Article Text

Abstract
Objectives To investigate whether the transient reduction in rheumatology services imposed by virus containment measures during the COVID-19 pandemic was associated with disease worsening in axial spondyloarthritis (axSpA), rheumatoid arthritis (RA) or psoriatic arthritis (PsA).
Methods Patient-reported disease activity assessed during face-to-face visits and/or via a smartphone application were compared between three periods of each 2 months duration (before, during and after the COVID-19-wave) from January to June 2020 in 666 patients with axSpA, RA and PsA in the Swiss Clinical Quality Management cohort.
Results The number of consultations dropped by 52%, whereas the number of remote assessments increased by 129%. The proportion of patients with drug non-compliance slightly increased during the pandemic, the difference reaching statistical significance in axSpA (19.9% vs 13.2% before the pandemic, p=0.003). The proportion of patients with disease flares remained stable (<15%). There was no increase in mean values of the Bath Ankylosing Disease Activity Index, the Rheumatoid Arthritis Disease Activity Index-5 and the Patient Global Assessment in patients with axSpA, RA and PsA, respectively.
Conclusion A short interruption of in-person patient–rheumatologist interactions had no major detrimental impact on the disease course of axSpA, RA and PsA as assessed by patient-reported outcomes.
- arthritis
- rheumatoid
- spondylitis
- ankylosing
- arthritis
- psoriatic
- epidemiology
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What is already known about this subject?
Partial or complete closure of rheumatology services was experienced in many countries as part of SARS-CoV-2 containment measures.
Remote consultation strategies might partly compensate for lower number of face-to-face visits to prevent a postponement of treatment decisions for inflammatory rheumatic diseases.
What does this study add?
In this real-life cohort study of patients with axial spondyloarthritis, rheumatoid arthritis and psoriatic arthritis with available patient-reported disease activity assessments during the first wave of the COVID-19 pandemic via a web-based application after a drop in face-to-face consultations no increase in disease activity could be observed.
Although the proportion of patients with medication non-compliance slightly increased during the pandemic, the proportion of patients with disease flares remained stable.
The patient population followed here used a smartphone app regularly and might be more invested in disease management. The results have to be interpreted in this light.
How might this impact on clinical practice or future developments?
The lack of a major detrimental effect of a short interruption of physical consultations on the disease course of several inflammatory rheumatic diseases informs potential future measures of public lockdown.
As patient-reported outcomes are insufficient to guide treat-to-target efforts, assessments of long-term outcomes are warranted.
Future studies are needed to confirm the usefulness of remote strategies to regularly assess patient-reported outcomes.
Introduction
The ongoing COVID-19 pandemic remains an important healthcare challenge.1 Data on the course of inflammatory rheumatic diseases during the pandemic are scarce.2 Partial or complete closure of rheumatology services was experienced in many countries as part of virus containment measures and transient lockdown of public life.3 It remains unclear, whether remote consultation strategies might partly compensate for lower numbers of face-to-face visits to prevent a postponement of treatment decisions.4 Additional factors may also potentially contribute to disease worsening during the pandemic. Some patients may choose to preventively stop immunosuppression out of fear of complications.2 Moreover, the psychological stress (anxiety about a new disease, economic pressure, less recreational opportunities and so on) encountered during the pandemic should not be underestimated.5 The aim of this study was to assess the course of self-reported disease activity and of drug adherence in patients with axial spondyloarthritis (axSpA), rheumatoid arthritis (RA) and psoriatic arthritis (PsA) before, during and after the initial COVID-19 wave in Switzerland.
Methods
Choice of disease assessments periods
The specific COVID-19 situation in Switzerland in the first 6 months of 2020 is detailed in the supplementary appendix. According to the described longitudinal course of SARS-CoV-2 infection numbers, we defined three study periods of 2 months duration each: (1) a pre-COVID-19 wave phase from 1 January to 29 February 2020; (2) a COVID-19 wave phase from 1 March to 30 April 2020 and (3) a post-COVID-19 wave phase from 1 May to 30 June 2020 (figure 1A).
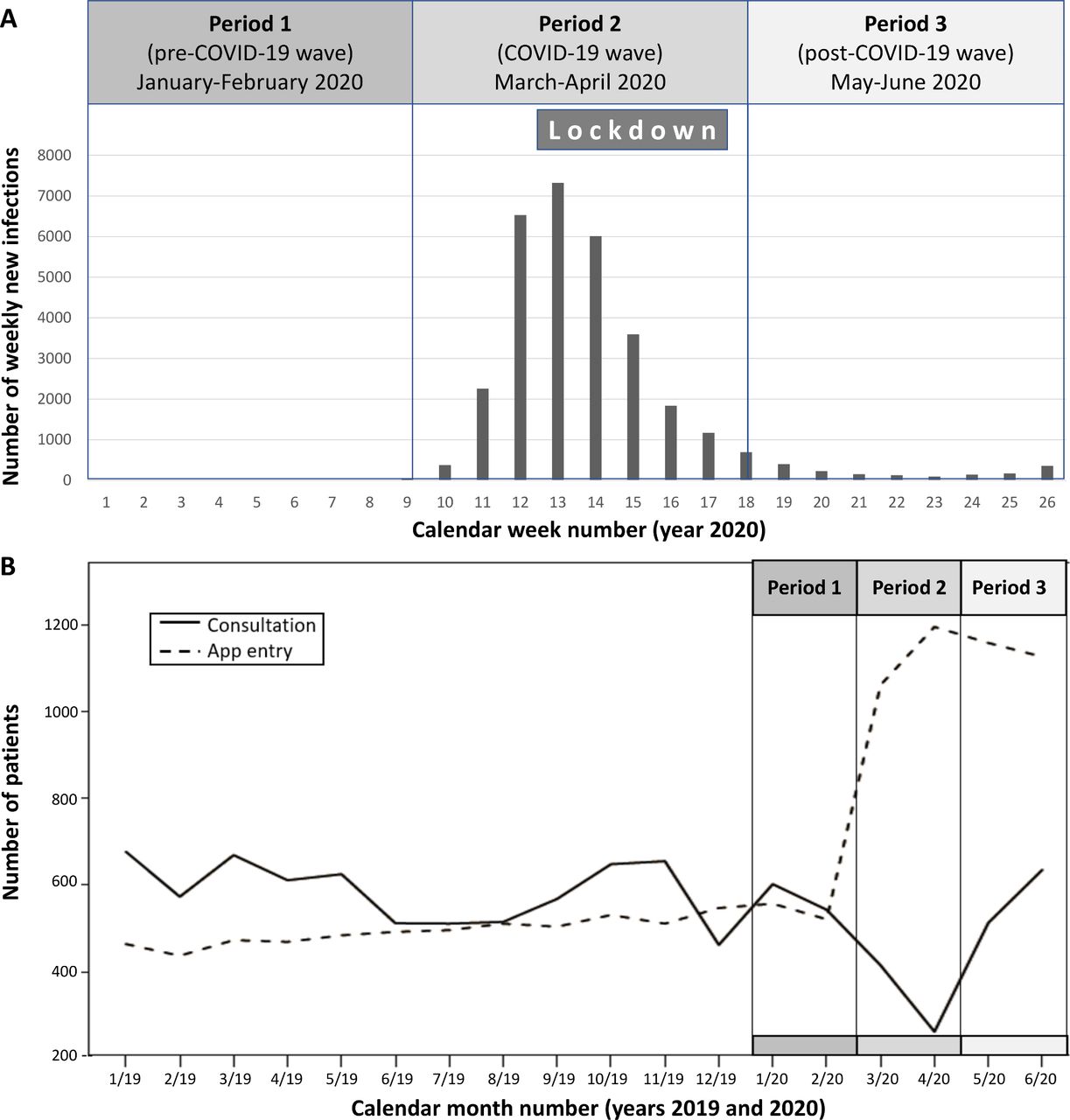
(A) Number of weekly new SARS-CoV-2 infections registered in Switzerland, defining three periods: a pre-COVID-19-wave phase from 1 January to29 February 2020; a COVID-19-wave phase from 1 March to 30 April 2020 and a post-COVID-19-wave phase from 1 May to 30 June 2020. The 5-week period of partial lockdown of public life imposed by the Swiss Federal Council is inscribed during the COVID-19-wave phase. (B) Monthly numbers of face-to-face consultations and remote app entries of patients with inflammatory rheumatic diseases followed in the Swiss Clinical Quality Management cohorts. The COVID-19-wave phases defined in (A) are indicated from January to June 2020.
Study population
Patients diagnosed as having axSpA, RA or PsA in the Swiss Clinical Quality Management (SCQM) cohort6–8 were included if at least one patient-reported disease activity measure was available in each of the study periods defined above, irrespective of whether the assessment was performed during consultations or remotely via a web-based application. All patients currently followed in SCQM, defined as patients with at least one visit during the last 18 months, served as control. The voluntary use of the app by the patients to monitor disease activity and drug compliance monthly started on 1 January 2019.9 Additional information provided to patients during the pandemic is compiled in the supplementary appendix. All patients gave informed consent prior to data collection. Ethical approval was given by the Geneva cantonal committee for research ethics (2020-01708).
Disease activity assessments
Patient-reported disease activity assessments included the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) in axSpA,10 the Rheumatoid Arthritis Disease Activity Index-5 (RADAI-5) in RA11 and the Patient Global Assessment (PGA) visual analogue scale for disease activity in PsA,12 both during visits and for app entries. Disease activity measures were investigated for each 2-month period as previously defined. A clinically important worsening in individual patients from period 1 to 2 and from period 2 to 3 was defined as follows: BASDAI showed increase of 2 points in axSpA; RADAI-5 showed increase of 1.4 points in RA11 and PGA showed increase of 1.2 points in PsA.12
Adherence to treatment
All other answers except ‘yes‘ to the question ‘Do you take the following medication regularly?’ in the monthly app questionnaire were considered as non-compliance with prescribed medication (online supplemental information).
Supplemental material
Statistical analyses
McNemar’s test was used to compare the proportions of patients with drug non-compliance or experiencing a disease flare and the paired t-test was used to compare disease activity scores between two subsequent periods.
Results
Number of visits and of APP entries over time
The monthly number of patients consulting rheumatologists and the monthly number of patients with app entries for 2019 and the three periods of interest in 2020 are depicted in figure 1B. The number of visits declined by 52% with the implementation of virus containment arrangements from n=543 in February to n=262 in April 2020. Given measures taken to motivate patients to use the app to enter disease activity and their willingness to contribute to shared decision making and research, this was paralleled by an increase in app entries (from 521 to 1195).
Adherence to DMARD therapy
Baseline characteristics of 287 axSpA, 248 RA and 131 PsA patients fulfilling the inclusion criteria are shown in table 1. The patients in the individual disease categories were comparable with the respective group of all SCQM patients currently followed in SCQM, with the exception of the subset of patients with RA, which was younger and had a slightly lower disease activity score at inclusion (online supplemental table S1). The low number of face-to-face visits precluded a comparison between patients with clinical visits and remote data entries. The majority of patients (>70%) were treated with a biological disease-modifying antirheumatic drug (bDMARD) at the study start with the proportion of patients on synthetic DMARDs depending on the underlying disease (table 1). The prepandemic proportion of patients with non-compliance to the prescribed medication was around 15%. There was a slight increase in the number of non-adherent patients during the pandemic, the difference to the pre-pandemic numbers reaching statistical significance in axSpA (table 1). Adherence returned to prepandemic levels in the post-COVID-19 phase.
Baseline characteristics of patients, mean disease activity scores as well as number of disease flares and of drug non-compliance cases in the respective 2 months before, during and after the COVID-19 wave in Switzerland
Course of disease and number of disease flares
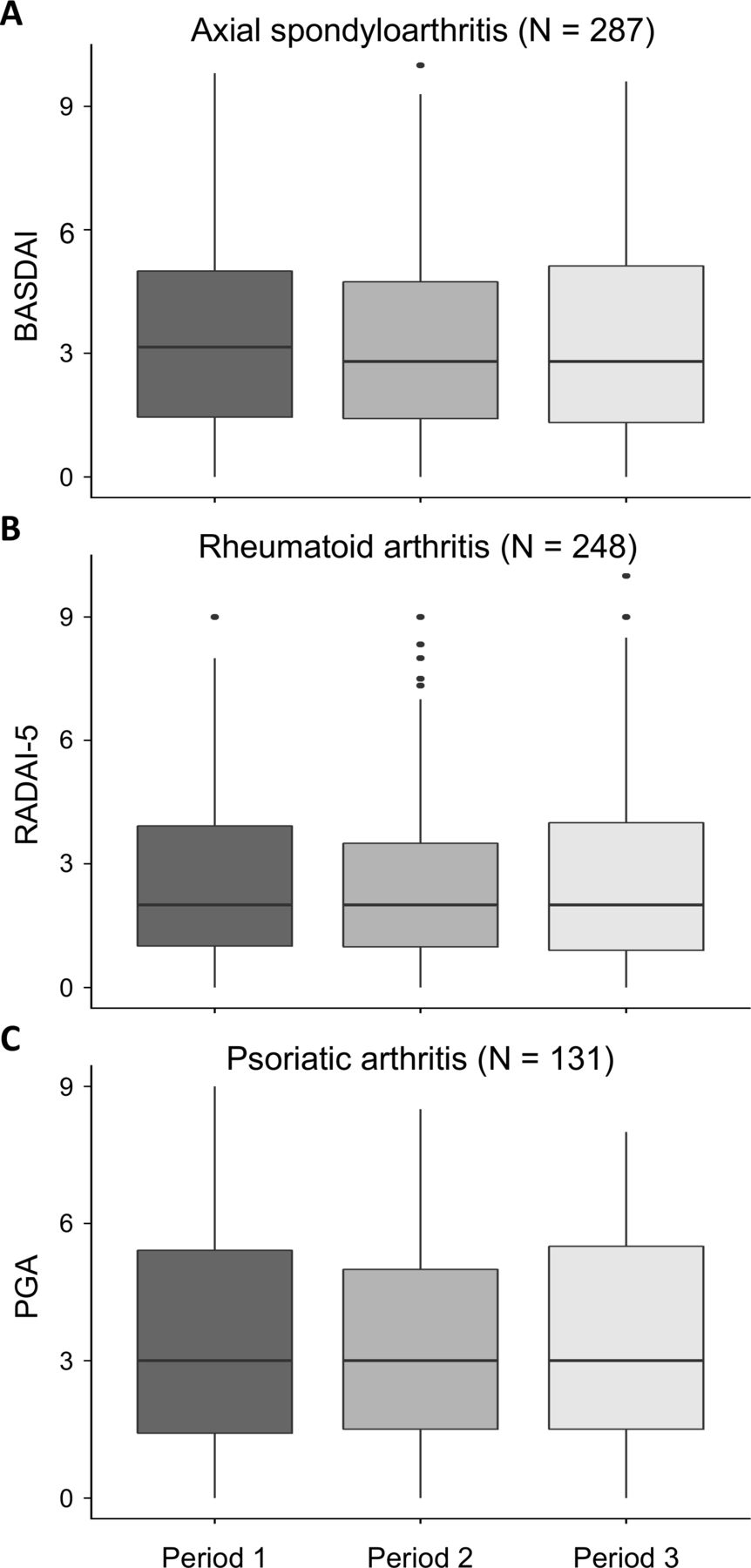
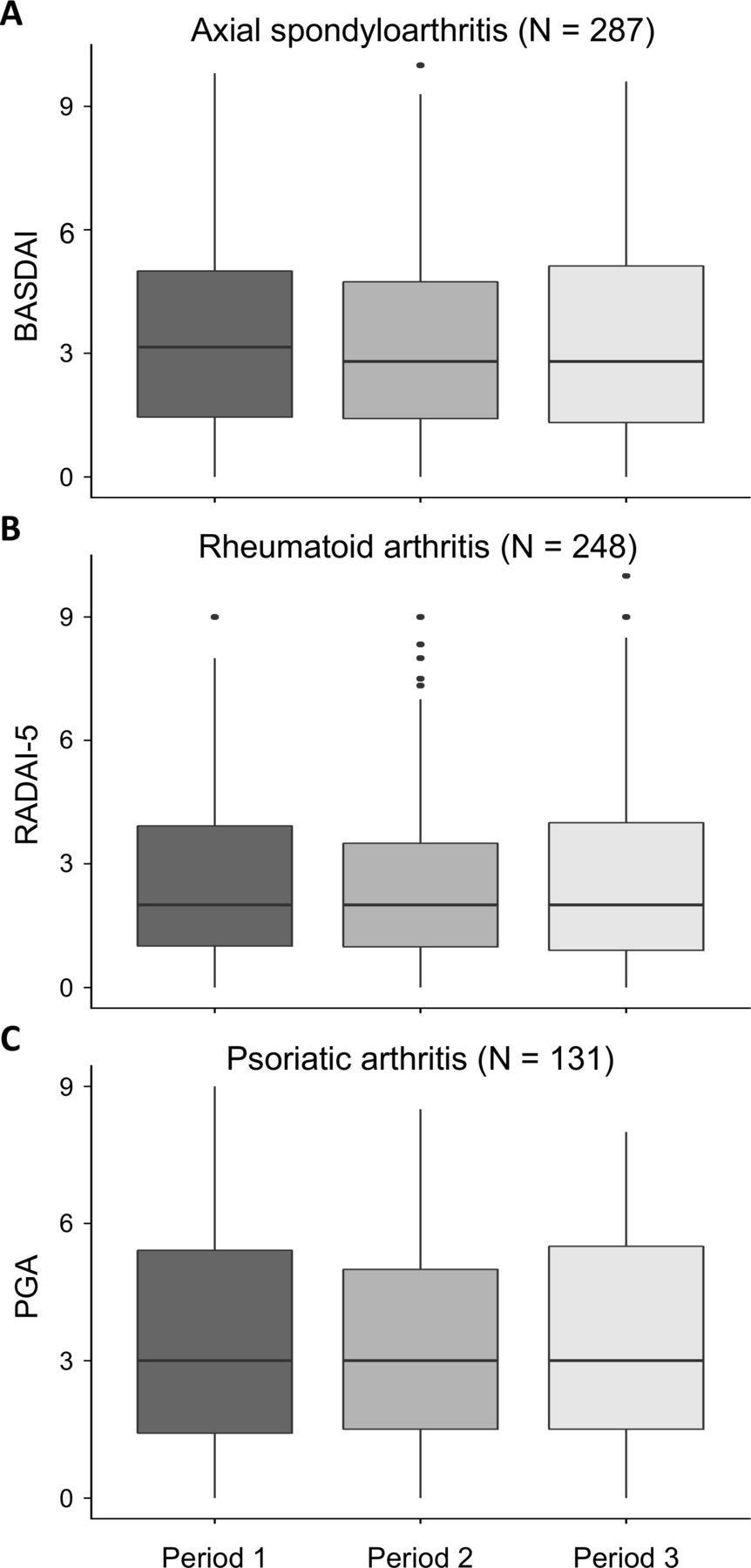
Patient-reported disease activity outcomes were stable over the first 6 months of 2020 (figure 2 and table 1), with a slight decrease during the pandemic wave, reaching statistical significance in axSpA (mean (SD) BASDAI 3.40 (2.23) before the pandemic and 3.23 (2.25) during the pandemic, p=0.02). To put the disease activity scores in a broader perspective, monthly median values from all SCQM patients are shown separately for physical consultations and remote app entries from January 2019 to June 2020 in the online supplemental figures S1 and S2. The proportion of patients with a disease flare during the pandemic wave was <15% for all three diseases (table 1) and no statistical significance could be found when compared with the proportion with disease worsening in the pre-COVID-19 phase.
{kind=link}
{kind=link}
Disease activity values for the pre-COVID-19-wave phase (period 1), the COVID-19-wave phase (period 2) and the post-COVID-19-wave phase (period 3) in patients with axial spondyloarthritis (A), rheumatoid arthritis (B) and psoriatic arthritis (C). The horizontal line in the boxes represents the median value. BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; PGA, Patient Global Assessment of disease activity; RADAI-5, Rheumatoid Arthritis Disease Activity Index-5.
Discussion
A web-based smartphone application had been implemented within the Swiss registry long before the current pandemic and allowed us to follow the course of inflammatory arthritides over the whole initial COVID-19 wave. We noted an acute drop in clinical encounters that was paralleled by an increase in app entries. Our study demonstrates that disease activity as assessed by the BASDAI in axSpA, the RADAI-5 in RA and PGA in PsA remained stable and even slightly decreased over the duration of the pandemic wave at the population level. Moreover, a disease flare occurred in <15% of patients, not statistically different from the pre-COVID-19 phase. Although cut-offs for a clinically important worsening exist for the patient-reported outcomes used here for RA and PsA, there is no consensus for a BASDAI cut-off in this regard. We have used a worsening by two points as its performance was comparable with the defined Ankylosing Spondylitis Disease Activity Score cut-off against the external standard ‘patient-worsening’.13 Patient-reported worsening was investigated in a recent observational study in patients with RA and patients with axSpA and was experienced by 29% of patients over a duration of 3 months.14
The results presented here can only be interpreted in the context of a rather short first COVID-19 pandemic wave as encountered in Switzerland. A recent international survey in 35 EULAR (European League Against Rheumatism) countries found that a partial closure of rheumatology services of 5–8 weeks duration during the COVID-19 pandemic was reported by 81% of 1428 respondents,3 underscoring the representativeness of our data.
Current guidelines based on preliminary data do not recommend the preventive cessation of immunosuppressive medication in the absence of infection.15 16 To continue or to stop medication in individual situations during the COVID-19 pandemic ultimately is part of a shared decision-making process between the patient and his rheumatologist. We have therefore focused on patient-reported non-adherence to the medication entered in the database by the rheumatologist and not on actual drug changes. We hypothesise that the duration of the pandemic was too short for the documented transient decrease in drug adherence to be reflected in an increase in disease flares.
Regular assessments of disease activity is a key component of the treat-to-target principle in the management of rheumatic diseases. In addition to the voluntary reporting of disease activity by the patients, we assume an important increase in the number of remote patient–physician interactions (email and phone calls) during the pandemic. Although their actual figures remain unknown, the influence of telemedicine on the outcome presented here should not be underestimated.4 We acknowledge the fact that patient-reported measures cannot replace clinical examination. Recent data have suggested that their exclusive use might be insufficient to guide treat-to-target efforts.17 In the absence of alternatives in the context of suspended visits to physicians, their use is however warranted.
An important limitation of this work is that we could only evaluate patients with regular assessments of disease activity, which was mostly based on remote data entries during the pandemic. This subset using the smartphone app is probably more invested in disease management and the non-compliance figures might be under-represented.
In conclusion, a temporary interruption of in person consultations during the COVID-19 pandemic had no major detrimental impact on the disease course of patients with inflammatory rheumatic diseases as assessed through patient-reported outcomes.
Acknowledgments
The authors thank all patients and their rheumatologists for participation and the entire SCQM staff for data management and support. A list of rheumatology private practices and hospitals that are contributing to the SCQM registries can be found on: http://www.scqm.ch/institutions.
References
Supplementary materials
Lay summary
Disclaimer : This is a summary of a scientific article written by a medical professional (“the Original Article”). The Summary is written to assist non medically trained readers to understand general points of the Original Article. It is supplied “as is” without any warranty. You should note that the Original Article (and Summary) may not be fully relevant nor accurate as medical science is constantly changing and errors can occur. It is therefore very important that readers not rely on the content in the Summary and consult their medical professionals for all aspects of their health care and only rely on the Summary if directed to do so by their medical professional. Please view our full Website Terms and Conditions. http://www.bmj.com/company/legal-information/
Copyright © 2021 BMJ Publishing Group Ltd & European League Against Rheumatism. Medical professionals may print copies for their and their patients and students non commercial use. Other individuals may print a single copy for their personal, non commercial use. For other uses please contact our Rights and Licensing Team.
Footnotes
Handling editor Josef S Smolen
AS and AF contributed equally.
Contributors Study conception and design: AC, AF, AM, AR-R, AS, BM, DD, DK, EP, IvL, OD, RB. Acquisition of data: AC, KB, RM, BM, AR-R, MA, DD, DK, OD and AF. Statistical analysis: EP and AS. All authors contributed to the interpretation of the data. AC wrote the manuscript. All authors critically revised the manuscript. All authors revised and approved the final manuscript to be published.
Funding The SCQM Foundation is supported by the Swiss Society of Rheumatology and by AbbVie, Amgen, Gilead, iQone, Lilly, Merck Sharp & Dohme, Novartis, Pfizer, Roche, Samsung Bioepis, Sandoz, Sanofi Genzyme, UCB.
Competing interests AC reports personal fees from Abbvie, Celgene, Eli-Lilly, Merck Sharp & Dohme, Novartis and Pfizer, outside the submitted work. OD reports personal fees from Abbvie, Amgen, Lilly and Pfizer, outside the submitted work. RM reports personal fees from Gilead, Eli-Lilly and Abbvie, outside the submitted work.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Ethics approval The study was approved by the Ethics Committee of the Canton of Geneva and written informed consent was obtained from all patients.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.