Article Text

Abstract
Objective There are limited data on long-term comorbidities and mortality among patients with familial Mediterranean fever (FMF). Our objective was to evaluate comorbidities and death rates among individuals with FMF.
Methods We studied a nationwide, population-based, retrospective cohort of 1225 individuals with FMF (59% men) in a database of 1 244 350 adolescents (16–20 years of age) medically evaluated for military service between 1973 and 1997. This cohort was linked with the national mortality, cancer and end-stage renal disease (ESRD) registries in Israel. Study outcomes were all-cause mortality, occurrence of ESRD and malignancy by the age of 50 years.
Results During 30 years of follow-up, death rates were 8.73/104 versus 4.32/104 person-years in the FMF and control groups, respectively (p=0.002). In a multivariable analysis adjusted for age, birth year, socio-economic status, education, ethnicity and body mass index, FMF was associated with increased mortality in men (HR=1.705 (95% CI 1.059 to 2.745), p=0.028) and women (HR=2.48 (1.032 to 5.992), p=0.042). Renal amyloidosis accounted for 35% and 60% of deaths in men and women, respectively. FMF was not associated with an increased incidence of cancer.
Conclusions FMF is associated with increased all-cause mortality that is likely attributed to reduced colchicine compliance or responsiveness. Individuals with FMF do not have an increased incidence of cancer. These results support the awareness among medical community to decrease the higher than average mortality rate among participants with FMF.
- Amyloidosis
- Familial Mediterranean Fever
- Epidemiology
Statistics from Altmetric.com
Introduction
Familial Mediterranean fever (FMF) is a genetic disease associated with mutations in MEditerrenean FeVer (MEFV), a gene that encodes the pyrin protein, and is characterised by recurrent episodes of fever and serositis.1 It is most prevalent among Turkish, Armenian, Arab and non-Ashkenazi Jewish populations, and when left untreated, results in renal amyloidosis before the age of 40 years in approximately 60% of cases.2
To date, insufficient data are available on the death rates of individuals with FMF compared to the general population. Prior to the colchicine era, excess mortality was seen in FMF patients and was attributed to the development of renal amyloidosis.3 In the sole report investigating mortality in a cohort of 587 Turkish FMF patients, the risk of death was found to be comparable to that of the general population.4 In parallel, the association between FMF and common risk factors for death such as cancer are not clear. While pyrin is suggested to play a role in apoptosis of leukocytes, no clear association has ever been demonstrated between MEFV or its mutations and cancer, limiting such speculations to anecdotal case reports.5 ,6
This nationwide cohort study was conducted to investigate the risk of death among individuals with FMF. To further explore potential mortality-related aetiologies, the secondary goal was to assess the risk for common comorbid conditions including end-stage renal disease (ESRD) and cancer.
Methods
Study population
The study group consisted of all individuals with FMF among military service recruits from 1973 to 1997; recruits without a diagnosis of FMF were assigned to the control group. One year before conscription into military service, all eligible Israeli adolescents undergo a medical examination to assess their health status, which includes a review of medical records obtained from their primary care physician, a medical history, a physical examination (including routine urinalysis), and when indicated, referral for further assessment. Inclusion criteria for the current study were age 16–20 years at the time of medical examination. The Israel Defense Forces (IDF) excludes from military draft candidates with severe illness including any degree of renal failure. Subjects who were exempt from military service due to any pre-existing medical condition, had a follow-up of less than 5 years, or died due to trauma during military service were excluded from the analysis. A total of 1 244 350 adolescents (736 308 men) of whom 1225 (approximately 0.1%) had a diagnosis of FMF (722 men) were included in the current study. The diagnosis of FMF was based on a documented diagnosis by a rheumatologist. The institutional review board of the IDF approved the study and waived the requirement for informed consent on the basis of strict maintenance of participants’ anonymity.
Study design, follow-up and outcome variables
The design of the current study is shown in figure 1. The primary outcome of the study was all-cause mortality. The Israeli Ministry of the Interior routinely reports the deaths of Israeli citizens previously enrolled for the medical examination to the IDF. The cause of death is not reported and was not available for analysis. Follow-up ended at either the time of the reported death, age of 50 years or 30 June 2011, whichever came first. Secondary outcomes included the occurrence of any type of cancer and ESRD.
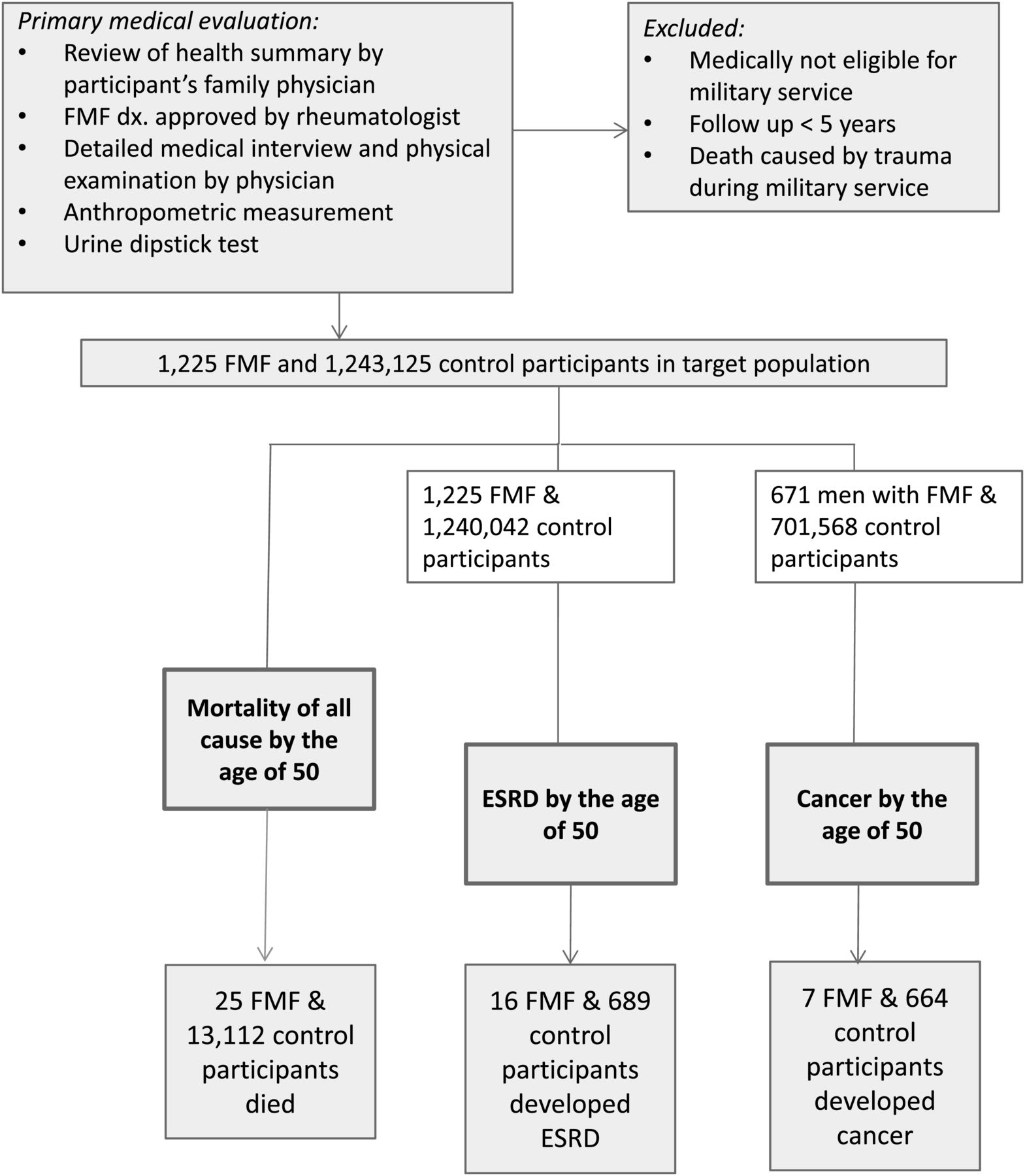
Participant assessment, designation and outcomes. ESRD, end-stage renal disease.
The Israel National Cancer Registry
The Israel National Cancer Registry (INCR) has been linked to the current database as described previously.7–9 The INCR is a population-based registry of all types of cancer. It was set up 50 years ago, with reporting becoming mandatory in 1982, and has a coverage rate of over 95%. The INCR data include the date of cancer diagnosis, the site affected and histological description of the tumour. In the current work only the data of men were available to us during the study period. Follow-up ended at the time of the reported cancer, death, age of 50 years or 31 December 2006, whichever came first.
The ESRD registry
The Israeli ESRD database is a national administrative registry maintained by the Israel Center of Disease Control (ICDC) of the Israeli Ministry of Health. It contains information on patients receiving any form of renal replacement therapy (haemodialysis, peritoneal dialysis or kidney transplantation). All nephrology dialysis units in Israel routinely report to the Ministry of Health regarding every new patient receiving renal replacement therapy and any change in treatment modality. The database also includes the primary diagnosis and the initial modality of renal replacement therapy, as well as the date when dialysis was initiated. The current study cohort was linked to the Israeli ESRD registry using the identification number given to all Israeli citizens at the time of birth or immigration in a similar manner to previous reports.10 ,11 Follow-up ended at the time of reported ESRD, death, age of 50 years or 31 May 2010, whichever came first.
Study variables and statistical analysis
Age at enrolment and body mass index (BMI) were taken as continuous variables in multivariable models. Socio-economic status (SES) based on place of residence was obtained from records of the Israeli Ministry of the Interior and was classified as low, intermediate or high, as reported previously.12 Education was divided into low and high levels below or above 10 full years of school education, respectively. Countries of origin (classified by the father's or grandfather's country of birth) were grouped into five geographical areas: former USSR countries, Asia (non-USSR), North Africa, Western (comprised of non-USSR Europe, North and South America, South Africa, Australia and New Zealand) and Israel. The participant's birth country was categorised according to the same five areas. Proteinuria (defined as dipstick levels of at least +1 protein) and haematuria (defined as five or more red blood cells per high-power field for urine specimens) were merged in a dichotomous ‘yes/no’ variable. Reported values are presented as mean±SD, unless noted otherwise. Categorical variables were compared between FMF and control participants with the χ2 test. The t test was used to test mean differences in continuous variables between FMF participants and controls. Trends in SES were calculated by linear-by-linear association. Cox proportional hazards regression models (univariable and multivariable) were used to test the association between FMF and time to death or occurrence of cancer. Log minus log plots for each variable were inspected to verify the assumption of proportionality of the hazards. Simple contrasts were used to compare each group to the reference group in case of categorical variables. Kaplan–Meier survival analysis was performed among men with FMF according to enrolment year (1973–1986 vs 1987–1997) and the log rank test was used for comparisons between cohorts. Analyses were performed with IBM SPSS V.19.
Results
Characteristics of study participants
The baseline characteristics of the FMF and control participants are presented in table 1. A higher proportion of the FMF men and women had a North African origin (70.9% and 68.3%, respectively) compared to the control group (27.4% and 24.0%, respectively). Participants with FMF generally had a lower SES and a lower level of education. When the control and FMF groups were restricted to those of North African and Asian origin, there were no differences in the level of education in either gender, but differences in SES persisted.
Baseline characteristics of the cohort population
FMF is associated with an increased risk for all-cause mortality
Among men, 20 (2.77%) deaths in the FMF group and 10 746 (1.36%) deaths in the control group were reported during a mean follow-up of 23.7±6.5 and 24.7±6.6 years, respectively (table 2). In the female group, five (0.99%) and 2366 (0.46%) deaths were reported in the FMF and control groups during a mean follow-up of 22.9±6.0 and 24.0±6.4 years, respectively.
Cox proportional univariable and multivariable analysis linking FMF and mortality
A multivariable model adjusted for age at enrolment, birth year, education, SES, birth country, origin and BMI yielded significantly higher HRs for death among FMF participants, which were 1.72 for men (95% CI 1.068 to 2.78) and 2.48 for women (95% CI 1.032 to 5.992) compared to the control population. The pattern of the survival function showed an increasing difference over time between the FMF and control groups (figure 2A,B). Cumulative survival was not significantly different between 1973–1986 and 1987–1997 (figure 2C; log rank p=0.712) or when the analysis was restricted to men only (p=0.843). Furthermore, when enrolment year was taken as a continuous variable in a Cox proportional hazards regression model, the HR was 1.014 (95% CI 0.933 to 1.102, p=0.744). No deaths were reported among FMF men or women with haematuria and/or proteinuria during the entire follow-up period. Death rates were similar between FMF participants of different origin.

{kind=link}
{kind=link}
Association between familial Mediterranean fever (FMF) and mortality. (A,B) Survival analysis of adults with and without FMF during 30 years of follow-up (continuous and dashed lines, respectively). Data for men (A) and women (B) cover 1 244 350 control participants and 1225 participants diagnosed with FMF. During a cumulative follow-up of 30 371 341 person-years, 13 112 and 25 deaths occurred in the control and FMF groups, respectively. Cox functions in both genders were adjusted for age at enrolment, birth year, education, socio-economic status, birth country and body mass index. (C) Kaplan–Meier curves for deaths among men and women with FMF by year of enrolment.
ESRD and mortality
Sixteen FMF individuals (13 men and 3 women) developed ESRD out of a total 705 (552 men) participants who were reported to the ESRD registry during the follow-up period. Renal amyloidosis was the most common cause of renal failure in FMF participants, in 92% of men and 100% of women, with a mean age of onset of ESRD before 40 years for both genders (39.2±5.4 and 36.9±1.2 years, respectively). Renal amyloidosis was significantly higher in the FMF group than in non-FMF ESRD participants, where its frequency was 1.53% in men and 1.71% in women with ESRD (p<0.001). All three women with renal amyloidosis died. Seven of 12 men who developed amyloidosis-associated ESRD died during the study period. North African origin was associated with 100% and 67% of deaths due to renal amyloidosis in men and women with FMF, respectively.
Cancer incidence
We assessed the incidence of malignancy before the age of 50 years in the group of men. During the research period, 7/671 FMF participants and 664/701 568 control participants developed cancer. Univariable analysis yielded HRs for the occurrence of malignant disease of any type in the FMF group that were not statistically different from those of the control group (HR=1.408, 95% CI 0.67 to 2.95, p=0.366). Of the seven cases of cancer among FMF participants, three died and none developed ESRD during the study period. Cancer types for FMF participants are listed in table 3.
Cancer cases among men with familial Mediterranean fever
Discussion
This nationwide study explores the rate of all-cause mortality during adulthood and its association with common risk factors for death among participants with FMF using four national databases. We have shown that participants with FMF are at a higher risk for death from all causes during adulthood, with renal amyloidosis being a primary comorbidity. The occurrence of cancer in men with FMF was comparable to that of the general population.
Mortality and renal amyloidosis
Early mortality data in untreated FMF participants showed that the onset of renal amyloidosis before the age of 40 years was the primary cause of death.2 ,3 In the sole mortality report since colchicine was introduced, that was based on 14 deaths (of which nine were women) with a mean follow-up of 6 years, the death rates of Turkish FMF subjects was comparable to the rates reported among the general population.4 Our data contradict these outcomes with a mean follow-up exceeding 24 years. Apart from the longer follow-up, at least three additional factors may account for the different conclusion concerning death rates among FMF participants: the selection of relatively healthy participants at enrolment, accurate definition of a parallel control group (rather than comparison with a general mortality table) and a multivariable model adjusted for well-recognised confounders of mortality including age, birth year, education, SES, birth country, country of origin and BMI.
Crude mortality data from the Israel Central Bureau of Statistics showed an average annual death rate in the general population in the age range 25–49 years between 1975 and 2009 of 11.71/104 and 6.61/104 for men and women, respectively. These values are comparable to those of FMF participants, but double the rates of the study control group (table 2), likely reflecting the exclusion of individuals with significant comorbidities that would medically disqualify them from military service.
The finding that 35% and 60% of deaths were associated with renal amyloidosis in men and women, respectively, is consistent with that of Akar et al4 who reported renal amyloidosis in 57% of deaths, of which approximately 90% occurred before the age of 50 years. Our data are concordant with the findings of Gershoni-Baruch et al13 who demonstrated that female patients have higher risk for arthritic attacks but that male patients more frequently develop amyloidosis in a 2 : 1 ratio. Cazeneuve et al14 reported that males had a fourfold higher rate of developing renal amyloidosis than females in a homogeneous population of 137 Armenian patients. However, these discrepancies may result from different patterns of compliance and adherence to colchicine therapy which is often culturally related.15
The similarity between the survival curves of men during 1973–1986 (the first 12 years after colchicine was introduced as a treatment for FMF) and 1987–1997 (figure 2C) indicates a component of mortality that is independent of colchicine availability. Low availability of colchicine is unlikely to underlie this component, as the prevalence of renal amyloidosis in Israel is threefold lower among FMF participants than in Turkey and Arab countries where FMF is relatively frequent.16 This finding correlates with a higher standard of medical care (also reflected by a lower infant death rate) in Israel than in these countries, thereby inferring good availability of colchicine in Israel.16
Inadequate response to colchicine treatment was reported in up to 30% of FMF participants, being more prevalent among M694V homozygotes.17 ,18 In the absence of other therapeutic alternatives, the more severe disease that is associated with the latter mutation prompts escalation of colchicine dosage. However, with the development of side effects, subsequent lowering of colchicine dosage may result in suboptimal treatment. In agreement with this, colchicine blood levels of colchicine non-responders were comparable to those of colchicine responders.19
Compliance with treatment is also a major issue in FMF patients with amyloidosis. Zemer et al20 reported that three of four patients who developed amyloidosis in a cohort of 1000 colchicine-treated FMF patients admitted non-compliance with treatment.20 In a recent study investigating risk factors for the development of amyloidosis in a group of Israeli kidney transplanted FMF patients with amyloidosis, non-compliance with colchicine treatment was disclosed by 50% of amyloidosis patients compared to 2% of the FMF control population.21 These findings emphasise that renal amyloidosis remains a devastating complication even in the colchicine era in a country where FMF-associated amyloidosis is low. Taken together, these data suggest that higher mortality is not necessarily an inherent feature of FMF but more likely associated with responsiveness to colchicine or low compliance with treatment.
Mortality due to malignancy
Pyrin was suggested as a modulator in myeloid differentiation5 and has been linked with several haematological malignancies.6 ,22 In addition, a series of lung mesothelioma cases without prior asbestos exposure raised the question of the contribution of chronic inflammation to the development of malignancy.23 However, in our study, only seven cases in the male cohort developed a malignancy, with an overall incidence of a single case of malignancy in adulthood for every 2443 person-years, similar to the rate of the control group. To our knowledge, this is the first published study that tested the association between FMF and the occurrence of cancer, suggesting that the latter is not a principal contributor to the excess mortality seen in FMF participants. Further studies are needed to extend this conclusion to women with FMF, as well as to older FMF individuals.
Several limitations of this study warrant consideration. During the study period, the diagnosis of FMF was based solely on clinical manifestations (as is current practice24) with no data on underlying genetics. It excluded participants with altered renal function at enrolment. However, these potentially false–positive results and pre-selection criteria would have only caused the association between FMF and study outcomes to be underestimated. The exact cause of death was unavailable to us, thus limiting identification of a specific comorbidity. The rates of colchicine prescription filling and dispensing were also not available, limiting our ability to accurately define the exact role of colchicine versus FMF per se in mortality or the occurrence of cancer. The clinical course of FMF participants was not available, thereby limiting our ability to accurately define markers and factors that could have affected study outcomes. The strengths of this study include its very large population and the use of highly reliable national databases.
In conclusion, renal amyloidosis is strongly associated with excess mortality in individuals with FMF. These findings warrant the ongoing awareness of FMF among the medical community to decrease the higher than average mortality rate among participants with this disease.
Acknowledgments
We thank Pinchas Borenstein's family for their unconditioned support of the Talpiot Medical Leadership programme. We thank Dr Solomon A Graf for critical reading and helpful comments on earlier versions of this manuscript and Mrs Yulia Bludnikov for assistance with statistical analysis.
References
Footnotes
-
Handling editor Tore K Kvien
-
Contributors GT: study concept and design, acquisition and interpretation of the data, research methods and statistical analyses, and drafting of the manuscript; AL, AV and HA: study concept and design, interpretation of the data, and critical revision of the manuscript for important intellectual content; AA, AS, IB-Z, AT, TS and EG: study concept and design and critical revision of the manuscript for important intellectual content; ED: acquisition and interpretation of the data, research methods and statistical analyses; DT: acquisition of the data; and MB: study concept and design.
-
Competing interests None.
-
Funding GT, AV, AT and IB-Z were partially supported by the Pinchas Borenstein Talpiot Medical Leadership Program of Sheba Medical Center.
-
Ethics approval The institutional review board of the Israel Defense Forces approved this study.
-
Provenance and peer review Not commissioned; externally peer reviewed.