Article Text

Abstract
Objectives To update a previous systematic review assessing the efficacy of conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) in rheumatoid arthritis (RA).
Methods Two systematic reviews of the literature using PubMed, Embase and the Cochrane library were performed from 2009 until January 2013 to assess the efficacy of csDMARDs (as monotherapy or combination therapy) in adults with RA, and the efficacy of glucocorticoids in early RA. A third systematic review was performed until March 2013 to assess the efficacy of tofacitinib by meta-analysis.
Results For glucocorticoids, of 222 hits, five publications relating to four new trials were analysed for efficacy, confirming that initial treatment of RA with low-dose prednisone plus methotrexate (MTX) results in better clinical and structural outcomes at 1 and 2 years than treatment with MTX alone. For csDMARDs, of 498 studies, only two new studies were randomised controlled trials comparing MTX monotherapy with MTX in combination with another csDMARD without differences in glucocorticoid usage. Using tight control principles, clinical outcomes were no better with immediate triple therapy than with ‘step-up’ therapy. For tofacitinib, the pooled analysis of 10 trials showed that tofacitinib was more efficacious on signs and symptoms, disability and appeared to be more efficacious on structural damage than control treatment with placebo (OR (95% CI)—American College of Rheumatology 20% (ACR20) response: 2.44 (1.97 to 3.02)) or treatment with MTX (ACR20 response: 2.38 (1.66 to 3.43)).
Conclusions Addition of low-dose glucocorticoids to csDMARD therapy produces benefits in early RA. Under tight control conditions, combination therapy with csDMARDs is no better than MTX monotherapy. Tofacitinib is a new DMARD with proven efficacy.
- Rheumatoid Arthritis
- Treatment
- Corticosteroids
- DMARDs (synthetic)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Since rheumatoid arthritis (RA) imposes a considerable burden for patients, their families and society, therapeutic approaches call for early intervention with, and timely adaptation of, disease-modifying antirheumatic drugs (DMARDs), either as monotherapy or as combination therapy, in order to avoid irreversible damage, long-term disability and premature death. In 2010 a European League Against Rheumatism (EULAR) task force aggregated the available information on RA treatment into practical recommendations,1 based on several systematic literature reviews (SLRs) providing the state of evidence at that time.2–4 DMARDs form two major classes: synthetic chemical compounds (synthetic DMARDs, sDMARDs) and biological agents (bDMARDs). We have now updated these 2009 searches to obtain the available published information on efficacy of synthetic DMARDs as monotherapy or combination therapy, with and without addition of glucocorticoids (GCs). Where appropriate, we will adhere to the recently proposed nomenclature for sDMARDs which, among other aspects, differentiates between conventional synthetic (cs) and targeted synthetic (ts) DMARDs.5
Methods
The four main research questions pertained to the efficacy on signs and symptoms, disability and joint damage. Topics considered were (1) the addition of GCs to csDMARDs in early RA; (2) methotrexate (MTX) as monotherapy versus its combination with other csDMARDs (disregarding the addition of biological agents discussed elsewhere)6; (3) individual csDMARDs and (4) tofacitinib, a new tsDMARD specifically targeted at inhibition of Janus kinases. Safety concerns were examined in a separate SLR.7 Tapering strategies for GCs were not dealt with in this SLR.
Guidelines for SLRs were followed and are detailed in the online supplementary material.
Study selection
A SLR was performed in PubMed Medline, Embase, Cochrane library and major congress abstracts after January 2009 until January 2013 for GCs and csDMARDs and until March 2013 for tofacitinib. In addition, abstracts of the American College of Rheumatology (ACR) meetings 2011–2012 and EULAR Congresses 2011–2013 were screened and full publications related to such abstracts taken into account until mid-2013. Only randomised controlled trials (RCTs) were included in this analysis. The risk of bias of the included studies was assessed using the Cochrane Collaboration's tool for risk of bias.8
Data collection
Efficacy was assessed by the change in signs and symptoms and disability status between baseline and week 24, week 52 and week 104, when available, and by the change in radiographic joint damage between baseline and week 52 and week 104.
Statistical analysis
In each trial the effect size or the standardised response mean for continuous measures and ORs for dichotomous measures were determined to assess the magnitude of the treatment effect. Where possible, pooled effect size, pooled standardised response mean and pooled OR were calculated by meta-analysis, using the inverse of variance method. RevMan V.5.2 (Review Manager, Copenhagen, The Nordic Cochrane Centre, The Cochrane Collaboration, 2012) statistical software was used. Statistical heterogeneity was tested by Q test and I2 test. All meta-analyses were carried out using random-effects models in cases of statistical heterogeneity.
Results
Glucocorticoids in early RA
Of 222 potentially relevant articles, five new studies relating to four RCTs were included (table 1). The selection of articles is shown in online supplementary figure A. Of the five studies, two trials were open-label trials with a high ‘risk of bias’ score10–12; one study was reported only as an abstract at the 2011 EULAR congress10 and two studies were RCTs with a low ‘risk of bias’.9 ,13 The SAVE (Stop Arthritis Very Early) trial has a particular design since its objective was to prevent development of RA in patients with very early arthritis who did not yet meet RA classification criteria; it did not show efficacy of a single GC injection in this respect, irrespective of added csDMARDs.9 In the other studies all patients had early RA, with a mean disease duration of <1 year and a mean Disease Activity Score in 28 joints (DAS28) of between 5.0 and 5.9. Overall, initial treatment of RA with low-dose prednisone plus MTX showed higher rates of remission at 12 and 52 weeks, lower DAS at 24 weeks and lower Health Assessment Questionnaire (HAQ) scores at 24, 52 and 104 weeks (table 1).10–13 A highly informative study (CAMERA II (Computer Assisted Management in Early Rheumatoid Arthritis trial-II)) reported the efficacy of GCs in a 2-year, prospective, randomised, placebo-controlled, double-blind, multicentre trial in 236 patients with early RA (duration <1 year). The MTX plus prednisone (10 mg/day) strategy was more effective than MTX plus placebo in reducing the progression of erosive joint damage at 104 weeks (primary outcome) (table 1). Patients receiving MTX plus prednisone attained sustained remission at an earlier time point during the trial than patients receiving MTX alone. In addition, the need for additional treatment (subcutaneous MTX, ciclosporin or adalimumab) was significantly lower in the MTX plus prednisone group than in the MTX monotherapy group.13
Randomised controlled trials of glucocorticoids added to DMARDs in early arthritis
Overall, there were no new safety concerns over 2 years beyond those previously reported.13–15
csDMARDs
Initially, 498 potentially relevant articles were screened by their abstracts.
Efficacy of MTX in monotherapy versus in combination
Two new studies were RCTs comparing MTX monotherapy with MTX in combination with another csDMARD, without differences in GC usage between the arms, in adult RA (selection process shown in online supplementary figure B).
The tREACH study was a randomised, single-blinded clinical trial in patients with recent-onset arthritis who had a ‘high probability of progressing to persistent arthritis’, with three arms: (A) combination therapy with csDMARDs (MTX+sulfasalazine (SSZ)+hydroxychloroquine (HQ)) with intramuscular GCs (91 patients); (B) combination therapy with oral GCs starting at 15 mg/day and tapering over 10 weeks (93 patients) and (C) MTX with oral GCs (same tapering scheme, 93 patients). Medication was intensified to MTX+etanercept (50 mg/week) if the DAS44 was≥2.4 at 3 months,16 which is rather early in light of the time to maximal effects of csDMARDs and current recommendations.2 At 3 months (interim analysis) the change in DAS was similar in both arms with the triple combination and higher than in the arm with monotherapy (mean (SD) change: −1.4 (1.0), −1.5 (1.0) and −1.2 (1.0), respectively), but baseline scores for HAQ disability index, tender joint count and C-reactive protein were 10% higher in the monotherapy arm than in both combination arms.16 Other outcomes, such as change in HAQ score, swollen joint count and erythrocyte sedimentation rate (ESR), did not differ across the groups,16 and the significant advantage of change in DAS score at 3 months was lost at 1 year.17
The Treatment of Early Aggressive Rheumatoid Arthritis (TEAR) study is a 2-year, randomised, double-blind trial with a two-by-two factorial design, of which two arms are pertinent for the current SLR: immediate oral triple therapy (MTX+SSZ+HQ) (132 patients), or step-up from MTX monotherapy to MTX+SSZ+HQ (124 patients) at week 24 if the DAS28-ESR was >3.2.18 The objective was to assess which approach is better—that is, to immediately treat all patients with early RA and a more severe phenotype (anti-cyclic citrullinated peptide antibody and/or rheumatoid factor positivity, or erosive disease) with combinations of DMARDs, or to reserve combination DMARD therapy for patients who do not have an appropriate response to monotherapy. The number of participants who did not complete this study was higher (32%) than the authors had originally expected (10%), resulting in loss of statistical power and interpretational problems. Furthermore, the main analysis presented was a completers-only analysis. An earlier improvement occurred with immediate combination arms, but after initial MTX monotherapy in those patients who lacked sufficient response a rapid improvement to similar levels as with immediate triple therapy was seen upon intensification of treatment. There were no radiographic advantages in favour of combination therapy. So, using principles of tight control and treat-to-target, clinical and radiographic benefits were no higher with immediate triple therapy than with ‘step-up’ therapy’.18
Efficacy of csDMARDs
Twenty-five studies were analysed. No new data conflicting with the previous conclusions were found. Several RCTs confirmed the efficacy of MTX as both first and second DMARD.19–24 Only one RCT included leflunomide: it compared MTX and leflunomide in 368 patients with early RA. Of the 240 subjects who were randomised and treated, 129 received leflunomide and 111 received MTX. This study showed that MTX was better than leflunomide for the four primary clinical efficacy endpoints (tender joint count, swollen joint count, physician and patient global assessment score). The difference was not statistically significant for the three secondary clinical efficacy endpoints (morning stiffness, pain intensity, HAQ).25 Very few studies confirmed the efficacy of sulfasalazine.26 ,27 The studies analysed did not provide new information on other csDMARDs.
Tofacitinib
Literature search results and trials characteristics
Initially, 27 potentially relevant articles were screened. Finally, 10 RCTs were included—four phase II studies and six phase III trials (selection process is shown in online supplementary figure C). Studies’ and patients’ characteristics are detailed in table 2.
Randomised controlled trials of tofacitinib in rheumatoid arthritis
Efficacy of tofacitinib at 5 mg twice daily
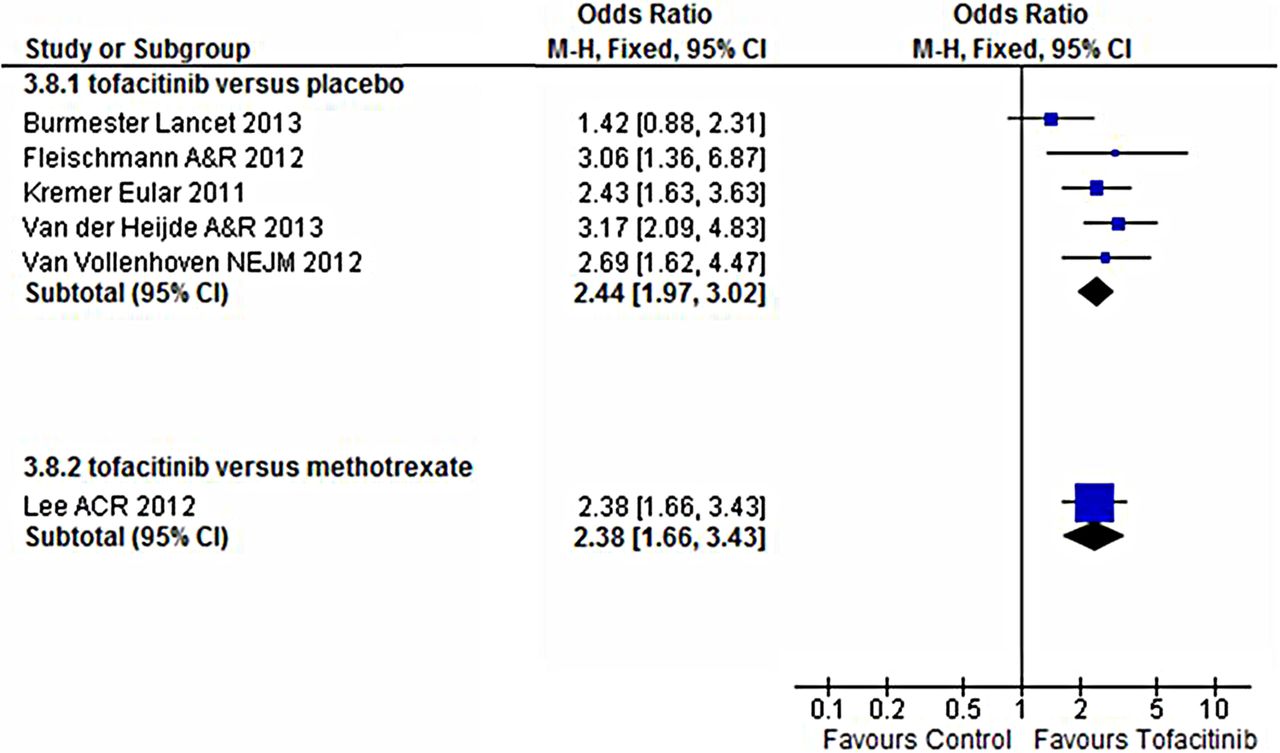
The meta-analysis showed that tofacitinib was better than the respective control groups in its effect on signs and symptoms and physical function at 12, 24 and 52 weeks. As an example, the pooled OR (95% CI) for ACR20 response at 24 weeks versus placebo was 2.44 (1.97 to 3.02) (figure 1 and online supplementary material).

{kind=link}
Efficacy of tofacitinib on ACR20 response criteria at 24 weeks.
Radiographic progression was assessed in two studies. In the ORAL Start study (early RA, MTX-naïve) mean change in total Sharp–van der Heijde score (SHS) score at 6 months was 0.18 for tofacitinib 5 mg twice daily versus 0.84 for MTX monotherapy (p<0.05) and the proportion of ‘non-progressors’ (≤0.5 unit increase from baseline in total SHS) was 83.5% versus 70.5%, respectively.37 In the ORAL Scan study (established RA, MTX-inadequate responder), mean change in total SHS score was 0.12 versus 0.47 (p=0.079) at 24 weeks and 0.3 versus 1.0 (p=0.0558) at 52 weeks and the proportion of ‘non-progressors’ was 86% versus 74.1% (p≤0.05) at 52 weeks.32
More details are shown in the online supplementary material.
Discussion
This SLR was performed to inform the EULAR task force involved in updating the 2010 recommendations for the management of RA on the efficacy of csDMARDs as monotherapy or combination therapy, with and without GCs in adult patients with RA. Overall, this SLR confirmed the SLRs performed in 20092–4 and expanded the overall insights.
Although the place of GC therapy in early RA is still a matter of debate, previous studies have clearly shown the benefit of adding GCs to csDMARD monotherapy or combination therapy, whether at low (≤10 mg/day) or higher doses, especially in patients with early RA.38–41 In 2010, we suggested that GCs might be used as ‘bridge therapy’ before slow-acting DMARDs have taken full effect. Several new studies have confirmed these data. Interestingly, the tREACH trial showed that intramuscular and oral GCs are equally effective as bridging treatments16 and thus answered one of the research questions posed in 2010.1 Moreover, accumulating evidence suggests that low-dose treatment is well tolerated and similarly effective, while reducing the risk of side effects associated with higher doses.13 ,42 However, bone loss should be prevented using appropriate strategies.43 Further research is needed, especially into chronotherapy44 and intra-articular GC therapy.
For combination therapy of csDMARDs, some studies suggest that triple therapy with MTX+SSZ+HQ may be better than MTX monotherapy in improving signs and symptoms.45 ,46 The tREACH study in its interim analysis at 3 months showed a somewhat faster improvement on DAS28 (but not on HAQ score, swollen joint count or ESR) with triple therapy+GCs than with MTX+GCs, but this difference was not maintained at 1 year.16 ,17
Moreover the TEAR trial has shown that, using tight control and principles of treat-to-target, clinical, functional and structural outcomes were no better with immediate triple therapy than with ‘step-up’ therapy.18
It has been difficult to interpret the results of several investigator-initiated pragmatic or effectiveness trials such as TEAR and tREACH and use them to choose the most appropriate treatment strategy. These trials are justified by clear practical clinical questions that go beyond whether a particular treatment is effective or not; however, the trial methodology is often so complicated that the trial performance and reporting may be jeopardised. Examples of these aspects are trials that do not reach their target number of patients (with lack of statistical power as a consequence), trials with high drop-out rates, or with relatively small numbers of patients (‘completers’) in which the primary endpoint has been assessed (with a risk of ‘bias by completion’), trials with an unplanned interim analysis or a change of primary endpoint (with the risk of convenience reporting, or reporting at odds with the definite results) and trials with an a priori superiority design that are reported with spurious non-inferiority conclusions.47 However, these studies explored valuable concepts that are of significant practical importance to rheumatologists and patients.
There are some limitations to our analyses; some outcomes from some studies could not be included in this meta-analysis because we needed at least one measure of variability such as SD. Nevertheless, the current SLR informs the Task Force on the evidence that (i) addition of low-dose GC to csDMARD monotherapy or combination therapy increases overall efficacy; (ii) combination of csDMARDs as triple therapy, is efficacious, but MTX monotherapy appears to be similarly efficacious, especially when combined with GCs and employing a treat-to-target approach; (iii) tofacitinib is a clinically, structurally and functionally efficacious agent.
Importantly, safety aspects were not covered here, since they were part of a separate SLR.7
Acknowledgments
The authors thank Michel Viala for his help with the literature search.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Handling editor Francis Berenbaum
-
Contributors All authors contributed and finally approved the current manuscript.
-
Competing interests CG-V—consultation and/or speaking engagements: Abbvie, BMS, MSD, Pfizer, Roche-Chugai, UCB; research funding: Expanscience, Nordic Pharma, Pfizer. JN—consultation and/or speaking engagements: UCB. SR—consultation and/or speaking engagements: Fundação para a Ciência e Tecnologia. RL—consultation and/or speaking engagements: Abbott/AbbVie, Ablynx, Amgen, Astra-Zeneca, Bristol Myers-Squibb, Centocor, Glaxo-Smith-Kline, Merck, Novartis, Pfizer, Roche, Schering-Plough, UCB, Wyeth; research funding: Abbott, Amgen, Centocor, Novartis, Pfizer, Roche, Schering-Plough, UCB, Wyeth. MHB—consultation and/or speaking engagements: Abbott, Bristol Myers-Squibb, Chugai, Pfizer, Roche; research funding: Pfizer. JSS—consultation and/or speaking engagements: Abbott/Abbvie, Amgen, Astra-Zeneka, BMS, Celgene, Glaxo, Infinity, Janssen, Lilly, Medimmune, Menarini, MSD, Novo-Nordsik, Pfizer, Roche, Samsung, Sandoz, Sanofi-Aventis, UCB, Vertex; research funding: Abbott, BMS, MSD, Pfizer, Roche, UCB. LG—consultation and/or speaking engagements: Abbott, BMS, Chugai, Pfizer, Roche, UCB.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Recommendation
- Clinical and epidemiological research
- Clinical and epidemiological research