Article Text

Abstract
Objectives To assess the kinetics of humoral response after the first and second dose of messenger RNA (mRNA) vaccines in patients with inflammatory joint diseases compared with healthy controls (HC). To analyse factors influencing the quantity of the immune response.
Methods We enrolled patients with rheumatoid arthritis (RA) and seronegative spondyloarthritis (SpA), excluding those receiving B-cell depleting therapies and assessed the humoral response to mRNA vaccines after the first and the second dose of the vaccine in terms of seroconversion rate and titre. We compared the results to a HC group and analysed the influence of therapies as well as other characteristics on the humoral response.
Results Samples from 53 patients with RA, 46 patients with SpA and 169 healthy participants were analysed. Seroconversion rates after the first immunisation were only 54% in patients with inflammatory arthritis compared with 98% in the HC group. However, seroconversion rates were 100% in all groups after second immunisation. Patients developed reduced antibody titres after the first vaccination compared with HC, but there was no difference after the second dose. While disease modifying anti-rheumatic drug (DMARD) monotherapy did not affect antibody levels, seroconversion rates as well as titre levels were reduced in patients receiving a combination of DMARDs compared with HC.
Conclusions Patients with inflammatory joint diseases under DMARD therapy show impaired humoral responses to the first vaccine dose but excellent final responses to vaccination with mRNA vaccines. Therefore, the full course of two immunisations is necessary for efficient vaccination responses in patients with inflammatory arthritis under DMARD therapy.
- arthritis
- COVID-19
- vaccination
Data availability statement
Data are available upon reasonable request. Not applicable.
This article is made freely available for personal use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What is already known about this subject?
Some patients with inflammatory arthritis treated with specific immunomodulatory drugs might be at risk for severe COVID-19 infection. Immunisation is therefore important to prevent disease. However, immunomodulatory therapies might interfere with successful immunisation. It is therefore important to develop vaccinations strategies for these patients.
What does this study add?
The response of patients with inflammatory arthritis treated with immunomodulatory therapies to the first vaccination with messenger RNA vaccines is impaired compared with a healthy control (HC) group. However, after the second dose of the vaccine, patients with inflammatory arthritis mount antibody responses indistinguishable from HC.
How might this impact on clinical practice or future developments?
These data suggest that the second dose of the primary vaccine series are critical for patients with inflammatory arthritis to develop a full vaccination response. Assessment of the vaccination response is not possible after the first vaccination. Moreover, non-pharmaceutical protective measures are mandatory until completion of the full vaccination schedule in these patients.
Introduction
Infectious diseases are a major issue in medicine, as illustrated by the dramatic events of the current COVID-19 pandemic. Of particular concern are patients with a compromised immune system, including those suffering from immune-mediated diseases. In addition to an altered immune system as part of their underlying disease, these patients are often treated with immunomodulating therapies. Vaccinations are of paramount importance to reduce the morbidity of infectious diseases. Immunocompromised patients are of particular concern with regards to vaccination responses, as their disease or treatment might interfere with vaccine efficiency, as it was shown in various instances for vaccines against influenza, tetanus toxoid or pneumococcal antigens.1–3
During the COVID-19 pandemic, vaccination became one of the fundamental cornerstones of the fight against this disease, and highly efficient vaccines have been developed and licensed at phenomenal speed.4–7 The European League Against Rheumatism (EULAR) and the American College of Rheumatology (ACR) recommend vaccination in all patients with rheumatological diseases, even as there is currently insufficient data to formulate data-driven recommendations for vaccination strategies for different diseases or for patients receiving specific immunomodulatory therapies.8 9 Therefore, data on the efficacy and safety of COVID-19 vaccines in patients with immune-mediated diseases are needed. There have been first reports on this topic, and, not surprisingly, vaccination efficiency has been demonstrated to be reduced as compared with the general population, in particular for patients receiving B-cell depleting therapies.10 11 Methotrexate and glucocorticoids also have been shown to hamper immunogenicity of SARS-CoV-2 vaccines, with surprisingly little effects of targeted anti-cytokine treatments, often analysed only after one immunisation/one time point.12–18 However, the kinetics of the humoral response in patients with inflammatory joint diseases treated with immunomodulatory drugs have not been analysed yet.
Here we report the response of patients with rheumatoid arthritis (RA) and seronegative spondyloarthritis (SpA) to vaccination with messenger RNA (mRNA) vaccines after the first and the second dose. We show that in patients with inflammatory joint diseases under immunomodulatory therapy, excluding those who are treated with B-cell depleting agents, vaccination responses are very efficient, with a seroconversion rate of 100% after two vaccinations, but only 50%–60% after the first vaccination. These data highlight the need for a second immunisation especially in patients with inflammatory joint diseases to obtain a sufficient serological vaccine response.
Materials and methods
Patients
Patients with clinical diagnosis of established RA or SpA (including psoriatic arthritis and peripheral and axial SpA), respectively, followed routinely at our outpatient clinic were enrolled. All patients were vaccinated twice with an mRNA vaccine. Serum samples were stored at the Biobank of the Medical University of Vienna, a centralised facility for the preparation and storage of biomaterial with certified quality management (ISO 9001:2015).19 Antibodies against the receptor-binding domain and the nucleocapsid protein were determined.
Individuals without known inflammatory rheumatic disease and no current intake of any immunomodulatory therapy including glucocorticoids who were vaccinated twice with an mRNA vaccine served as healthy controls (HC). Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Anti-SARS-CoV-2 testing: The Elecsys Anti-SARS-CoV-2 S immunoassay was used for the quantitative determination of antibodies to the receptor-binding domain of the viral spike (S) protein.20 The quantitation range is between 0.4 and 2500.0 binding antibody units (BAU)/mL. Previous SARS-CoV-2 infection was ruled out by measuring nucleocapsid-specific antibodies with the qualitative Elecsys Anti-SARS-CoV-2 assay.21 Both tests were performed on a cobas e801 analyzer (Roche Diagnostics, Rotkreuz, Switzerland) at the Department of Laboratory Medicine, Medical University of Vienna (certified acc. to ISO 9001:2015 and accredited acc. to ISO 15189:2012).
Statistical analysis
Variables are depicted as medians and IQRs or means and SD (m±SD), depending on their distribution. To investigate differences in anti-SARS-CoV-2 S protein titre between rheumatic diseases and HC, either Student’s t-test, Mann-Whitney-U test or one-way analysis of variance or Kruskal-Wallis test were used, depending on the distribution. Seroconversion rates were compared using χ2 and Fisher’s exact test. In univariate analyses, association of anti-SARS-CoV-2 S titre with patient and disease characteristics were investigated using Spearman correlation coefficient and logistic regression analyses were implemented to assess the association of relevant variables with seroconversion rates. Cross-sectional analyses were performed in the total population, longitudinal analyses only in those with two titres available. GraphPad Prism (V.9.1.0) and IBM SPSS Statistics (V.26) were used for the statistics and graphical presentation of the data.
Results
Ninety-nine patients (53 with RA and 46 with SpA) and 169 HC were included in the study. The demographic characteristics are shown in table 1. We obtained serological responses of 72 patients and 136 HC 2–3 weeks after the first immunisation (mean after 19.6 days for patients and after 18.9 days for HC) and of 89 patients 3–6 weeks after the second immunisation (mean 29.1 days for patients and mean 24.3 days for HC); 63 patients and 145 HC had data on both time points.
Characteristics of patients and controls. Age, CRP and prednisolone dose are shown as mean (±SD)
Seroconversion rates and respective antibody titres after first and second immunisation
Seroconversion rates after the first dose of an mRNA vaccine were significantly lower in our patient cohort (52.5% of the patients with RA and 54.8% of the patients with SpA) compared with the healthy control group (98%) (figure 1A). Similar results were obtained analysing patients with data on both time points (online supplemental figure 1A). Seroconversion rates were 100% in all patients after the second dose of the vaccine and in all healthy controls (figure 1A). After the first immunisation, median titre levels of antibodies directed against the spike protein of SARS-CoV-2 were significantly lower in patients with RA (median 0.61 (IQR 0–17) BAU/mL), and SpA (median 1.65 (IQR 0–55.1) BAU/mL) compared with HC (median 43.3 (IQR 14.4–191), figure 1B). However, after the second immunisation, no differences in median titre levels were observed between patients with either RA or SpA and healthy controls (median (IQR) RA 1188 (263.5–2500) BAU/mL vs SpA 1785 (410.8–2500) BAU/mL vs HC 1614 (716–2500) BAU/mL) (figure 1C).
Supplemental material
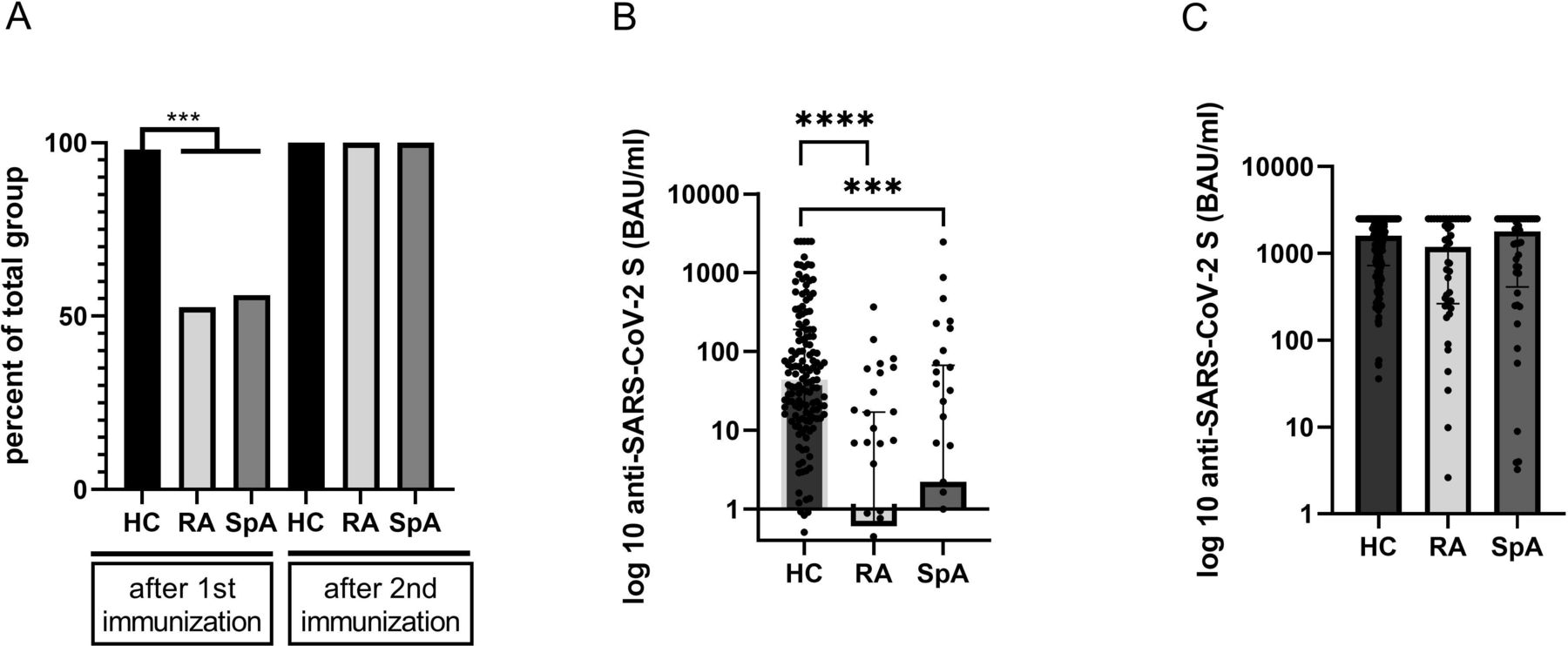
(A) Seroconversion in percent was analysed in patients with rheumatoid arthritis (RA), spondyloarthritis (SpA) and healthy controls (HC) after the first and second vaccination. (B) Analysis of anti-SARS-CoV-2 viral spike (S) titres after the first vaccination in patients with RA, SpA and HC. (C) Analysis of anti-SARS-CoV-2 S titres after the second vaccination in patients with RA, SpA and HC (**p≤0.01; ***p≤0.005, ****p≤0.001). BAU, binding antibody units.
In longitudinal analyses of patients (RA and SpA) for whom we had data both after first and second immunisation (n=63), the titres increased markedly after receiving the second vaccine dose in all patients except for one (median (IQR) change RA 1700.4 (292.8–2455.5) BAU/mL and SpA 1270 (89.6–2445.3] BAU/mL) (online supplemental figure 2).
Factors associated with seroconversion rates and antibody-titres
Analysing factors that influenced the immunisation efficiency, we found that patients receiving disease modifying anti-rheumatic drug (DMARD) combination therapy consisting of a conventional synthetic DMARD (csDMARD) and a biological/targeted synthetic DMARD (b/tsDMARD) had significantly lower rates of seroconversion after the first immunisation compared with csDMARD or b/tsDMARD monotherapy (combination therapy (n=15), 26.7% vs csDMARD (n=28), 60.7% or b/tsDMARDs mono (n=27), 61.5 %) or healthy controls (98%; figure 2A). Again, similar results were obtained when analysing patients with data on both time points (online supplemental figure 1B). Patients on combination therapies also developed significantly lower anti-SARS-CoV-2 S titres after the second immunisation compared with both patients on csDMARD monotherapy and HC. In contrast, there was no difference between patients receiving csDMARD or b/tsDMARD monotherapy and HC (median (IQR) combination 260.5 (96.4–1931.5) BAU/mL vs csDMARD 2062 (771–2500) BAU/mL vs b/tsDMARD 1292 (346.5–2500) BAU/mL vs HC 1614 (716–2500) BAU/mL; figure 2B).

(A) Seroconversion rates after the first vaccination in patients treated with csDMARD or b/tsDMARD or a combination of csDMARD and b/tsDMARD. (B) Analysis of anti-SARS-CoV-2 S titres in patients treated with csDMARD or b/tsDMARD or a combination of a csDMARD and a b/tsDMARD. (C) ORs of univariate logistic regression assessing seroconversion in patients with RA and SpA after first immunisation (csDMARD used as reference category). (**p≤0.01; ***p≤0.005). BAU, binding antibody units; b/tsDMARD, biological/targeted synthetic DMARD; csDMARD, conventional synthetic DMARD; DMARD, disease-modifying anti-rheumatic drug; HC, healthy controls.
In univariate analyses we found a moderate but significant correlation of the anti-SARS-CoV-2 S titres after the first and after the second immunisation in the patient cohort (r=0.41, p<0.01) as well as in HC (r=0.3, p<0.01). Further, we found an inverse correlation between age and anti-SARS-CoV-2 S titre after first and second vaccination in patients as well as healthy controls (online supplemental table 1). As our patient cohort is significantly older than our HC cohort, we performed age matching (±5 years) and analysed seroconversion rates and anti-SARS-CoV-2 S titres after the first immunisation as a sensitivity analysis. As in our initial analysis, we found reduced seroconversion rates in our patient cohort (54.8% (n=72) vs 95.2% in HC; n=72) and reduced anti-SARS-CoV-2 S titres (median (IQR) patient cohort compared with HC (patients 0.92 (0–28.6) BAU/mL vs HC 23.55 (6.6–132.0) BAU/mL (online supplemental figure 3A). In addition, we found no difference in age within the patient cohort between those who seroconverted after the first immunisation and those who did not (online supplemental figure 3B), suggesting that reduced vaccination responses in our patient cohort after the first immunisation is not driven by differences in age.
In an exploratory analysis, we analysed the effect of individual therapies on vaccination responses. When comparing individual treatments to the total HC group, we find that all regimens analysed (methotrexate (MTX) monotherapy (n=21 after first and n=15 after second immunisation), interleukin-17i monotherapy (n=3 after first and n=7 after second immunisation), tumour necrosis factor inhibitor (TNFi) monotherapy (n=19 after first, n=22 after second immunisation), TNFi +MTX (n=9 after first and n=10 after second immunisation), Janus kinase inhibitor +csDMARD) (n=3 after first and n=4 after second immunisation), showed reduced anti-SARS-CoV-2 S titres after the first immunisation. No differences were detected after the second immunisation (online supplemental figure 4A,B).
We did not detect an association between glucocorticoids or systemic inflammation, measured as C-reactive protein in serum and anti-SARS-CoV-2 S titre development both after the first or second immunisation, although the usage of glucocorticoids was negligible in our cohort (see table 1). In addition, we did not detect differences in anti-SARS-CoV-2 S titres after the first and after the second immunisation between patients with active arthritis (swollen joint count (SJC) >0) and patients with no active arthritis (SJC=0) (online supplemental figure 5A,B). In univariate logistic regression models OR predicting seroconversion rates after first immunisation were significant for combination therapy (OR 0.24, 95% CI 0.06 to 0.93). No significant effect of glucocorticoids, age or gender could be identified (see figure 2C, online supplemental table 2). Furthermore, we have analysed the role of age, gender, therapy and glucocorticoids in a multivariate regression model, with similar results (online supplemental figure 6).
We detected no change in disease activity after immunisation that required modification of the DMARD therapy. One patient, however, developed a swollen wrist after the first immunisation that was treated with a short course of glucocorticoids. Analysing adverse events, we found increased incidences of local reactions, fatigue and myalgia, but decreased incidences of fever, nausea, shivering and sweating in our patient cohort compared with HC (figure 3).

{kind=link}
{kind=link}
{kind=link}
Adverse events after immunisation in healthy controls (HC) and the patient cohort.
Discussion
Our study on the kinetics of the humoral response in patients with inflammatory arthritis reveals that while the immunisation efficiency after two doses of an mRNA vaccine is comparable to HC, the response to only a single dose of the vaccine is significantly reduced. While it is unclear what titre is necessary to fully protect people from COVID-19 disease, it is obvious that any measurable humoral immune response against anti-SARS-CoV-2 S protein is a prerequisite for a protective vaccination response. While we did not measure neutralising antibodies in our study, there is increasing evidence that titres of antibodies directed against the S protein measured in our study are a very good approximation of vaccine efficiency,22 and as it has been shown earlier, that titres and neutralising antibodies are highly correlated.10
The current study suggests that most patients with inflammatory joint diseases need both vaccinations to develop a substantial antibody response. It is therefore important for the management of patients with inflammatory joint diseases that non-pharmaceutical protective measures are mandatory until completion of the full vaccination schedule. Seroconversion rates after the first vaccination of our patients with arthritis are significantly below those of healthy controls, which in our hands as well as in previous reports were beyond 90% in the age groups comparable to our cohort.23 It is noteworthy that seroconversion rates in this patient group after the first vaccination are even smaller than in patients with cancer, which were reported to have a 83% response rate after the first vaccination.24 We need to highlight, that evaluation of the vaccination response in patients with inflammatory arthritis should be performed after the second vaccine dose, as seroconversion rates and titres after the first immunisation are low and do not predict successful immunisation after the full course of two doses.
It is reassuring, however, that after full immunisation with two doses of an mRNA vaccine, the seroconversion rate in our patient group was 100%. Overall, our data suggests that the response of patients with rheumatic diseases to single-dose vaccines needs to be evaluated before it can safely be recommended, and initial analyses indeed suggest reduced efficacy in patients with rheumatic diseases.25 It is important to keep in mind that we excluded patients receiving B-cell depleting therapies from our study, who were reported to have significantly reduced seroconversion rates even after full immunisation.10 13 Other studies have reported reduced immunogenicity of SARS-CoV-2 vaccines in patients on MTX,16 which might be explained by the different age of the patient groups, especially since we could demonstrate a significant inverse relation between vaccination efficiency and age in our arthritis cohort, which is younger than those reported previously, or the time point of the analysis of the serological response.26 In our cohort, we found that only patients treated with a combination of DMARDs develop reduced titres after completing the full vaccination course, but patients on csDMARD monotherapy show responses indistinguishable from healthy control. These data would argue against withholding csDMARDs after vaccinations, as currently suggested by the ACR.27 It will be important to collect data for meta-analyses, which will then be able to address more in-depths questions in the future.
Data availability statement
Data are available upon reasonable request. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval for this study was granted by the ethics committee of the Medical University of Vienna, Austria (1291/2021; 559/2005; 1073/202).
Acknowledgments
We thank all the patients who participated. We thank Sylvia Taxer and Zoltan Vass for their support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Lay summary
Disclaimer : This is a summary of a scientific article written by a medical professional (“the Original Article”). The Summary is written to assist non medically trained readers to understand general points of the Original Article. It is supplied “as is” without any warranty. You should note that the Original Article (and Summary) may not be fully relevant nor accurate as medical science is constantly changing and errors can occur. It is therefore very important that readers not rely on the content in the Summary and consult their medical professionals for all aspects of their health care and only rely on the Summary if directed to do so by their medical professional. Please view our full Website Terms and Conditions.
Copyright © 2022 BMJ Publishing Group Ltd & European League Against Rheumatism. Medical professionals may print copies for their and their patients and students non commercial use. Other individuals may print a single copy for their personal, non commercial use. For other uses please contact our Rights and Licensing Team.
Footnotes
Handling editor Gerd-Rüdiger R Burmester
ES, ST, SW and SB contributed equally.
Contributors ES, ST, HB, SW, JS, DA and SB designed the study. ST, PM, TN, FW, JS, SB, ES, HH, HR and TP analysed the data. ST, PM, ES, HH, TP, JS, HB, DA, SW and SB interpreted the results. ES, ST, PM, DA, JS and SB wrote the paper. All authors revised the manuscript and were involved in editing or quality control. SB had access to all the data, accepts full responsibility for the work and conduct of the study and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PM reports speaker fees from AbbVie, Janssen and Novartis and research grants from AbbVie, BMS, Novartis, Janssen, MSD and UCB. HH received grants from Glock Health, BlueSky Immunotherapies and Neutrolis. JS is the President of the Austrian Society of Rheumatology and Rehabilitation (unpaid position). HB received consulting fees from MSD, Pfizer, Takeda and Gilead, speaker fees from Shionogi, Pfizer and MSD, advisory boards for Valneva, MSD and Gilead. DA reports grants from AbbVie, Amgen, Lilly, Novartis, Roche, SoBi and Sanofi, other from AbbVie, Amgen, Lilly, Merck, Novartis, Pfizer, Roche and Sandoz, outside the submitted work. SB reports personal fees from AbbVie and personal fees from Novartis, outside the submitted work. ES reports support for meeting attendances from Pfizer and Bristol Myers Squibb.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.