Article Text

Abstract
OBJECTIVE The purpose of this study was to compare the long term effectiveness between chloroquine (CQ) and hydroxychloroquine (HCQ).
METHODS Medical charts of all patients seen by eight rheumatologists practising in two tertiary care centres and starting antimalarial treatment between January 1985 and December 1993 were reviewed. Patient characteristics, disease, and treatment information were collected. The main outcome measures were the cause of and the time to the discontinuation of antimalarial drugs resulting from all causes, principally toxicity or inefficacy, or both. Bivariate analysis including t tests and χ2 tests were used to assess differences between means and proportions respectively. Survival curves were evaluated using the Kaplan-Meier method. Multivariate analysis (Cox regression) was used to adjust for potential confounders.
RESULTS After all medical records were reviewed, 1042 eligible cases were identified. From these, 940 (90%) had usable information and they represent the cohort. Five hundred and fifty eight had rheumatoid arthritis, 178 had systemic lupus erythematosus, 127 had palindromic arthritis, and 77 had other diagnoses. Fifty seven per cent of the patients received CQ and 43% HCQ. The proportion of patients with side effects taking HCQ and CQ was 15% and 28% respectively (p=0.001). Using Cox regression model to adjust for age at the onset of antimalarial treatment, physician differences, sex, disease type, disease duration before treatment, and rank selection, there were no differences in the hazard ratio (HR) for overall discontinuations between CQ and HCQ. While the HR for discontinuations because of toxicity was lower for HCQ (HR= 0.6, 95% CI 0.4, 0.9), the HR for discontinuations because of inefficacy was significantly higher for HCQ (HR= 1.4, 95% CI 1.1, 1.9).
CONCLUSIONS After adjusting for time and several confounders HCQ was less toxic but less effective than CQ. Only one case of probable/possible retinopathy was found. Therefore, we propose a careful baseline ophthalmological evaluation by an expert and then one or every two years if proper doses are used.
- antimalarial drugs
- long term effectiveness
- efficacy
- toxicity
- rheumatic diseases
Statistics from Altmetric.com
Antimalarial drugs have become one of the most commonly prescribed drugs in the treatment of many rheumatic diseases such as rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), palindromic arthritis (PA), and psoriatic arthritis.1-7This seems to be related mainly to their low toxicity in comparison with the other antirheumatic agents.7-10 Chloroquine (CQ) and hydroxychloroquine (HCQ) are the only 4-aminoquinoline derivatives that are used as antirheumatic drugs,11 and although structural similarities between CQ and HCQ exist, it has been suggested that there are differences in efficacy and in toxicity.12-16 In addition, there are considerable differences in costs between these two drugs, HCQ being seven times more expensive than CQ, at least in Canada. Differences in the prescription patterns for antimalarial drugs among rheumatologists have been reported.10 17 18 Long term effectiveness (efficacy and toxicity under non-experimental conditions) should be considered when selecting one drug over another. However, most studies reviewing the long term effectiveness of antimalarial drugs considered both drugs as a single group.6-10
In this study we evaluated the long term effectiveness of antimalarial drugs in rheumatic diseases, also considering potential differences between CQ and HCQ.
Methods
STUDY POPULATION
A cohort of patients with several rheumatic disorders who received antimalarial treatment was retrospectively assembled. All eight rheumatologists practising in Edmonton between 1985 and 1993 participated in the study permitting us to review their medical records. All the records of patients with any rheumatic disorder who received any antimalarial drug were further reviewed. Patients were eligible for the study according to the following criteria: (a) diagnosis of any rheumatic disorder confirmed by a rheumatologist, (b) onset of antimalarial treatment between January 1985 to December 1993. All medical records were reviewed by one of us (JAAZ) and the information about antimalarial treatment was recorded on a structured form. Patient characteristics, disease, and other treatments were also recorded. The main outcome measures were the cause and time of discontinuation. The following were considered as causes of discontinuation according to the treating rheumatologist: (a) inefficacy, (b) toxicity, (c) other, and (d) uncertain.
STATISTICAL ANALYSIS
The χ2 test with Yates’s corrections were used to compare differences in proportions. Two tailed Student ttests were used to compare differences in means between two groups. Kaplan-Meier survival analyses were performed to estimate rates of discontinuation for each drug. Cox regression models were used to evaluate the effects of age, sex, disease type, disease duration, rank selection (the order in which the different antimalarial drugs were chosen for treatment), rheumatologist, and type of antimalarial drug. Hazard ratios (HR) were estimated for discontinuation of use because of: (a) all causes, (b) toxicity, and (c) inefficacy. Models were built using two methods: (1) Univariate: each variable was entered separately to test whether that single variable was a significant predictor. (2) Multivariate (best model): this model was an investigator driven model with the purpose of finding the variables that explained most of the variability of the dependent variable. This model was built in a forward stepwise fashion using the likelihood ratio test as method for comparison and selection of the variables as well as the models. All the analyses were performed using SPSS for Windows, version 6.1.
Results
After all medical records were reviewed, 1042 eligible cases were identified. From these, 940 (90%) had the minimum required information. Table 1 shows the patient and clinical characteristics of the study group. RA accounted for 59% of the antimalarial prescriptions, followed by SLE (19%), PA (14%), and other various diseases (8%). CQ accounted for 58% of the antimalarial prescriptions and was the main antimalarial in all disease groups. Six per cent of the patients received both antimalarial drugs at different times, however, only the first antimalarial drug received was considered in the analysis.
Patients characteristics
Overall, antimalarial drugs were the first choice for second line treatment in 72% of the patients. Six per cent of the patients received more than one course of antimalarial treatment. However, for the purposes of this study only the first cycle was included in the analysis.
DISCONTINUATION OF TREATMENT
At the time of data collection 50% of the patients were still receiving the drug (table 2). Fifteen per cent and 19% of the cases discontinued the drug because of toxicity and inefficacy respectively. Other various reasons accounted for 16% of discontinuations. Toxicity was the main cause of discontinuation for CQ while inefficacy was for HCQ.
Reason for discontinuation of AM in total (and by drug)
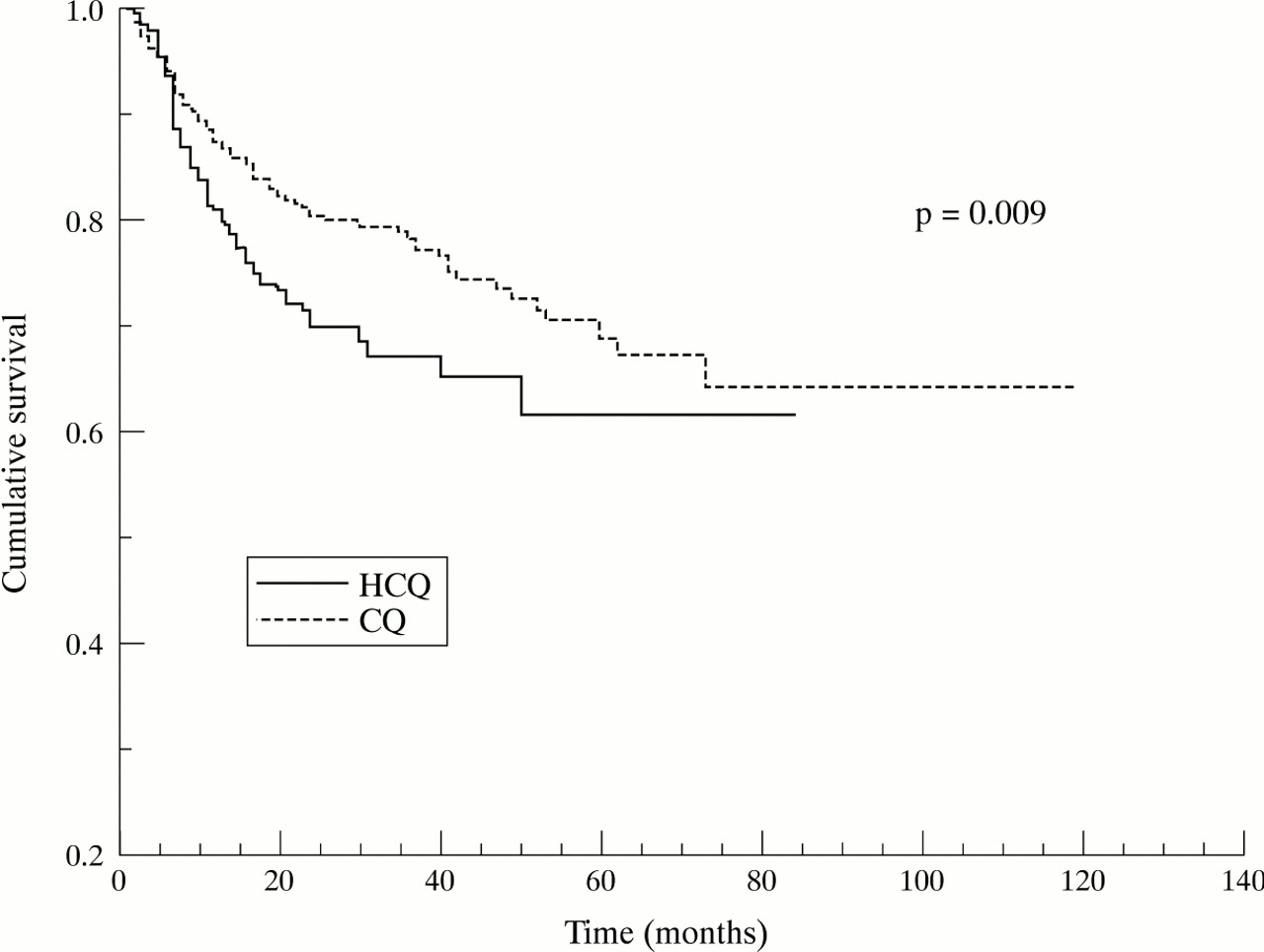
Survival analysis was conducted using the Kaplan-Meier product limit method to calculate the proportion of patients still receiving antimalarial drugs at different points in time. Survival was calculated for each drug for all causes of discontinuations, toxicity, and inefficacy (figs 1 to 3). Overall, around 30% of the patients were still receiving treatment at 120 months with no differences between CQ and HCQ (fig 1). This similarity is seen across all different points in time. However, when survival curves were estimated for discontinuations resulting from toxicity alone (all other causes of discontinuation and no discontinuations were considered as censored) a trend for more discontinuations in patients who received CQ than those who received HCQ was seen. However, this difference was not statistically significant using the log rank test (fig 2). Inefficacy discontinuations between CQ and HCQ were statistically significant (log rank test p= 0.009) (fig 3). Patients who received CQ discontinued less often as a consequence of inefficacy than patients who received HCQ. This difference starts to be noticeable at about one year and continues until 70 months when a plateau is reached in both drugs.

Kaplan-Meier curves for any cause of discontinuation of treatment.

Kaplan-Meier curves for discontinuation of treatment because of inefficacy.

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves for discontinuation of treament because of toxicity.
Multivariate analysis was used (Cox regression) to examine the associations of different variables with the outcome of antimalarial treatment (for example, overall, toxicity, and inefficacy discontinuations). Initially all the variables were modelled individually (univariate) and results are shown in table 3. Type of antimalarial drug was a significant predictor only for discontinuations resulting from inefficacy. Thus HCQ had a higher chance of discontinuation because of inefficacy than CQ (HR= 1.4; 95%CI 1.09, 1.99). A second model was built (multivariate), this was an investigator driven model with the purpose of finding the best predictor variables. For all causes of discontinuation, disease type and physician were the best predictor variables (table 4). Thus, patients with SLE and PA had less chance of discontinuation than patients with RA. Type of antimalarial drug was not a significant predictor in this model. When the same variables were evaluated to find the best predictors for discontinuation because of toxicity, type of antimalarial drug was a statistically significant predictor. Thus, patients who received HCQ had less chance of discontinuation resulting from toxicity than patients who received CQ (HR= 0.62; 95% CI 0.40, 0.96) (table 4). For discontinuation resulting from inefficacy type of antimalarial drug was a significant predictor among others with patients receiving HCQ at higher risk for discontinuation (HR = 1.4; 95% CI 1.06, 1.96).
Cox regression for discontinuation of treatment (univariate)
Cox regression for discontinuation of treatment (multivariate)
SIDE EFFECTS
Overall, there were 212 (23%) cases who experienced side effects. Of these only 146 (69%) required discontinuation of the drug permanently, 11 (5%) discontinued the drug temporarily, 12 (6%) required only a decrease in dose, 27 (13%) switched to the other antimalarial drug, and 45 (21%) did not require any action. Fifty nine (15%) of those who received HCQ had side effects in comparison with 153 (28%) of those with CQ (p<0.00001): of these, 48 (81%) and 97 (64%) respectively discontinued the drug permanently (p<0.01). Furthermore, there were significant differences in the type of side effects (table 5), all of them in favour of HCQ. Certain rare side effects such as hair bleaching (two cases), nightmares (four cases), and neuromyopathy (six cases) occurred only in patients with CQ. With respect to retinal toxicity three possible cases were identified (two with CQ and one with HCQ) and that was the reason of discontinuation. However, when these patients were re-evaluated by a retinologist with experience in senile and antimalarial maculopathy, only one case could be retained as retinal changes “probably” related to CQ . These changes disappeared after CQ was discontinued.
Side effects between AM
Discussion
Although CQ and HCQ have been used for the treatment of rheumatic diseases for more than 40 years, they have been considered as a single drug in the few studies that have evaluated long term effectiveness.7-10 Therefore, to our knowledge this report is the first comparing the long term effectiveness of CQ and HCQ.
In general, the characteristics of this cohort are similar to those reported elsewhere for patients receiving antimalarial treatment.1 5 7-10 19 The female-male ratio was 3 to 1 (table 1) in accordance with the demographic distribution of rheumatic diseases. More discontinuations because of toxicity were seen in patients receiving CQ (table 2). This trend was also seen in the Kaplan-Meier curves although with this type of analysis it did not reach a statistically significant difference (fig 2). Furthermore, in the multivariate analysis the HR for discontinuation because of toxicity was lower for HCQ (HR= 0.62; 95% CI 0.40, 0.96). In other words, after adjusting for time and several confounders patients taking CQ were 40% more likely to discontinue because of toxicity than patients who received HCQ. On the other hand—again after adjustment for time and confounders—patients taking HCQ had a 40% larger chance of discontinuing the drug because of inefficacy.
Five per cent of the patients had more than one cycle of antimalarial treatment and we decided to analyse only the first cycle to simplify the analysis. Thus, we were interested in the outcome of the antimalarial drug received for the first time. Moreover, including several outcomes in the same patient receiving the same drug at different times may produce bias, as patients could discontinue the drug early or later based on their previous experience with the drug. In addition, for those patients who received both drugs only the first antimalarial drug was included in the analysis. This was to avoid bias because the second antimalarial drug would depend on which was the first antimalarial drug. Furthermore, toxicity would be the only reason to choose another drug as discontinuation because of inefficacy would hardly be associated with a second attempt with the other antimalarial drug.
A limiting factor of this study was that we did not have baseline characteristics of disease to adjust for. However, there is no evidence to suggest that disease severity influenced the rheumatologist to prescribe one of the antimalarial drugs in preference to the other. This is more related to patterns of practice, which we had previously reported for the rheumatologists who participated in the study.17 18 We did not evaluate factors associated with patterns of prescriptions for the two antimalarial drugs. However, all but two rheumatologists have been using the same antimalarial drug while practising. In addition, we observed differences in the rates as well the causes of discontinuation among rheumatologists, and we adjusted for these differences in the multivariate analysis. Concomitant use of corticosteroids was not registered in the study and this could have contributed to the effectiveness. If this were the case then the effect of this would probably not be important because the use of corticosteroids by the specific rheumatologists participating in the study has already been reported to be low10 (at least in RA, which was the main disease group).
Overall, the prevalence of side effects was higher in patients who received CQ. Of interest, rare side effects like retinopathy or pre-maculopathy (one possible case), hair bleaching (two cases), and neuromyopathy (six cases) occurred only in patients treated with CQ, which confirm previous reports that clinically significant side effects are more likely to occur with CQ.15 21 Three patients were reported to have retinal changes that were suggestive of retinopathy (two had RA and one had SLE). All of them received the antimalarial drug at conventional doses (250 mg/day for CQ and 400 mg/day for HCQ). However, when they were sent to a retinologist with experience in retinopathy resulting from antimalarial treatment, only one case was defined as retinal changes possibly/probably related to CQ. This patient had SLE and had received CQ for 59 months at a dose of 4.5 mg/kg/day with a cumulative dose of 447.4 g. The patient was followed up and retinal changes disappeared. Nineteen months after CQ was discontinued she received HCQ, with no recurrence of the retinal changes at her most recent ophthalmological evaluation. Our results confirm previous and recent findings (particularly focused on HCQ 25–27) that retinopathy is a very rare complication when conventional doses are used, and that daily dose based on ideal body weight (<4 mg/kg/day for CQ and <6 mg/kg/day) may be more important than cumulative doses in the development of this major complication.15 22-29 Furthermore, there have been other patients within and outside this study where a confident diagnosis of antimalarial retinopathy made by a local ophthalmologist was not supported when this patient was reviewed by an expert. Monitoring ocular toxicity twice a year or three times a year as recommended by manufacturers seems excessive and may not be cost effective as recently reviewed by MacLean et al for HCQ.30 Hence, we suggest that patients who receive antimalarial treatment should have a careful “baseline” ophthalmological evaluation by an expert (that is, within the first few months of use) and then every one or two years. The physician responsible for the ongoing patient’s care could monitor ocular toxicity using less expensive and less time consuming methods such as Amsler’s grid on each patient visit.
In summary, in this study crude rates of discontinuations were different for each drug. The main cause of discontinuation for antimalarial treatment in general and for HCQ was inefficacy with 19% and 21% respectively. In contrast, the main cause of discontinuation for CQ was toxicity (18%). The multivariate analysis showed that HR for discontinuations because of toxicity are lower for HCQ(HR=0.62,95%CI0.60, 0.96), and HR for discontinuations because of inefficacy are higher for HCQ (HR=1.4, 95% CI 1.06, 1.96). No significant differences were observed between CQ and HCQ in terms of HR for overall discontinuations. Therefore, if we use rates of discontinuation as a measure of effectiveness the long term effectiveness between CQ and HCQis similar. Nevertheless given the apparent differences in efficacy and toxicity between the two drugs (as well as economic differences) potential trade offs between increased efficacy and increased toxicity, and vice versa, should be carefully considered by the patient and physician when selecting antimalarial treatment. Ocular and neuromuscular side effects occurred more often in patients who received CQ. No cases of definite retinopathy were found. Monitoring each six months for ocular toxicity seems to be excessive if conventional doses are used.
Acknowledgments
The authors wish to thank the rheumatologists in Edmonton. This study would not have been possible without the cooperation of Dr Stephen Aaron, Dr Paul Davis, Dr Avril Fitzgerald, Dr Sharon LeClercq, Dr Walter P Maksymowych, Dr John Percy, and Dr Keneth Skeith.