Article Text

Abstract
Objective To evaluate the response to treatment of autoinflammatory diseases from an international registry and an up-to-date literature review.
Methods The response to treatment was studied in a web-based registry in which clinical information on anonymised patients with autoinflammatory diseases was collected retrospectively as part of the Eurofever initiative. Participating hospitals included paediatric rheumatology centres of the Paediatric Rheumatology International Trial Organisation network and adult centres with a specific interest in autoinflammatory diseases. The following diseases were included: familial Mediterranean fever (FMF), cryopyrin-associated periodic syndromes (CAPS), tumour necrosis factor (TNF)-receptor associated periodic syndrome (TRAPS), mevalonate kinase deficiency (MKD), pyogenic arthritis pustulosis acne (PAPA) syndrome, deficiency of interleukin-1 receptor antagonist (DIRA), NLRP12-related periodic fever and periodic fever aphthosis pharyngitis adenitis (PFAPA) syndrome. Cases were independently validated by experts for each disease. A literature search regarding treatment of the abovementioned diseases was also performed using Medline and Embase.
Results 22 months from the beginning of the enrolment, complete information on 496 validated patients was available. Data from the registry in combination with evidence from the literature confirmed that colchicine is the treatment of choice for FMF and IL-1 blockade for DIRA and CAPS. Corticosteroids on demand probably represent a valid therapeutic strategy for PFAPA, but also for MKD and TRAPS. Patients with poorly controlled MKD, TRAPS, PAPA or FMF may benefit from IL-1 blockade; anti-TNF treatment may represent a possible valuable alternative.
Conclusions In the absence of high-grade evidence, these results could serve as a basis for therapeutic guidelines and to identify candidate drugs for future therapeutic trials.
Statistics from Altmetric.com
Introduction
Autoinflammatory syndromes are disorders characterised by recurrent or chronic inflammation caused by dysregulation of the innate immune system.1 Since most of these diseases are very rare, treatment data are limited. Few randomised controlled trials (RCTs) have been conducted; for most autoinflammatory diseases, clinicians have relied on case reports and personal experience. The rarity of these diseases and the fragmentary clinical experience has hampered the development of consensus for treatment guidelines. We set out to document current clinical practices and to compare these with published reports on treatment of autoinflammatory diseases in order to identify promising treatment approaches. To analyse current practice, we used the Eurofever Registry. This international web-based registry was designed to identify the clinical characteristics and response to treatment in patients who had been treated for autoinflammatory diseases.2
Methods
Eurofever Registry
An international registry for autoinflammatory diseases was initiated by the Eurofever initiative (EAHC Project No. 2007332).2 A secured web-based registry was hosted at the Paediatric Rheumatology International Trial Organisation website (PRINTO, http://www.printo.it). Participating hospitals included paediatric rheumatology centres of the PRINTO network and adult centres with a specific interest in autoinflammatory diseases.3 Seventy-seven centres from 33 countries participated in this effort. Local attending physicians retrospectively provided anonymised demographic and clinical information on patients with the following diseases: familial Mediterranean fever (FMF), cryopyrin-associated periodic syndromes (CAPS), tumour necrosis factor (TNF)-receptor associated periodic syndrome (TRAPS), mevalonate kinase deficiency (MKD, also known as hyper IgD and periodic fever syndrome HIDS), pyogenic arthritis pustulosis acne (PAPA) syndrome, deficiency of interleukin-1 receptor antagonist (DIRA), NLRP12-related periodic fever, and periodic fever aphthosis pharyngitis adenitis (PFAPA) syndrome. Inclusion criteria for each disease are given in the online supplement. All completed cases were anonymously and independently validated by at least one expert for the specific disease in order to confirm the diagnosis. All cases validated before 1 September 2011 for whom the response to treatment had been documented were used for the analysis. All treatments that had been tried during the life time of the patient were evaluated. Local physicians reported per treatment the way it was prescribed (maintenance or during attacks), the response and whether the drug was continued or discontinued. The response was graded as complete remission, partial remission, failure or worsening. We considered remission to be complete when signs of active disease were absent and reported inflammatory markers had normalised, allowing for the persistence of sequelae.
Literature search
A literature search on the treatment of autoinflammatory diseases was performed using Medline, Embase, Cochrane databases and an additional search within the references of the retrieved papers. Only articles in English published before February 2012 were included. The reader is referred to the online supplement for more information about the search and selection of papers. All the treatments that had been reported were included in the analysis of the literature and graded for strength of evidence according to the Oxford CEBM table.4 When the response was not clearly described, the authors of the original papers were contacted. For each disease, only papers with the highest grade of evidence were included on each treatment (see supplementary figure 1). Of the 175 retrieved papers, only prospective trials or studies on at least five patients were included in the reference list of the print version of this article. Reports on fewer than five patients can be found in the supplementary references in the online supplement.
Results
Eurofever Registry
By 31 August 2011, complete clinical information was available on 902 patients. Of these patients, diagnosis was validated and confirmed in 684 at that time. In 188 patients, information on treatment was incomplete, so 496 patients were included in the study. Many patients had tried multiple drugs. The characteristics of these patients are summarised in table 1. Information about reported side effects and patients who received non-steroidal anti-inflammatory drugs (NSAIDs) and/or corticosteroids as single therapeutic strategy can be found in supplementary tables 2 and 3, respectively.
Baseline data of the patients included in the Eurofever Registry
Familial Mediterranean fever (FMF)
Eurofever Registry
In the Eurofever Registry, data on 121 patients with FMF are available. All received colchicine; 75 (62%) experienced a complete response, 44 (36%) a partial response and two failed to respond. Side effects, mainly diarrhoea, were noted in five patients (see supplementary table 2). No patient was reported to have discontinued colchicine. Forty-two patients were additionally treated with NSAID and/or corticosteroid on-demand with a variable response (figure 1). Three patients were treated with anakinra, with a complete response in all of them, including one patient who failed to respond to colchicine.
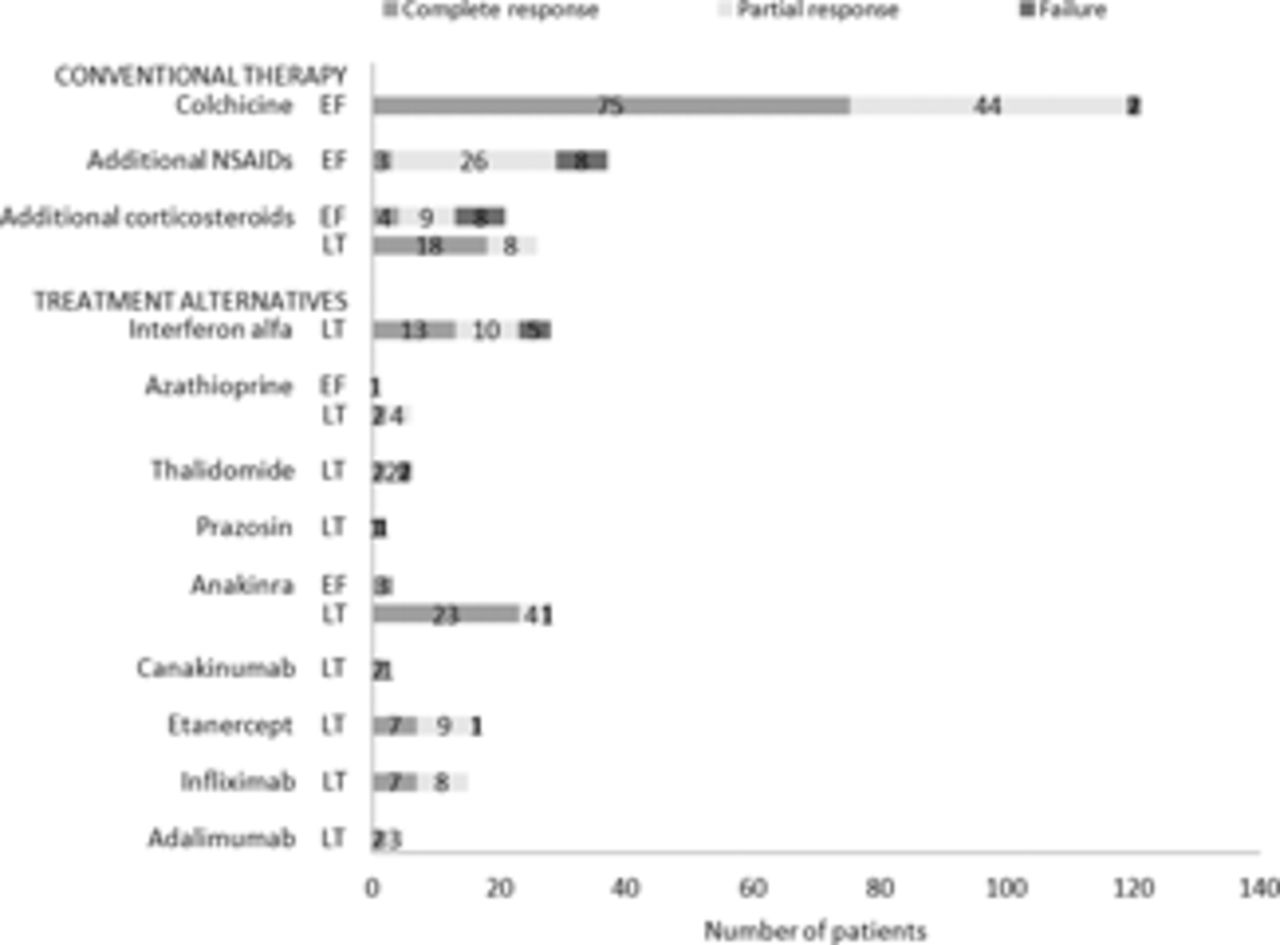
Response to treatment in 121 patients with familial Mediterranean fever from the Eurofever Registry (EF) and combined data on 139 patients from the literature (LT) from 48 papers. Treatment alternatives are therapies used for colchicine-resistant patients. It was not possible to derive data about efficacy per patient in the randomised controlled trial of Tunca et al.15
Data from the literature
In three RCTs, colchicine significantly decreased the number of attacks.5,–,7 As reviewed by Kallinich in 2007, colchicine induces complete remission in two-thirds and partial remission in approximately one-third of paediatric patients with FMF and prevents development of AA amyloidosis.8 However, 5–10% of the patients fail on colchicine because of ongoing inflammatory activity or severe side effects.8 ,9 Alternative therapies have therefore been explored and are summarised in figure 1 (data are also derived from supplementary references 1–39).
A trial of 31 patients indicates that on-demand additional corticosteroids are effective in decreasing attack symptoms and pain.10 Other cases suggest protracted febrile myalgia responds to corticosteroids.11 Interferon α (IFNα) given at the onset of an attack reduced the intensity and duration in three prospective series12,–,14 but, in a RCT, IFNα did not have a significant clinical effect.15 Studies describing a beneficial effect of prazosin, thalidomide or azathioprine have not been replicated.16 The vast majority of reported cases using anti-interleukin (IL)-1 therapy (anakinra or canakinumab) have shown complete resolution of attacks and normalisation of acute phase reactants.17 ,18 TNF blockade with etanercept, infliximab or adalimumab has been studied especially in patients with protracted arthritis and resulted in partial or complete cessation of the attacks.16 ,19
Cryopyrin-associated periodic syndromes (CAPS)
Eurofever Registry
Among the 94 patients with CAPS analysed in the Eurofever Registry, 86 received at least one anti-IL-1 agent. Anakinra was used in 61 patients with a complete response in 39 (64%) and a partial response in 21 (34%). Rare side effects included local skin reactions and anaphylactoid reactions (see supplementary table 2). Canakinumab induced complete remission in 39 patients (75%) and partial remission in 13 (25%). Corticosteroids and NSAIDs were beneficial in, respectively, 19/24 and 25/36 of the patients using these drugs, mostly as on-demand therapy, although complete remission was reported in just two patients on NSAIDs and none on corticosteroids. Eight patients reported a satisfactory response to NSAIDs and/or corticosteroids without the use of IL-1 blockade (see supplementary table 3).
Data from the literature
In a RCT on 35 patients, canakinumab was significantly effective.20 In a cohort study, 85 (78%) of 109 canakinumab-naïve patients experienced a complete response and 23 a partial response. Furthermore, 127 (90%) of the total 141 patients did not relapse and had normal C reactive protein (CRP)/serum amyloid A levels.21 This effect is also seen in smaller pilot studies.22 ,23 Another IL-1 targeted drug, rilonacept, also induced a significant improvement in 47 patients enrolled in a RCT and in five patients in a pilot study.24 ,25
Combined data of 107 patients from cohort studies show that 84 (79%) achieved complete remission with anakinra and, in some young patients, hearing improved as well.22 ,26,–,33 However, since anakinra does not always normalise the acute phase reactants, it may be necessary to increase the dose in order to induce and maintain complete remission.32 Furthermore, a lack of complete control of CNS-related clinical manifestations and bone dysplasia has also been reported.33
Tumour necrosis factor-receptor associated periodic syndrome (TRAPS)
Eurofever Registry
NSAIDs and corticosteroids were prescribed in 48 and 88 patients, respectively, of the Eurofever Registry, mostly as on-demand therapy, and were beneficial in the majority of them (figure 2). Colchicine was beneficial in 21 of 39 patients, three of whom had a complete response. Patients with the mild R92Q mutation seem to respond better to NSAIDs and colchicine compared with other TNFRSF1A mutations. Etanercept was beneficial in 32 of the 37 patients, although only 11 (30%) experienced a complete response. Anakinra is a promising therapy, inducing a complete response in 26 of 33 patients (79%) and a partial response in five others.

Response to treatment in 113 patients with tumour necrosis factor-receptor associated periodic syndrome from the Eurofever Registry (EF) and combined data on 187 patients from the literature (LT) from 48 papers.
Data from the literature
Case series indicate that NSAIDs and corticosteroids are often used to control the clinical manifestations or to abort fever episodes.34 In comparison with data from Eurofever, NSAIDs and steroids are reported to have a less beneficial impact in the control of TRAPS-related clinical manifestations (figure 2). Overall, the effect of colchicine is disappointing.35,–,37 Anakinra induced a complete response in half of the published cases and in all five patients of a prospective trial.38,–,41 As in the Eurofever Registry, most patients in the literature treated with etanercept had a favourable but incomplete response.36 ,39 ,41,–,44 Moreover, the response was reported to decline with time.43 Infliximab gave an excellent response in one case that was unresponsive to etanercept, but failure or even deterioration was noted in the seven other treated patients.36 ,43 This deterioration was also seen with adalimumab.43 Tocilizumab appeared effective in one case (see also supplementary references 40–73).
Mevalonate kinase deficiency (MKD)
Eurofever Registry
In the Eurofever Registry, NSAIDs and corticosteroids were reportedly used mainly as on-demand therapy in 39 and 33 patients, respectively. The response to NSAIDs was complete in five patients (13%) and partial in 25 (64%) (figure 3). Of these five patients, three also used corticosteroids with a complete response and one with a partial response. Corticosteroids induced a complete response in eight (24%) and a partial response in another 22 (67%). In seven complete responders, corticosteroids (in five cases in combination with NSAIDs) were referred as the only therapeutic strategy. Colchicine was used in 17 patients with a lack of response in the majority of them (65%). Anakinra was effective in 24 (89%) of 27 patients, inducing complete remission in six (22%). Etanercept was effective in 11 (65%) of 17 treated patients, with only one complete response.

Response to treatment in 67 patients with mevalonate kinase deficiency from the Eurofever Registry (EF) and combined data on 187 patients from the literature (LT) from 19 papers.
Data from the literature
Case series suggest that the results of NSAIDs and colchicine are disappointing.45 ,46 Corticosteroids given in high doses can decrease the duration of fever attacks, although the results found in the literature are less favourable than those reported by centres involved in Eurofever.45
In a RCT, thalidomide did not decrease attack frequency.47 In a small RCT, simvastatin decreased the attack frequency but clinically the results were very modest.48 In other reports, statins generally failed to control the disease.45 ,46
Both etanercept and anakinra have been reported to induce major improvement, but failure and even deterioration have also been described.45 ,46 In a prospective trial with seven patients receiving on-demand anakinra, attack duration was significantly shorter and the maximum CRP decreased.49 Patients who do not respond on etanercept could benefit from anakinra and vice versa.50 A few patients have been successfully treated with the newer biological agents adalimumab and canakinumab46 (see also supplementary references 74–87).
Pyogenic arthritis pyoderma acne syndrome (PAPA)
Eurofever Registry
Five patients with PAPA enrolled in the Eurofever Registry. NSAIDs alone failed to control disease activity. Although corticosteroids induced a complete response in two of the five patients, both discontinued the drug in favour of biological agents. Indeed, complete responses have been achieved with etanercept, the combination of isotretinoin and anakinra and adalimumab.
Data from the literature
Reports from the literature suggest that corticosteroids are beneficial for arthritis but less effective in pyoderma gangrenosum.51,–,53 Immunosuppressants are partially effective at best, although the combination of sulfasalazine and leflunomide induced remission in one reported case.52 ,53 Anakinra was completely effective in three of 10 reported cases and partially in five others. Etanercept induced complete remission in two out of four patients. All three reported patients with PAPA using infliximab responded completely, as well as two patients using adalimumab53 (see also supplementary references 88–96).
Deficiency of IL-1 receptor antagonist (DIRA)
Since endogenous IL-1RA is lacking in patients with DIRA, its supplementation is the mainstay of treatment. Of the 11 patients reported in the literature (see also supplementary references 97–100) that were treated with anakinra, nine experienced a complete remission, including the two enrolled in the Eurofever Registry who are also described by Aksentijevich.54 The two patients with a partial response had a homozygous deletion causing IL36-receptor antagonist deficiency in addition to DIRA, possibly explaining the reduced efficacy of anakinra.
NLRP12-related periodic fever
One of the two patients in the Eurofever Registry, who was also reported by Borghini et al, achieved complete control of the disease by the combination of corticosteroids and antihistamines.55 Other reports (supplementary references 101, 102) describe a beneficial effect of NSAIDs and corticosteroids. Anakinra initially induced significant improvement but the effect decreased in time.
Periodic fever adenitis pharyngitis aphthosis syndrome (PFAPA)
Eurofever Registry
In 81 of 92 patients with PFAPA from the Eurofever Registry, corticosteroids were given at the onset of attacks. This aborted fever in 73 patients (90%) and induced partial improvement in an additional six (figure 4). NSAIDs were beneficial in 21 of the 28 patients, but only completely effective in one patient as monotherapy and an additional one in combination with corticosteroids. Tonsillectomy (with or without adenoidectomy) was performed in eight patients only. A complete response was observed in four patients, whereas a partial response was reported in three patients. Colchicine induced a complete response in three patients and a partial response in two. Notably, cimetidine was not reported in any of the patients.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Response to treatment in 92 patients with periodic fever adenitis pharyngitis aphthosis syndrome from the Eurofever Registry (EF) and combined data on 404 patients from the literature (LT) from 21 papers.
Data from the literature
Cohort studies and case series indicate that corticosteroids are effective in aborting fever episodes.56,–,62 Resolution of the fever episode usually occurs within 24 h.60 Unfortunately, some patients on corticosteroids report an increased frequency of the episodes.58,–,60 ,63
Although cimetidine had initially been reported to induce remission, it was ineffective in the majority of recently reported patients (figure 4).60 ,61 ,64 Beneficial effects of colchicine or thalidomide have been reported occasionally, but these results have not been replicated.65 A cohort of five patients with PFAPA treated with anakinra all experienced a rapid decline of fever, although two relapsed.66
A meta-analysis of two RCTs indicates that (adeno)tonsillectomy is significantly effective in inducing a complete remission,67 although these results should be interpreted with caution because of the limitations of the constituent trials.67 Case series and prospective cohort studies show an overall good response to (adeno)tonsillectomy as well.57,–,62 ,64 ,67,–,72
Summary of data from the literature
The overall published evidence on treatment of periodic fever syndromes is summarised in table 2 (see also supplementary references 103–106).
Summary of evidence for treatments of choice
The doses reported for each drug (table 2) were the following: colchicine: 0.5–2 mg per day, anakinra 100 mg or 1–5 mg/kg per day (PFAPA: once at the onset of an attack), etanercept 25 mg twice a week, canakinumab 150 mg or 2 mg/kg every 8 weeks, rilonacept 160 mg per week, infliximab 3–5 mg/kg every 6–8 weeks, IFNα 3–5 million units at the onset of an attack. The types and dosing regimens of NSAIDs and corticosteroids varied widely among studies.
Discussion
This paper describes the responses to treatment in the largest international cohort of patients with periodic fever syndromes and provides a review of all reported series and case reports available in the English language literature.
The rarity of these diseases poses important limitations to trials. Hence, the level of published evidence for treatment in most autoinflammatory diseases is low, derived from small series and case reports, prone to bias in favour of novel drugs and positive results. Moreover, in nearly all studies observation has been short, limiting data on long-term efficacy and safety.
One of the main goals of the Eurofever Registry is to provide ‘real-life’ information about the clinical presentation, course and response to treatment of the autoinflammatory diseases. The strengths of this approach include broad geographical coverage with involvement of both adult and paediatric centres, selection of well-defined patients through validation of each patient by independent disease experts and the possibility to evaluate the response to several treatments per patient, including ‘old’ drugs like NSAIDs and corticosteroids which have been important in clinical practice but underreported in the literature. We have shown in supplementary table 3 that the majority of patients with PFAPA and approximately one-third of those with MKD and TRAPS received NSAIDs and/or corticosteroids as single therapy.
A number of differences appear between the Eurofever Registry and the reviewed literature. A lower frequency of complete responders is seen in the registry for colchicine in FMF. This might be due to a selection bias in Eurofever since patients who had achieved complete remission might not have been followed any longer by specialised centres whereas patients who had been difficult to treat were.
Similarly, in CAPS the number of complete responders to anti-IL-1 therapy in the registry is lower than expected from the literature (eg, anakinra: 65% complete response in Eurofever vs 85% in the literature).The reason for this difference remains unclear.
The cohort of TRAPS patients in the registry is the largest ever reported, including more patients using anti-IL-1 therapy than have been reported in the literature. Interestingly, both in the registry and in the literature, patients with TRAPS tended to respond better to IL-1 targeted therapies than anti-TNF agents. This is in accordance with recent insights in the pathophysiology of TRAPS.73
In patients with MKD in the registry, NSAIDs and corticosteroids appear to perform better than what might be expected from the literature. A sizeable proportion of patients with MKD are adequately controlled with corticosteroids. In fact, the response rate to corticosteroids and NSAIDs in the registry is at least comparable to anti-TNF and anti-IL-1 agents. This difference could be due to a publication bias in favour of biological agents whose effectiveness is often described together with failure of corticosteroids and NSAIDs.
A number of caveats apply to the present study. The literature review is mainly derived from case reports and case series with different clinical endpoints and follow-up periods, and this precludes valid quantitative analysis.
A major limitation to the interpretation of both registry and literature data is the absence of criteria for partial and complete remission. Notably, no minimal duration of remission has ever been defined. Another problem affecting interpretation of both datasets was the use of multiple therapies in unclear order (possibly simultaneously) and especially during fever attacks. Despite these drawbacks, this cohort analysis combined with the literature review provides the best available current evidence on response to treatment in the different periodic fever syndromes. We conclude that colchicine is the treatment of choice for FMF and IL-1 blockade for DIRA and CAPS. Corticosteroids on demand probably represent a valid therapeutic strategy for PFAPA and for MKD and TRAPS. Most patients with otherwise poorly controlled MKD, TRAPS, PAPA syndrome or FMF may benefit from IL-1 blockade; anti-TNF treatment may represent a possible valuable alternative.
In the absence of high-grade evidence, our findings should facilitate the development of initial treatment guidelines for autoinflammatory diseases. There remains a clear need for well-defined remission criteria. These are currently being developed in order to enable high-quality therapeutic trials. Ultimately, the large number of patients enrolled in the Eurofever Registry should enable such trials to provide evidence-based effective and safe therapies for all autoinflammatory diseases.
Acknowledgments
The authors thank Eugenia Mosci and Michele Pesce of the PRINTO coordinating centre for their help in web database implementation and data collection management. The authors also thank all members of PRINTO who participated as investigators in the study and whose enthusiastic effort made this work possible. Albania: Anuela Kondi; Argentina: Carmen De Cunto, Graciela Espada, Ricardo Russo; Armenia: Gayane Amaryan; Australia: Christina Boros; Belgium: Carine Wouters; Brazil: Sheila Knupp Feitosa de Oliveira; Chile: Arturo Borzutzky; Croatia: Marija Jelusic-Drazic; Czech Republic: Pavla Dolezalova; Denmark: Troels Herlin; France: Marine Desjonqueres, Djamal Djeddi, Veronique Hentgen, Martha Darce; Georgia: Maka Ioseliani; Germany: Rainer Berendes, Gerd Horneff, Annette Jansson, Kirsten Minden, Tobias Schwarz, Ralf Trauzeddel; Greece: Florence Kanakoudi Tsakalidou, Olga Vougiouka; Hungary: Tamàs Constantin; India: Anand Prahalad Rao; Israel: Riva Brik, Liora Harel; Italy: Maria Alessio, Luciana Breda, Rolando Cimaz, Rita Consolini, Giovanna Fabio, Rosaria Garozzo, Loredana Lepore, Raffaele Manna, Antonella Meini, Alma Nunzia Olivieri; Latvia: Valda Stanevicha; Lithuania: Skirmante Rusoniene; Netherlands: Esther Hoppenreijs; Oman: Safiya Al-Abrawi; Russian Federation: Irina Nikishina; Saudi Arabia: Wafaa Mohammed Saad Sewairi; Serbia: Gordana Susic; Slovakia: Peter Ciznar; Slovenia: Tadej Avcin; Spain: Jordi Anton, Rosa Bou, Rosa Merino, Maria Jesus Rua Elorduy; Sweden: Anders Fasth; Turkey: Guzide Aksu, Erkan Demirkaya.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Funding This project is supported by the Executive Agency for Health and Consumers of the European Union (EAHC, Project No2007332) and by Coordination Theme 1 (Health) of the European Community's FP7, grant agreement number HEALTH-F2-2008-200923. Unrestricted educational grants were also kindly provided by PRINTO and Novartis.
-
Competing interests The Gaslini Hospital, which is the public hospital where NR, MG and AM work as full-time employees, has received contributions to support PRINTO and Eurofever research activities from Abbott, ACRAF, Astra Zeneca, Bristol Myers and Squibb, Centocor Research & Development, Eli Lilly and Company, ‘Francesco Angelini’, GlaxoSmithKline, Italfarmaco, Novartis, Pfizer, Roche, Sanofi Aventis, Schwartz Biosciences, Wyeth Pharmaceuticals and Xoma. NR and AM have received payment for service on speakers' bureaus from Astra Zeneca, Bristol Myers and Squibb, Janssen Biologics BV, Roche and Wyeth/Pfizer. LO and SO have received consultancy fees from Novartis. IK-P has received consultancy fees from Novartis, SOBI Biovitrum, Roche, Abbot, Pfizer and research grants from LFB and SOBI Biovitrum. AS has received consultancy fees from Novartis and SOBI Biovitrum. HL and JF have received honoraria for meeting presentations from Novartis and SOBI Biovitrum. JK-D has received consultancy fees from Novartis, SOBI Biovitrum and Roche and research grants and speaker fees from Novartis. MH has received honoraria for meeting presentations from Novartis and Pfizer. MG has received consultancy fees and honoraria for meeting presentations from Novartis and SOBI Biovitrum.
-
Ethics approval Ethics approval was obtained from the ethical board of the G Gaslini Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.