Article Text

Abstract
Objective To determine the association between inflammatory markers and change in knee pain over 5 years.
Methods A total of 149 randomly selected subjects (mean 63 years, range 52–78; 46% female) was studied. Serum levels of high sensitivity C-reactive protein (hs-CRP), tumour necrosis factor alpha (TNF–α) and interleukin (IL)-6 were measured at baseline and 2.7 years later. Knee pain was recorded using the Western Ontario and McMasters osteoarthritis index questionnaire at baseline and 5 years later. Knee radiographic osteoarthritis of both knees was assessed at baseline, and knee bone marrow lesions, joint effusion and cartilage defects were determined using T1 or T2-weighted fat saturated MRI.
Results After adjustment for confounding variables, baseline hs-CRP was positively associated with change in total knee pain (β=0.33 per mg/l, p=0.032), as well as change in the pain at night in bed (β=0.12 per ml/pg, p=0.010) and while sitting/lying (β=0.12 per ml/pg, p=0.002). Change in hs-CRP was also associated with change in knee pain at night and when sitting/lying (both p<0.05). Baseline TNFα and IL-6 were associated with change in pain while standing (β=0.06 per ml/pg, p=0.033; β=0.16 per ml/pg, p=0.035, respectively), and change in TNFα was positively associated with change in total knee pain (β=0.66 ml/pg, p=0.020) and change in pain while standing (β=0.26 ml/pg, p=0.002). Adjustment for radiographic osteoarthritis or MRI-detected structural abnormalities led to no or minor attenuation of these associations.
Conclusion Systemic inflammation is an independent predictor of worsening knee pain over 5 years.
Statistics from Altmetric.com
Knee pain, often the most prominent and disabling symptom of knee osteoarthritis, is common among older adults. Almost half of older adults aged between 50 and 79 years have reported knee pain,1 and 25% of people over 55 years have persistent knee pain during a 1-year period.2 Knee pain is associated with body mass index (BMI) and knee structural changes such as cartilage defects,1 bone marrow lesions (BML),1 ,3 synovitis and joint effusion4,–,6 and osteophytes.7 The positive associations between synovitis/effusion and knee pain6 indicate that inflammation may play a role in knee pain genesis.
Inflammatory cytokines such as tumour necrosis factor alpha (TNFα), interleukin (IL)-1 and IL-6 can be produced by a variety of cells both within and without the joint.8,–,13 We14 ,15 and others16 reported that IL-6 and TNFα were associated with radiographic osteoarthritis and knee cartilage loss in middle-aged to older people with or without knee pain. C-reactive protein (CRP) is a marker of low-grade systemic inflammation and can be upregulated by IL-6,17 and high serum levels of high sensitivity C-reactive protein (hs-CRP) are present in early osteoarthritis18 ,19 and are associated with reduced cartilage volume.20 These findings suggest that inflammatory factors may play a role in structural changes in osteoarthritis.
Given that knee structural changes do not explain all knee pain,4 the associations of inflammatory factors with structural changes may not translate to their associations with knee pain. Indeed, a few cross-sectional studies have reported inconsistent associations between inflammatory markers and knee pain,21,–,23 so this area remains controversial, and more studies are necessary to identify the roles of inflammation in knee pain.24 In addition, subscales relating to pain during different activities may be independent and reflect different pain aetiologies.25 The aim of this study was, therefore, to determine the association between inflammatory markers and change in total knee pain and various subscales of knee pain over 5 years.
Materials and methods
Subjects
The study was carried out in southern Tasmania from March to August 2002. The follow-up study was conducted 2.7 years later (range 2.6–3.3 years), with a set of measures also taken at a second follow-up after 5 years (range 5.3–6.8 years; average 5.6 years). Subjects between the age of 50 and 79 years were selected randomly from the roll of electors in southern Tasmania (population 229 000) with an equal number of men and women. This study was conducted as part of the Tasmanian Older Adult Cohort Study, an ongoing, prospective, population-based study in 1100 subjects with an overall response rate of 57% at baseline, 82% retention for 3-year follow-up, and 69% retention for 5-year follow-up. The first 172 subjects were selected to perform the measurements of serum inflammatory markers at baseline and first follow-up. Knee pain was recorded at baseline and at the second follow-up for all subjects. At first follow-up, biomarker measurements were not performed in nine subjects due to insufficient serum sample, and 14 of the remainder were lost to the second follow-up, leaving 149 subjects. The study was approved by the Southern Tasmanian Health and Medical Human Research Ethics Committee, and written informed consent was obtained from all participants.
Anthropometrics and questionnaire
Height and weight were measured, and BMI was calculated as previously described.26
Serum inflammatory markers measurement
IL-6, TNFα and hs-CRP were measured from serum at baseline and then at the first follow-up as previously described.24 Samples with undetectable concentrations were assigned a value corresponding to the lower limit of detection of the assay (2 pg/ml for IL-6 (27%), 4.0 pg/ml (13%) for TNFα and 0.01 mg/l (22%) for hs-CRP). The coefficients of variation in our hands were 8% for IL-6, 6% for TNFα and 4.8% for hs-CRP.24
Changes in these markers were calculated as absolute change per annum.
Knee pain and x-ray assessment
Knee pain (walking on flat surface, going up/down stairs, at night in the bed, sitting/lying and standing upright) was assessed by self-administered questionnaire using the Western Ontario McMaster osteoarthritis index (WOMAC) with a 10-point scale from 0 (no pain) to 9 (most severe pain).27 Each component was summed to create a total pain (0–45) score. Prevalent knee pain was defined as a total score of 1 or greater. Change in knee pain was calculated as (follow-up value – baseline value) for each subscale as well as total pain. We have calculated the smallest statistically significant difference for the WOMAC knee pain score28 to be 0.9 for our population, so we defined an increase in pain as a change in score of 1 or greater.
All subjects had baseline radiographs scored for osteophytes and joint space narrowing (JSN) on a scale of 0–3 (0=normal and 3=severe) according to the Osteoarthritis Research Society International (OARSI) atlas, as previously described.26 The intraclass correlation coefficients for osteophytes were 0.99 and for JSN was 0.98. The presence of medial or lateral tibiofemoral JSN or osteophytes was defined as any score of 1 or greater in that compartment, and 1 or greater in either for whole tibiofemoral JSN or osteophytes. Grades of JSN and osteophytes were each summed across compartments within the knee for use in multivariable analysis.
Magnetic resonance imaging
MRI of the right knee was performed at baseline with a 1.5T whole-body magnetic resonance unit (Picker International, Uniontown, Ohio, USA), using a commercial transmit/receive extremity coil. Both a T1-weighted fat suppression three-dimensional gradient recalled and T2-weighted fat saturation three-dimensional fast spin echo acquisition were used, as previously described.26
Cartilage defects were assessed for each compartment using a 5-point scale as previously described,29 and were summed over the patella and medial and lateral tibia and femur to create a total score. BML were measured on the T2 MRI images using a 3-point grading system, as previously described,1 and summed similarly. The intraclass correlation coefficients for MRI measures of BML and cartilage defects were 0.80–1.00. Suprapatellar effusion was scored visually using the Boston–Leeds osteoarthritis knee score30 as either present (≥1) or absent on the baseline T2 MRI images, with κ=1.00.
Data analysis
With this sample size, this study had 80% power to detect a correlation of 0.2 between inflammatory markers and change in knee pain, with p<0.05. t Tests or χ2 tests (when appropriate) were used to compare means or proportions between those who increased in total pain and those who did not. Pearson's correlations with two-sided tests for significance were used to examine the associations between changes in each subscale of knee pain. Multivariable linear regression was used to examine the associations between inflammatory biomarkers and change in knee pain (total or by subscale), by including both baseline and change per annum values of either TNFα, IL-6 or CRP as the main predictors of change in knee pain. The associations were adjusted for age, sex, BMI and other potential confounding factors. To test for independence of associations to radiographic osteoarthritis or MRI-detected abnormalities, linear regressions were further adjusted for JSN and osteophytes or cartilage defects, BML and effusion. We also used multivariable logistic regression to determine the associations between inflammatory markers and increase in total knee pain using different cutpoints for knee pain increase (change ≥1 or change ≥3). A p value less than 0.05 (two-tailed) or a 95% CI not including the null point (for linear regression) was regarded as statistically significant. All statistical analyses were performed on PASW statistics (SPSS) version 18.0 for Windows. Two outlier (>30 pg/ml) values of IL-6 were excluded from analysis. Adjustments for multiple testing on regression results were undertaken using the Hochberg method.31
Results
Knee pain was prevalent in 45% of subjects. There were no significant differences in demographic factors, radiographic osteoarthritis and cartilage loss between the current cohort and the subjects who did not have serum markers measured (data not shown). The median level of IL-6 was 2.9 pg/ml, of TNFα was 7.3 pg/ml and of hs-CRP was 2.2 mg/l. In unadjusted analysis, serum levels of hs-CRP were positively associated with TNFα (r=0.17, p=0.02) but not with IL-6 (r=0.04, p=0.59), and TNFα was positively associated with IL-6 (r=0.27, p<0.001). Baseline levels of biomarkers were not significantly associated with baseline total knee pain (all p>0.05). Radiographic osteoarthritis was prevalent in 61% of subjects. Effusion was present in 12% of subjects, BML were present in 37% and cartilage defects were present in 49%. Serum levels of biomarkers were not significantly different between those with or without effusion, BML or cartilage defects (all p≥0.05). In univariable analysis, the total defect score was associated with change in total knee pain (β=0.212, p=0.013) and knee pain while lying in bed (β=0.058, p=0.014); prevalent effusion was associated with change in knee pain while lying in bed (β=0.791, p=0.031).
The distribution of change in knee pain is shown in figure 1. Most subjects (55%) had no pain at baseline. Of all subjects, 45% did not change in pain status from baseline to follow-up, 23% had a total pain increase of 1 unit or more and 10% had a pain increase of 3 units or more. The characteristics of participants are presented in table 1. Those whose total knee pain increased over 5 years had, compared with the others, a significantly higher prevalence of osteophytes in the right, left and whole tibiofemoral compartments, as well as a higher prevalence of any JSN in the whole compartment. There were no significant differences between these two groups in all other characteristics. Table 2 shows the correlations between changes in subscales of knee pain. The correlations varied from 0.361 to 0.738, with the strongest being between change in pain while sitting and change in pain in bed at night (r=0.738).
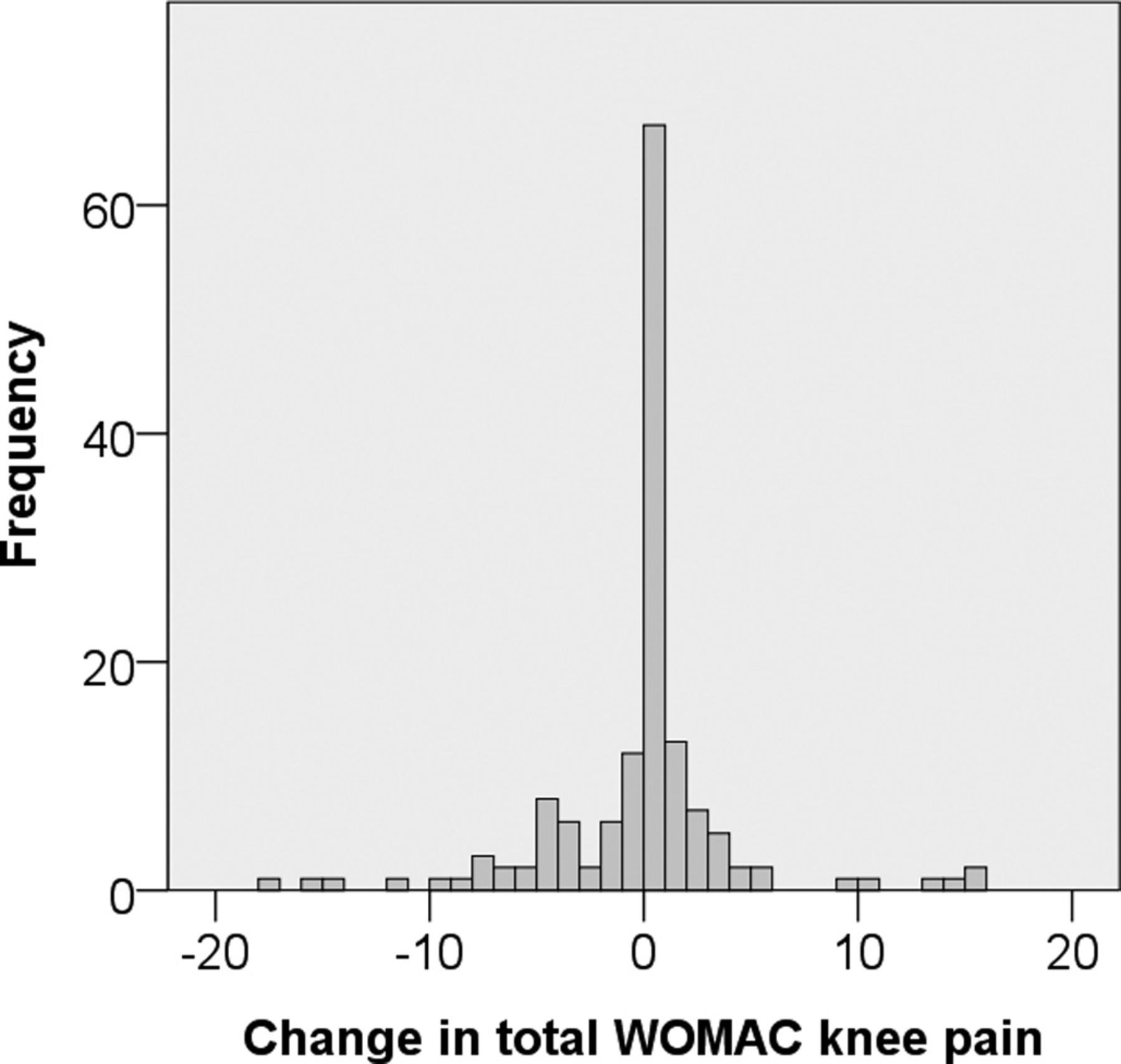
Distribution of change in total Western Ontario and McMasters osteoarthritis index (WOMAC) knee pain.
Characteristics of participants
Correlations between changes in pain scales
In logistic regression analyses, baseline and change in hs-CRP were each associated with an increase in total knee pain of 3 units or more (figure 2), but this was not apparent in analyses for single unit increase in total knee pain (see supplementary figure S1, available online only). Baseline hs-CRP was significantly and positively associated with change in total knee pain (p=0.032) after adjustment for potential confounders, while both baseline and change in hs-CRP were associated with change in the subscales for pain while at night in bed (p=0.010 and p=0.018, respectively) and sitting/lying (p=0.002 and p=0.013, respectively) in multivariable analyses (table 3). The associations between hs-CRP and knee pain remained significant after further adjustment for radiographic features (table 3) or cartilage defects/joint effusion (data not shown); but the association between baseline hs-CRP and change in total pain became of borderline significance (effect size decreased by 11%) after adjustment for BML.

{kind=link}
{kind=link}
OR for multivariable associations between either baseline or change in biomarkers and increase (change ≥3) in Western Ontario and McMasters osteoarthritis index total knee pain. Adjusted for age, sex, body mass index, baseline pain, current smoking, asthma, bronchitis, diabetes, heart disease and steps per day. Bars denote CI. Bold denotes significant association. hs-CRP, high-sensitivity C-reactive protein; IL-6, interleukin 6; TNFα, tumour necrosis factor alpha.
Associations between baseline hs-CRP, change in hs-CRP over 2.5 years and change in knee pain over 5 years
Baseline and change in TNFα were each associated with an increase in total pain as defined by a change of either 1 or greater (see supplementary figure S1, available online only) or 3 or greater (figure 2). In multivariable linear regression analyses, baseline levels of TNFα were positively associated with change in pain while standing (p=0.033) but not with change in total knee pain and other subscales of knee pain (table 4). Change per annum in TNFα was associated with change in total knee pain (p=0.020) and knee pain while standing (p=0.002), but not with any other pain subscales (table 4). After further adjustment for radiographic osteoarthritis, the association between change in TNFα and change in total knee pain decreased in magnitude by 15%, and the association between baseline TNFα and change in standing knee pain decreased in magnitude by 17%, with both becoming of borderline significance (p=0.051 and p=0.085, respectively). However, after adjustment for cartilage defects, BML and joint effusion, all three significant associations remained unchanged (all p<0.05; data not shown).
Associations between baseline TNFa, change in TNFa over 2.5 years and change in knee pain over 5 years
Neither baseline nor change per annum in IL-6 was associated with change in total knee pain (table 5) or a defined increase in total knee pain (figure 2, supplementary figure S1, available online only). However, baseline IL-6 levels were positively associated with change in the standing subscale of pain after adjustment for potential confounders (p=0.035). This significant association persisted after further adjustment for radiographic features (table 5), or cartilage defects, BML and joint effusion (data not shown).
Associations between baseline IL-6, change in IL-6 over 2.5 years and change in knee pain over 5 years
After adjustments for multiple testing using the Hochberg approach over tables 3–5, only the associations for change in TNFα predicting change in knee pain while standing and baseline hs-CRP predicting change in knee pain while sitting remained significant. Results remained unchanged after the exclusion of subjects with radiographic osteoarthritis.
Discussion
This study is the first to examine the associations between levels of inflammatory biomarkers and changes in knee pain in community-based older adults over a large interval of time. Our major findings were that, over 5 years, baseline and change in hs-CRP and TNFα over 2.7 years were associated with increases in knee pain as assessed by the total WOMAC score. While hs-CRP was associated with increased knee pain when lying in bed at night and while sitting or lying, TNFα and IL-6 predicted greater change in knee pain while standing.
Currently, there has been limited investigation into the role of inflammatory markers in knee pain severity, development or progression. Several cross-sectional studies have found inconsistent associations between knee pain and IL-6, TNFα and CRP.21,–,23 ,32 In a longitudinal study, Pelletier et al33 reported that baseline CRP, but not IL-6, predicted worsening knee pain and function over 2 years in a sample of 161 subjects with osteoarthritis, but this association was not adjusted for potential confounders. These inconsistencies are most likely due to variations in sample size, study population and design, and/or, if any, a short period of follow-up.
We reported mostly consistent associations between baseline hs-CRP, change in hs-CRP over 2.7 years, and change/increase in total knee pain over 5 years in older adults. The relationship between hs-CRP and total knee pain change seemed to be mostly driven through the subscales of pain in bed and sitting, with which both baseline and change over 2.7 years in hs-CRP were associated. Baseline and/or change in TNFα were associated with increase/change in total knee pain and change in knee pain while standing. A similar association was also found between baseline IL-6 and change in knee pain while standing. These results suggest different inflammatory markers may play roles in the development and progression of different subscales of knee pain in older adults. There is evidence supporting the use of the WOMAC pain subscale scores as independent outcomes, instead of the total summed pain score.25 In particular, results from our study suggest pain while sitting shares a strong correlation with pain while lying in bed at night, as does pain while walking on a flat surface with pain while walking on stairs, with knee pain standing sharing some relationships with both clusters of knee pain. The associations between inflammatory markers and change in the subscale of knee pain scores we observed in this study largely support the clusters of knee pain. Our multivariable associations showed the same predictor (hs-CRP) for knee pain while in bed and sitting or lying in bed at night, and other predictors (TNFα and IL-6) for knee pain while standing. The fact that we did not find significant results for knee pain while walking or climbing stairs suggests that pain of those subtypes may be more related to other mechanisms than inflammatory factors; mechanical loading might be more relevant with these symptomatic outcomes.
The consistent results for hs-CRP as a predictor of change in knee pain while in bed at night and while sitting or lying suggests that the contribution of hs-CRP to knee pain is specific to sedentary non-weight-bearing pain outcomes. CRP reflects systemic inflammatory effects,32 possibly independent of adiposity,34 for which our analysis was adjusted. However, Kerkhof et al35 argued against CRP representing the influence of systemic inflammation on the knee, and levels of CRP may also simply reflect the downstream effects of cytokine release in various tissues, including synovium36 and subchondral bone. BML are a common painful feature of knees in older subjects,1 and can vary with time.3 Intraosseous pressure from BML is a possible cause of knee pain37 that may explain pain in stationary non-load-bearing positions, and serum hs-CRP levels may reflect an inflammatory component to BML. Our results for hs-CRP as a predictor of total knee pain change remained significant after adjustment for radiographic osteoarthritis, cartilage defects and effusion, but became of borderline significance after adjustment for BML. This suggests that BML may be a structural factor partly mediating the association between hs-CRP and total knee pain change. However, the change in estimates was small and BML seem not to mediate the association between hs-CRP and change in pain while in bed at night and while sitting or lying, and the discordance for these is unknown.
Cartilage lesions may be an important source of pain,1 ,38 and there is some evidence for inflammation predicting cartilage loss.4 ,14 TNFα can stimulate chondrocyte production of matrix metalloproteinases.39 ,40 Increased TNFα levels may upregulate the production of IL-6 by chondrocytes through IL-1 mediation,41 ,42 in which IL-6 may have deleterious effects through the downregulation of collagen synthesis.43 The fact that the associations between TNFα, IL-6 and knee pain changes remained significant after adjustment for cartilage lesions and other structural abnormalities (BML and effusion) suggests that these structural changes may not be of primary importance in the relationship. In contrast, the associations between TNFα and change in knee pain decreased in magnitude after adjustment for radiographic changes, suggesting radiographic changes may be partly responsible for the effect of TNFα on change in knee pain.
Synovitis4,–,6 is a likely explanation for our results showing associations between inflammatory markers and change in knee pain over time. We reported that cytokine levels were not significantly different between the subjects with and without effusion, and significant associations between TNFα, IL-6, hs-CRP and knee pain remained after adjustment for effusion, suggesting that the associations we observed may be independent of effusion-related inflammation. However, the use of effusion as a surrogate of synovitis (the correlation between effusion and synovitis was minimal)44 limits our ability to rule out synovitis acting as a mediator between circulating inflammatory markers and changes in knee pain.
Aside from structural changes, pro-inflammatory cytokines may also contribute to pain through inducing hypersensitivity.45 ,46 While TNFα can induce a long-lasting sensitisation of joint nociceptors to mechanical stimuli and thus can induce long-lasting mechanical hyperalgesia in knee joints,47 a single injection of IL-6 into a normal knee joint can also cause a slowly rising but persistent sensitisation of C fibres to mechanical stimulation of the joint.48 Such effects could explain our results with serum levels of TNFα and IL-6 predicting standing pain increase after adjustment for structural abnormalities and effusion.
Our study has several potential limitations. The sample size was modest (N=149). It is possible that with a larger sample we may have been able to detect even more significant associations. In addition, the levels of inflammatory biomarkers were measured in serum, as opposed to synovial fluid, which do not allow us to detect local autocrine or paracrine effects. However, serum CRP has been shown to correlate well with CRP in synovial fluid in patients with osteoarthritis.49 While we performed adjustment for the BMI of subjects, we cannot completely exclude the possibility that the associations of serum measures with knee pain could be affected by adipose tissue. We found the associations between change in TNFα and change in pain while standing and between baseline hs-CRP and change in pain while sitting both passed the Hochberg correction, suggesting that these can be considered true positive results. While caution must be exercised when interpreting significant results that did not pass correction, those that did not pass showed consistent associations of hs-CRP with change in both at night and sitting knee pain, and consistent associations of both IL-6 and TNFα with change in standing knee pain, indicating that these findings are biologically plausible, and may not be false positives.
Conclusion
These results suggest that systemic inflammation is an independent predictor of worsening knee pain over 5 years, and anti-inflammatory therapy may reduce knee pain in patients with osteoarthritis. The underlying mechanisms largely remain uncertain at this time.
Acknowledgments
Special thanks go to the subjects who made this study possible. The roles of C Boon and P Boon in collecting data, and of V Parameswaran and J Burgess in measuring biomarkers are gratefully acknowledged.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Funding This study received funding from the National Health and Medical Research Council of Australia. CD is a recipient of an ARC future fellowship, and GJ is a recipient of a NHMRC practitioner fellowship.
-
Ethics approval The study was approved by the Southern Tasmanian Health and Medical Human Research Ethics Committee.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.