Article Text

Abstract
OBJECTIVE The aim of this study was to investigate the concentrations of T cell derived cytokines in the synovial fluids (SFs) of patients with psoriatic arthritis (PsA) in comparison with rheumatoid arthritis (RA) and osteoarthritis (OA).
METHODS Th1 type cytokines (interleukin 2 (IL2), tumour necrosis factor β (TNFβ), and interferon γ (INFγ)) and Th2 type cytokines (IL4, IL10) were measured by means of enzyme linked immunosorbent assays.
RESULTS IL2 was usually not detectable in any of the disease groups. TNFβ was found in 3 of 31 PsA SFs (mean (SEM) 11.1 (2.3) pg/ml) and in a significantly lower concentration than in 20 of the 40 RA SFs (42.2 (15.6) pg/ml; p < 0.002). INFγ was measurable in 2 of 10 PsA and 6 of 16 RA SFs (p > 0.05). IL4 was present at low concentrations in 4 of 22 PsA SFs (0.41 (0.8) pg/ml), and in 15 of 20 RA SFs (0.63 (0.09) pg/ml; p < 0.01). IL10 was found in 4 of 27 PsA SFs (12.3 (0.9) pg/ml) and in 27 of 32 RA SFs (37.3 (4.9) pg/ml; p < 0.0001). In all OA SFs cytokine concentrations were below the limit of detection.
CONCLUSION The pattern of T cell derived cytokines in PsA SFs was similar to that of RA SFs. However, both the frequency and the concentrations of cytokines were lower in PsA SFs than in RA SFs, while OA SFs generally lacked any detectable T cell cytokines altogether. The presence of Th1 and Th2 cell derived cytokines in PsA SFs suggests the presence of activated T cells in the inflamed joint tissues and their participation in the immunoinflammatory events.
- psoriatic arthritis
- rheumatoid arthritis
- cytokines
- T cells
- synovial fluids
Statistics from Altmetric.com
T cells are important cellular components in the development of inflammatory joint diseases such as rheumatoid arthritis (RA).1 2 Psoriatic arthritis (PsA), an inflammatory seronegative disease of unknown aetiology, is also characterised by the infiltration of joints and involved skin by activated T cells.3 The synovial membranes of PsA and RA cannot be differentiated from each other by immunohistology.4
Activated T cells belong to two major subpopulations, which may be differentiated by their cytokine profiles: Th1 cells produce the proinflammatory cytokines interleukin 2 (IL2), tumour necrosis factor β (TNFβ), and interferon γ (INFγ), while Th2 cells synthesise the anti-inflammatory cytokines IL4 and IL10.5 As the role or presence of T cell derived cytokines in PsA is still unknown, we investigated them and compared them with those in RA and osteoarthritis (OA).
Methods
PATIENTS
Synovial fluids (SFs) from 35 patients with PsA, 60 patients with RA6, and 25 patients with OA7 were analysed. Table 1 gives details of the patients.
Demographic data of the patients (mean (SEM))
At the time of arthrocentesis swollen and tender joints, morning stiffness, erythrocyte sedimentation rate (ESR), and C reactive protein (CRP) were determined as markers of disease activity in PsA and RA. In addition, the leucocyte counts and rheumatoid factor (RF) values in the SFs were measured.
The SFs were obtained from knee joint effusions, treated with hyaluronidase (20 μg/ml SF; H-2251 sheep testes, type III, Sigma, St Louis, MO, USA), centrifuged, and the supernatant used to determine the cytokines.
CYTOKINE ASSAYS
All of the test kits for T cell derived cytokines were commercial “sandwich” enzyme linked immunosorbent assays (ELISA) and were used according to the manufacturers’ instructions. The lower limits of detection were as follows: for IL2 (Research and Diagnostic Systems (R and D), Minneapolis, USA; Quantikine) 31 pg/ml; for IL4 (R and D, Quantikine HS with high sensitivity) 0.25 pg/ml, for IL10 (Medgenix Diagnostics SA, Fleurus, Belgium) 11 pg/ml; for TNFβ (Bender MedSystems, Vienna, Austria) 7 pg/ml, and for INFγ (Endogen, Cambridge, MA, USA) 15 pg/ml.
STATISTICAL ANALYSIS
The parameter free two tailed Mann-Whitney U test for independent samples was used to analyse statistical significances as indicated; p values below 0.05 were considered significant. Similar results were obtained with the χ2 test. All concentrations are presented as mean (SEM).
Results
In all OA SFs cytokine concentrations were below the limits of detection.
INTERLEUKIN 2
IL2 was not detectable in PsA SFs or RA SFs (with two exceptions).
TUMOUR NECROSIS FACTOR β
Three of 31 (10%) PsA SFs contained TNFβ (mean 11.1 (2.3 pg/ml)) as did 20 of 40 (50%) RA SFs (mean 42.2 (15.6) pg/ml; p < 0.002 compared with PsA), (fig 1A).

Concentrations of Th1 cell derived cytokines in synovial fluids ((shaded bars) mean concentration (SEM); solid line shows limit of detection). (A) TNFβ of patients with osteoarthritis (OA, n = 6), psoriatic arthritis (PsA, n = 31), and rheumatoid arthritis (RA, n = 40); (B) INFγ of patients with osteoarthritis (OA, n = 9), psoriatic arthritis (PsA, n = 10), and rheumatoid arthritis (RA, n = 16).
INTERFERON γ
INFγ was found in 2 of 10 (20 %) PsA SFs (mean 16.7 (1.2 pg/ml)) and in 6 of the 16 (45%) RA SFs (mean 28.2 (5.3) pg/ml; p > 0.05 compared with PsA), (fig 1B).
INTERLEUKIN 4
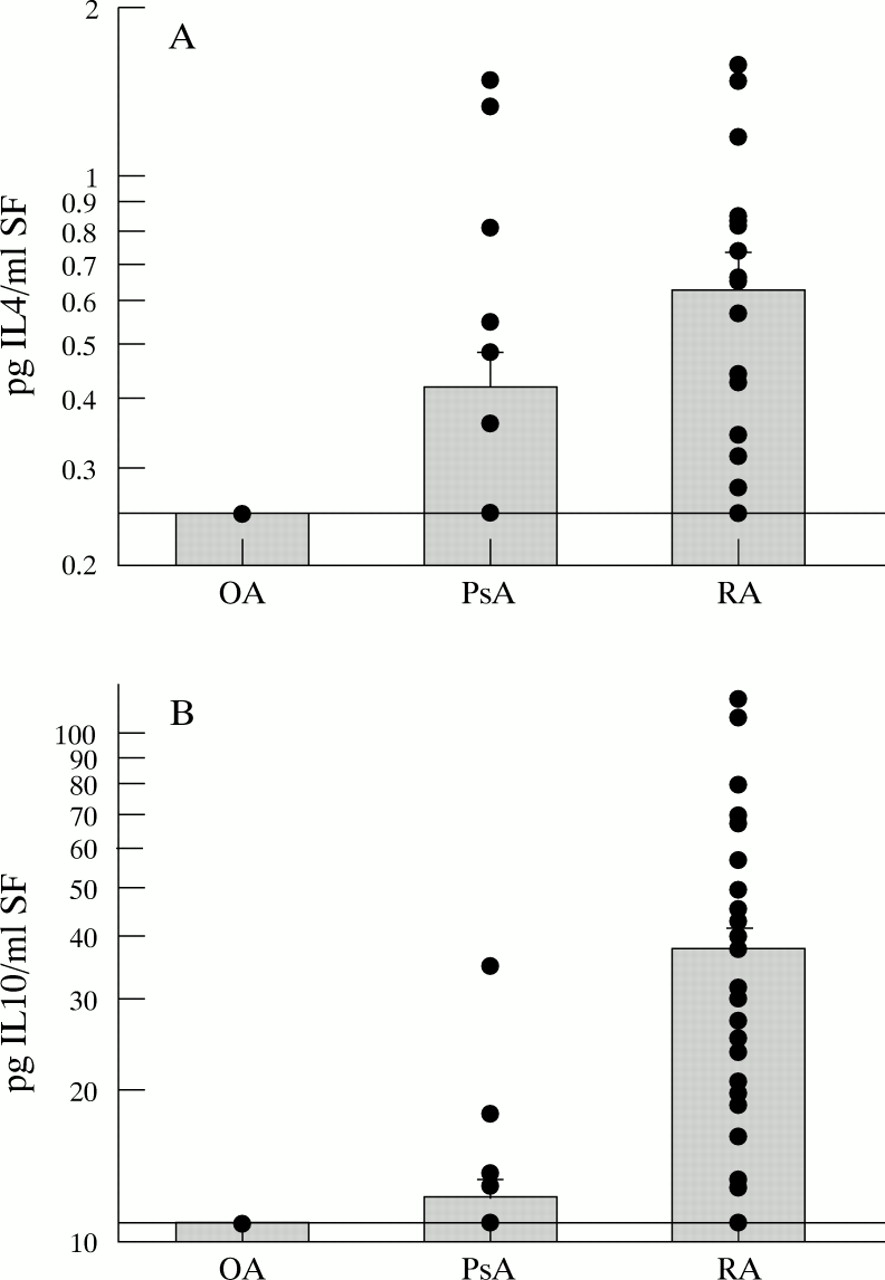
IL4 (fig 2A) was found in 4 of 22 (18%) PsA SFs (mean 0.41 (0.08 pg/ml)) but in significantly lower concentrations (p < 0.01) than in 15 of the 20 (75%) RA SFs (mean 0.63 (0.09) pg/ml).

{kind=link}
{kind=link}
Concentrations of Th2 cell derived cytokines in synovial fluids ((shaded bars) mean concentration (SEM); solid line shows limit of detection). (A) IL4 of patients with osteoarthritis (OA, n = 15), psoriatic arthritis (PsA, n = 22), and rheumatoid arthritis (RA, n = 20); (B) IL10 of patients with osteoarthritis (OA, n = 16), psoriatic arthritis (PsA, n = 27), and rheumatoid arthritis (RA, n = 32).
INTERLEUKIN 10
IL10 (fig 2B) was detected in only 4 of 27 (15%) PsA SFs (mean 12.3 (0.9) pg/ml), but in 27 of 32 (84%) RA SFs where it was also found in much higher concentrations than in the PsA SFs (mean 37.3 (4.9) pg/ml; p < 0.0001).
Discussion
In this study T cell derived cytokines were detected in 10 to 20% of PsA SFs. However, the frequencies and values of TNFβ, IL4, and IL10 were significantly higher in RA. The concentrations of INFγ did not statistically differ in PsA and RA SFs even though it is also produced by CD8+ cells, which are increased in PsA SFs.8 None of these lymphokines was found in OA SFs.
From a quantitative point of view, the Th1 derived cytokines TNFβ and INFγ were found in much higher concentrations than the Th2 lymphokine IL4. This indicates that Th1 cytokines may be a major factor in the inflammation of PsA. This has been accepted for arthritis in other seronegative spondylarthropathies and for RA.9 10 The sensitivity of the assay used permitted the detection of lower concentrations of IL4 than was previously possible.11
In contrast, IL10 was readily found, although of all the cytokines analysed it is the only one that is also readily produced by non-T cells.12 The lower frequency and concentrations of IL10 in PsA SFs may therefore be because of the lower numbers of macrophages in the synovial membranes of PsA compared with RA patients.13
The presence of lymphokines in SFs has its synovial membrane correlate in RA. Moreover, we have also observed that the same proinflammatory monokines that are characteristic of RA, namely TNFα and IL1β are also found in PsA SFs, albeit at lower concentrations and frequencies.14 These observations in conjunction with the findings reported here indicate that the psoriatic joint inflammation bears similarities to rheumatoid inflammation, but to a lesser extent. This is well in line with both the potential of PsA to be a destructive, erosive joint disease and its generally more benign nature compared with RA.15
Because of the lack of validated criteria for disease activity in PsA, the same criteria were used for both PsA and RA.16 This represents a somewhat limiting factor in our study, as the parameters chosen may not reflect disease activity to the same extent in the two diseases.
Our conclusions are in agreement with earlier observations about similarities between the histological changes in PsA and RA.4 The diversity in genetic associations as well as the probable heterogeneity in the hitherto unknown aetiological events and the nature of eliciting (and/or perpetuating) antigens may govern the differences between the two diseases.
The results obtained suggest that T cells participate actively in the immunoinflammatory events in PsA. Thus targeting T cells may be an important therapeutic approach in this disease. This notion is supported by the efficacy of cyclosporin A, a compound that targets T cell lymphokine gene activation in PsA.17
Acknowledgments
This study was supported by grants from the Austrian Ministry of Health, Sports and Consumer Protection (Zl 236.065/3-II/A/6/91) and the City of Vienna (Department of Urban Development, Planning and Scientific Affairs). The authors are grateful to Ing Christine Schwarzer for her excellent laboratory work and to Erika Karner for expert secretarial assistance.