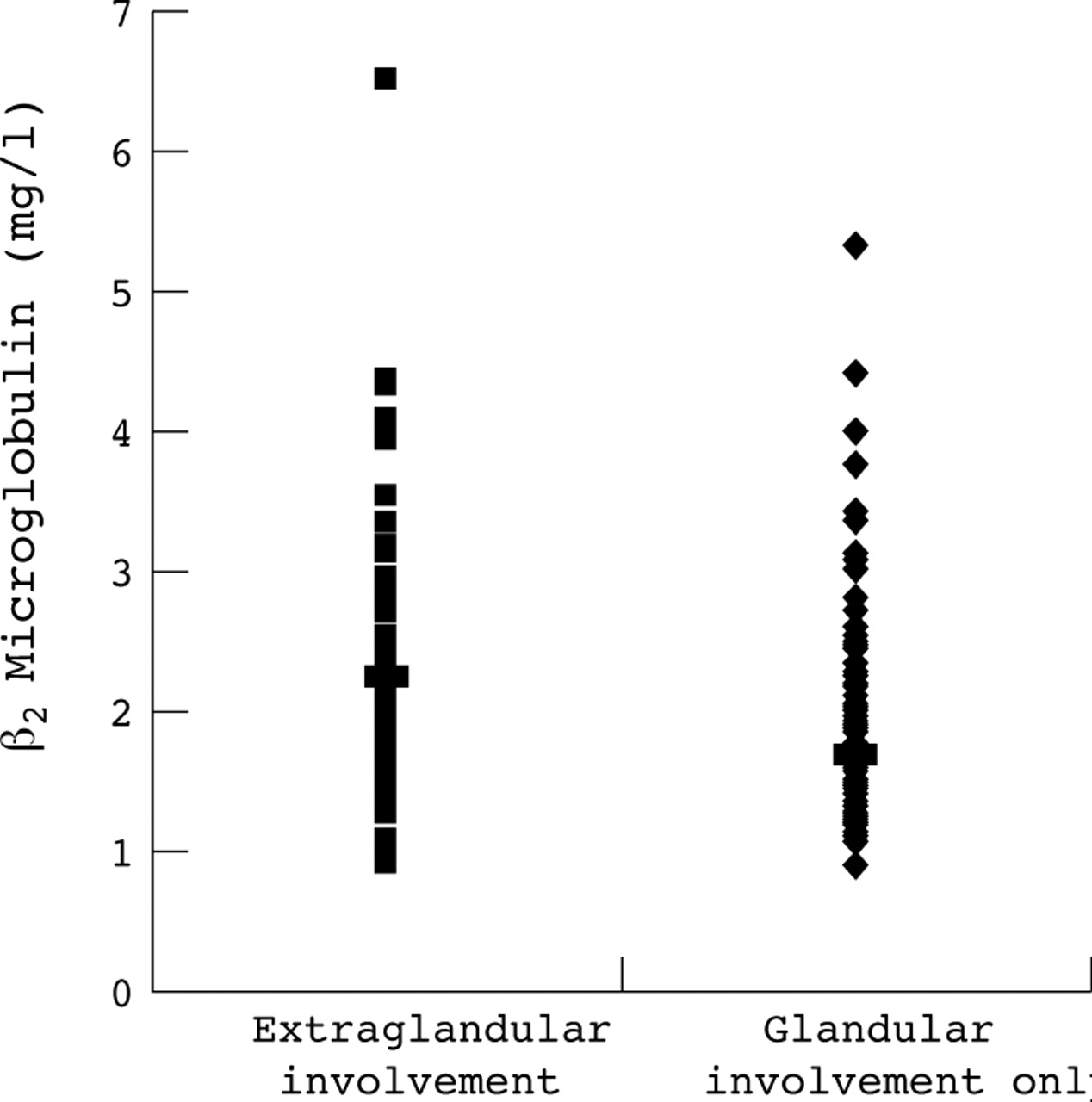
Among 13 potential predictive factors tested, only three were associated with extraglandular involvement on univariate analysis (table 3): a high serum β2 microglobulin concentration (2.2 (0.9) mg/l in patients with extraglandular involvement v 1.7 (0.8) mg/l in those without, p<10−4) (fig 2), the presence of anti-SSB antibody (43.8% of patients with extraglandular involvement v 25% of those without, p = 0.004), and a high C reactive protein level (10.5 (10.9) mg/l in patients with systemic disease v 6.1 (2.8) mg/l in those without). Increased serum BLyS, gamma globulin, IgG value, anti-SSA antibody alone, decreased C3 or C4 levels, and ESR were not associated with extraglandular involvement (table 3).
Univariate analysis of extraglandular involvement in patients with primary Sjögren’s syndrome

β2 microglobulin concentrations in patients with extraglandular involvement and in patients with glandular involvement only.
Multivariate analysis included significant risk factors identified by univariate analysis: serum β2 microglobulin, positive results for anti-SSB antibody, and C reactive protein level. As the data on C reactive protein were not available for the whole population, a second more potent model of logistic regression included serum β2 microglobulin level and the presence of anti-SSB antibody. Multivariate analysis showed that extraglandular involvement was associated only with increased serum β2 microglobulin levels in the model that included serum β2 microglobulin, positive anti-SSB results, and C reactive protein level (p = 0.035; odds ratio (OR) = 2.78 (95% confidence interval (CI), 1.07 to 7.22)), and also in the model including only serum β2 microglobulin and positive anti-SSB results (p = 0.018, OR = 2.41 (1.16 to 4.98)). It is noteworthy that the level of serum β2 microglobulin was increased with extraglandular involvement in patients without autoantibodies (1.75 (0.7) v 1.39 (0.5) mg/l; p = 0.039) and in patients with anti-SSA antibody alone (2.11 (0.80) v 1.66 (0.60) mg/l, p = 0.07), but not in patients with anti-SSA and anti-SSB antibodies (2.53 (0.90) v 2.32 (0.90) mg/l; p = 0.5; fig 3). Accordingly, in patients with an increased serum β2 microglobulin level, extraglandular involvement was independent of the presence of anti-SSB antibody (58.1% of patients with anti-SSB v 57.1% of patients without antibody, p>0.9).

{kind=link}
{kind=link}
{kind=link}
Mean serum β2 microglobulin value in 154 patients with primary Sjögren’s syndrome according to the presence of extraglandular involvement and of anti-SSA/SSB antibodies.
The serum β2 microglobulin level was raised in the presence of all clinical manifestations except neurological involvement. However, because of the small number of individual extraglandular manifestations, the increase did not reach significance except in the case of purpura (2.39 (0.8) v 1.86 (0.86) mg/l, p = 0.04). Serum BLyS was not significantly associated with any individual clinical manifestation. Neither increased serum β2 microglobulin nor BLyS levels were significantly associated with the presence of Raynaud’s phenomenon (RP): β2 microglobulin, 2 mg/l and 1.8 mg/l in patients with and without RP, respectively, p = 0.15; BLyS, 6.2 ng/ml and 5.2 ng/ml in patients with and without RP, p = 0.46.
Patients with extraglandular involvement were not significantly older and did not have a longer disease duration than those without extraglandular involvement (mean (SD): 56.2 (14.6) v 57.2 (12.5) years, respectively, p = 0.6; and 12.1 (7.0) v 12.4 (7.1) years, p = 0.75, respectively). Serum β2 microglobulin was not significantly higher in patients with active extraglandular disease at the time of the blood tests than in those with confirmed records of extraglandular involvement during the evolution of the disease (2.3 (1.1) v 1.9 (0.9) mg/l, p = 0.12). Serum creatinine was not significantly different in patients with increased serum β2 microglobulin levels (77.1 (11.9) v 75.7 (13.8) μmol/l, p = 0.53).
Longitudinal study of 25 patients
Twenty five patients without lymphoma or renal functional impairment had serial determinations of serum β2 microglobulin (mean (SD) number of samples per patient, 2.6 (1.3), range 2 to 7; mean follow up period, 23.5 (11.4) months). Sixteen patients showed no clinical change and no marked increase in serum β2 microglobulin. Six of the nine patients who experienced a significant increase in serum β2 microglobulin (a 50% increase or an increase above the normal value of 2.1 mg/l, or both) had changed clinical symptoms. Four patients had systemic involvement (synovitis in two; bronchial and bronchiolar involvement in one, and purpura in one), and two patients had disease flares (polyarthralgias in one; parotiditis and keratitis in the other). The swollen joint count (SJC) and β2 microglobulin concentration in one patient with polysynovitis (SJC = 9, β2m 4.32 mg/l, without treatment) went in parallel after the start of methotrexate and hydroxychloroquine treatment: SJC = 0, β2m 2.52 mg/l; SJC = 2, β2m 2.79 mg/l; and SJC = 6, β2m 2.97 mg/l. A parallel decrease in SJC and β2 microglobulin was also observed in another patient with polysynovitis (SJC = 4, β2m 3.97 mg/l, without treatment) after starting hydroxychloroquine: SJC = 2, β2m 4.18 mg/l; SJC = 0, β2m 3.6 mg/l; SJC = 0, β2m 2.44 mg/l, successively. Serum β2 microglobulin in a patient with distal bronchial and bronchiolar involvement treated with azathioprine rose from 1.81 to 2.59 mg/l during a lung flare, and normalised (1.74 mg/l) as the clinical situation improved. One patient had a concomitant decrease in the frequency of purpuric flares and the serum β2 microglobulin level (3.18 mg/l without treatment; 2.97 and 2.7 mg/l during hydroxychloroquine treatment, successively). One patient who developed polyarthralgias had a marked increase of serum β2 microglobulin from 1.96 to 3.22 mg/l. One patient with uncomplicated sicca eye symptoms and parotiditis who developed severe keratitis had a concomitant increase in serum β2 microglobulin from 2.1 to 2.4 mg/l.
DISCUSSION
In this study of 177 patients with pSS, serum BLyS and β2 microglobulin were both correlated with autoantibody secretion but not with each other. Extraglandular involvement was associated only with increased serum β2 microglobulin on multivariate analysis. Limitations of our study include its transverse design and the choice of a composite clinical parameter, extraglandular involvement (presence or confirmed records of systemic features during the evolution of disease). Of note, we confirmed the association between increased gamma globulin, IgG, rheumatoid factor levels, decreased C4 level, and anti-SSA/SSB autoantibodies.
To our knowledge, this is the first time that parallelism between an increase in serum β2 microglobulin and spread of the immune response from anti-SSA antibody alone to anti-SSA and anti-SSB has been demonstrated. Only one previous study has shown that patients with either anti-SSA or anti-SSB antibodies had a higher mean serum β2 microglobulin level than patients without these autoantibodies.25
The specific function of serum β2 microglobulin remains unknown in pSS, as in other lymphoproliferative diseases. β2 Microglobulin stabilises the tertiary structure of the MHC class I α chain6 and is required for the loading of peptides and the presentation of processed antigens to CD8+ T cells.26 In addition, the potential role of β2 microglobulin as an initiator of inflammatory response, apoptosis inducing factor, or inhibitor of dendritic cells has been reported.27–29 Serum β2 microglobulin could help process some autoantigens such as SSA or SSB by antigen presenting cells, as demonstrated in studies of exogenous antigens such as hepatitis B surface antigen particles.30 More probably, however, the serum β2 microglobulin level may only be a non-specific marker of immune activation, as it is correlated with other classical markers of B cell activation.
We confirmed the association between serum BLyS level and autoantibody production and the correlation between serum BLyS and gamma globulin, IgM, and rheumatoid factor levels.22
Unexpectedly, although serum β2 microglobulin and BLyS levels were both associated with autoantibody production, they were not correlated with each other. The respective biological origins of serum BLyS and β2 microglobulin may account for this discrepancy. BLyS is expressed by monocytes, dendritic cells, and, in pSS, by T cells infiltrating labial salivary cells.31 Its increase in pSS can be considered a pathogenic trigger of B cell activation. Conversely, β2 microglobulin may be expressed by all nucleated cells including B cells. Thus increased serum β2 microglobulin could reflect a later and more global stage of immune activation than the increase in serum BLyS.
Serum BLyS was not associated with features of systemic involvement, possibly because BLyS has no known direct proinflammatory properties. The role of serum BLyS as a disease activity marker is controversial in SLE; one study found an association between serum BLyS levels and the SLE disease activity index,32 whereas another study did not.33 Further longitudinal studies are required to investigate the role of serum BLyS as a marker of clinical activity in pSS. Likewise, serum IgG, C3, and C4 levels were not associated with extraglandular involvement. Thus the clinical relevance of decreased serum IgG and gamma globulin levels, which have been observed during treatment with hydroxychloroquine in patients with pSS,34–36 may be of minor importance.
We confirmed the association between extraglandular involvement and presence of anti-SSA+anti-SSB.37 The genetic determinism of the spread of the autoimmune response,38 along with the relative stability of anti-SSB titres over time,39 precludes the use of anti-SSB antibodies as disease activity markers in daily practice.
The most interesting finding of this study was the association between serum β2 microglobulin and extraglandular involvement on univariate and multivariate analysis. With respect to disease activity, the β2 microglobulin value could add significant information to routine measurements such as ESR or quantitative immunoglobulin values (which were not associated with extraglandular involvement on univariate analysis) or C reactive protein (which was not associated with extraglandular involvement on multivariate analysis).
Previously, serum β2 microglobulin has been shown to be increased in pSS patients with particular individual clinical manifestations such as distal renal tubular acidosis,40 disturbed lung function,41 and alveolitis.42 In addition, the results of a longitudinal cohort study showed that patients with pSS and subsequent lymphoma had higher baseline serum β2 microglobulin values.43 Interestingly, multivariate analysis revealed that serum β2 microglobulin added significant information about extraglandular involvement to that provided by positive anti-SSB antibody results. The increased level of serum β2 microglobulin with extraglandular involvement in the subgroup of patients without autoantibodies, as well as the high degree of extraglandular involvement in patients with increased serum β2 microglobulin levels with or without anti-SSB antibody, are two additional strong arguments in favour of the association between serum β2 microglobulin level and clinical features, independent of the presence of autoantibodies.
Our longitudinal follow up of 25 patients added important information on the potential clinical value of assessing serum β2 microglobulin. The levels appeared to be sensitive to change. Thus serum β2 microglobulin was increased in all patients with disease flare and decreased in three patients following a therapeutic response. This result confirmed that from a previous report detailing the evolution of serum β2 microglobulin level in nine patients, including two in whom lymphoma developed.13 Further longitudinal analysis with a larger population is needed to determine whether serum β2 microglobulin could represent a relevant disease activity marker in pSS, as proposed by Oxholm.44
CONCLUSION
Serum β2 microglobulin and BLyS explore B cell activation in different ways in pSS. Serum β2 microglobulin assessment could be helpful in this disease, for which few activity markers exist.45,46 The potential use of this simple, widely available, and inexpensive blood test deserves prospective analysis. Should its role be confirmed, serum β2 microglobulin level might also become a relevant surrogate marker for use in randomised controlled trials evaluating new drugs in pSS.
Acknowledgments
JEG was supported by the Institut Pour la Santé et la Recherche Médicale (INSERM).