Article Text

Abstract
Objectives To test the American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) and disease activity score in 44 and 28 joints (DAS, DAS28) definitions of remission in early rheumatoid arthritis (RA), against disability and ultrasound-detectable synovitis.
Methods In an observational study of early RA patients, remission rates were determined and compared in 166 patients. The remission definitions included the simplified disease activity index (SDAI≤3.3), ACR/EULAR (categorical), DAS28 (<2.6) and DAS (<1.6). The health assessment questionnaire (HAQ) was completed at baseline and 12 months, power Doppler-positive synovitis (PDPS) was assessed at baseline, 6 and 12 months. Cross-sectionally, the outcomes were low functional disability (HAQ≤0.5) or absent PDPS in all joints, while longitudinally the outcomes were stable low functional disability and persistent absent PDPS in all joints.
Results At baseline, 33.7% of patients achieved DAS28 remission, 43.37% DAS remission, 16.8% SDAI remission, 13.8% ACR/EULAR remission. DAS28, SDAI and ACR/EULAR remission was cross-sectionally associated with low functional disability and absent PDPS. All definitions were longitudinally associated with low functional disability: positive likelihood ratios (LR+) of 3.24 for DAS28, 2.14 for DAS, 4.86 for SDAI, 5.67 for ACR/EULAR criteria, and with absent PDPS for DAS28 (LR+ 1.66), SDAI (LR+ 6.46), ACR/EULAR (LR+ 5.07).
Conclusions The new remission definitions confirmed their validity in an observational setting and identify patients with better disease control.
- Rheumatoid Arthritis
- DAS28
- Ultrasonography
Statistics from Altmetric.com
Introduction
Early intervention with disease-modifying antirheumatic drugs (DMARD) and new therapies have improved the management of rheumatoid arthritis (RA), making clinical remission a realistic target.1 ,2 Several definitions of remission have been proposed, with a great variability in their selectivity and the possibility of subclinical imaging detectable disease activity, leading to radiographic progression.3 ,4
The American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) proposed a new definition of remission for trials.5 Remission occurs if the results of swollen and tender joint counts based on 28 joints, patient's global assessment (PtGA), C-reactive protein (CRP) are all 1 or less or simplified disease activity index (SDAI) is 3.3 or less. These definitions were tested against radiographic progression and disability data from different trials, and in external cohorts, proving to be effective against disability, but with possible radiographic progression.6 ,7
Although ultrasonography was not included in the definition, it is considered more sensitive than clinical examination in detecting subclinical synovitis in RA, especially when patients are in remission.8 ,9 The persistence of power Doppler-positive synovitis (PDPS) in remission identifies patients at higher risk of relapse and radiographic progression.10 ,11 In one study patients in SDAI remission showed a lower rate of PDPS compared to those in disease activity score in 28 joints (DAS28) remission, but in another study the prevalence of PDPS in patients fulfilling ACR/EULAR and DAS28 remission was similar.12 ,13
The aim of this study was to assess cross-sectionally the association between remission based on different definitions and the absence of functional disability or absence of subclinical synovitis, and to determine the predictive ability of these definitions, adopting the same approach used for their development, on low stable functional disability and persistent absence of PDPS over 1 year.
Patients and methods
Patient recruitment and treatment
Patients from an inception-based cohort study at the Early Arthritis Clinic of Pavia University Hospital, Italy, were asked to participate in this study. Referral criteria and the detailed therapeutic protocol of the original study are reported elsewhere (figure 1).10 In summary, patients treated with non-biological DMARD, fulfilling the 1987 RA classification criteria 1 year after starting treatment, were enrolled. Out of 189 patients with a primary diagnosis of RA, 29 were lost to follow-up and 21 started tumour necrosis factor α blockers and were excluded from the current study. Of the 78 patients with undifferentiated polyarthritis who started treatment, 27 fulfilled the ACR criteria for RA and were also included in this study. Therefore, after 1 year 166 fulfilled the 1987 ACR criteria for RA and these patients were included in the current 1-year follow-up study (figure 1).14 Regular clinical monitoring visits meant clinical and laboratory findings were available every 3 months until the end of the follow-up. This study was approved by the ethics committee of the IRCCS Policlinico San Matteo Foundation of Pavia, Italy, and all patients gave written consent.

Patient recruitment and design of the study. RA, rheumatoid arthritis; UPA, undifferentiated polyarthritis.
Patient assessment
At baseline and each visit, the 28 tender and swollen joint counts, PtGA, evaluator's global assessment, global health assessment, erythrocyte sedimentation rate (ESR) and CRP were assessed. The disease activity score (DAS) and DAS28 were calculated based on ESR. Clinical remission was defined as DAS28<2.6, DAS<2.0 (a cut-off evaluated during the development of the new definitions), DAS<1.6, SDAI≤3.3 or ACR/EULAR remission criteria (28 tender and swollen joint counts, PtGA and CRP all ≤1). The Italian health assessment questionnaire (HAQ) was completed at baseline and each visit until the end of follow-up.15
Ultrasound examination
Ultrasound examination was performed at baseline, 6 and 12 months by a single experienced operator, unaware of clinical data, using a Logiq 9 scanner (General Electrics Medical Systems, Milwaukee, Wisconsin, USA) with a multifrequency linear array transducer (8–15 MHz), according to the EULAR guidelines.16 Bilateral wrist and metacarpophalangeal joints (1–5) were assessed (see supplementary data, available online only).
Outcomes
In the cross-sectional analyses the functional outcome was defined as HAQ≤0.5 and the ultrasound outcome was the absence of PDPS in all examined joints.17 In longitudinal analyses, positive functional outcome was defined as a change in HAQ≤0 between baseline and 1 year, and persistent HAQ≤0.5 during the follow-up, as applied to develop the new definition of remission.5 Ultrasound outcome was the persistent absence of PDPS in all joints at baseline, +6 and +12 months.
Statistical analysis
Summary statistics of mean and SD or median and IQR are presented for continuous variables, when appropriate. Absolute and relative frequencies are presented for categorical variables. Unweighted κ statistics were used to analyse the concordance between criteria. Cross-sectional associations between remission, disability and ultrasound were tested using the χ2 test.
Longitudinal analyses were performed calculating the positive likelihood ratios (LR+) and presented along with exact 95% CI. For all analysis, data were first analysed including all patients. An analysis on complete data was performed afterwards. All the analyses were conducted using Stata V.11.
Results
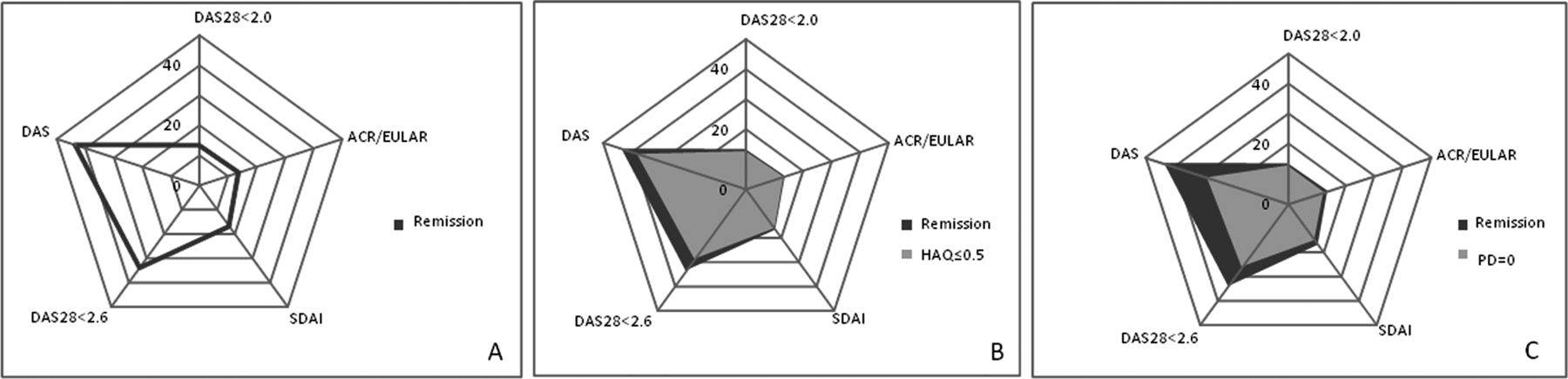
A total of 166 patients (73% female) were included (table 1). At baseline (after 12 months of consecutive DMARD therapy), median (IQR) disease duration was 16 months (15–18), median (IQR) age 60 (50–72) years and 68/166 (41%) of the patients were rheumatoid factor positive (53% before treatment). All but one patient were taking DMARDs, 143/166 (86.1%) were taking methotrexate. DAS28 was <2.6 in 56/166 (33.7%) patients, DAS28<2.0 in 22/166 (13.2%), DAS<1.6 in 72/166 (43.3%), SDAI remission in 28/166 (16.8%) and ACR/EULAR categorical definition in 23/166 (13.8%) patients. The categorical criterion and SDAI showed a high agreement (95.8%), with a kappa of 0.83 (p<0.001). Overall, 113/166 (68.5%) patients had an HAQ≤0.5, and PDPS was absent in 107/166 (64.5%) patients. At baseline, all remission criteria were associated with low functional disability and absence of PDPS (figure 2, see supplementary table S1, available online only), compared to patients with active disease, except for DAS.
Patient characteristics at the beginning of the study, after 12 months of DMARD treatment

{kind=link}
{kind=link}
Cross-sectional association between remission criteria and functional/ultrasonographic outcomes. (A) Prevalence of clinical remission according to different criteria in our population (percentage of patients in remission over total population: dark grey line). (B) Cross-sectional prevalence of patients in remission having low functional disability (dark grey area: percentage of patients in remission over total population; light grey area: percentage of patients in remission with low functional disability). All tested remission criteria were significantly associated with health assessment questionnaire (HAQ) of 0.5 or less (p<0.05). (C) Prevalence of absent power Doppler-positive synovitis (PDPS) in patients in remission (dark grey area: percentage of patients in remission over total population; light grey area: percentage of patients in remission with absent PDPS). All criteria were significantly associated with the absence of PDPS (p<0.05), except disease activity score (DAS). ACR/EULAR, American College of Rheumatology/European League Against Rheumatism; DAS28, disease activity score in 28 joints; SDAI, simplified disease activity index.
Longitudinal analysis
One hundred and forty-one out of 166 patients (84.9%) completed the 1-year follow-up, with no significant differences in demographic and clinical characteristics compared to those who were lost to follow-up. One hundred and thirty-four out of 141 patients (80.7%) had complete baseline and follow-up functional outcome data and 124/141 (74.6%) patients had complete ultrasound baseline and follow-up data. After 1 year, a total of 74/134 (55.2%) patients had low functional disability and 52/124 (41.9%) had absent PDPS. Clinical remission at baseline according to all examined criteria was associated with stable and low HAQ at 12 months (table 2).
Predictive validity of different remission definitions for no functional disability and absence of PDPS over 1 year
Some of the remission criteria had a good predictive ability for the absence of PDPS: LR+ were 1.66 (1.03, 2.66) for DAS28<2.6, 2.53 (1.00, 6.42) for DAS28<2.0, 1.04 (0.71, 1.53) for DAS<1.6, 6.46 (1.95, 21.34) for SDAI and 5.07 (1.49, 17.29) with more restrictive criteria (SDAI and ACR/EULAR) resulting in more suppression of PDPS (table 2).
Discussion
The remission rates in our population were similar to other early RA cohorts followed with a treat-to-target strategy. As expected, ACR/EULAR definitions (categorical or SDAI) classified a smaller number of patients in clinical remission, with high agreement.
Being in remission was associated with low disability and absent PDPS (except with DAS). The mismatch between the joint count in the DAS and in ultrasound might have led to patients with prevalent hand involvement with detectable PDPS and more PDPS longitudinally being considered in remission. Although SDAI remission was more frequently associated with absent PDPS than DAS28 in one study, another study showed a similar prevalence of negative power Doppler in patients achieving either ACR/EULAR remission or DAS28 remission.12 ,13 In our study, more patients in ACR/EULAR remission had absent PDPS compared to patients with DAS28<2.6. A longer disease duration and a large proportion of patients on biological agents in the other study might explain these differences. To test the predictive ability of the new definitions, we used the same definition for low and stable functional disability applied for their development. Achieving clinical remission, regardless of the criterion used to define remission, leads to higher rates of low functional disability compared to patients not in remission.
As a surrogate marker of the suppression of synovitis, we chose the absence of PDPS during follow-up. The ACR/EULAR definition was associated with persistent absence of PDPS, while DAS28<2.6 showed only a marginally significant effect on PDPS, and the remaining criteria did not show a statistically significant effect. As PDPS relates to erosive progression, this may represent the associative effect of different definitions of remission on 1-year radiographic progression.18 Nevertheless, in a 5-year follow-up study radiographic deterioration has been reported even in patients satisfying the new definitions, probably due to remitting-relapsing disease.7
One of the strengths of this study is the evaluation of a uniform cohort of early RA patients experiencing incident remission on a standardised therapeutic protocol. Patients on biological agents or starting biological agents during the follow-up were not included due to the possible effect modification on ultrasound.19 The exclusion of this subgroup inflates the rates of baseline remission, but makes its assessment more reliable using ultrasound as an outcome. A distinct prospective study on this subgroup of patients has been planned.
The small number of patients fulfilling the more stringent criteria affects the precision of our estimates. Multiple comparisons have been applied to small groups, but even with a conservative estimate according to Bonferroni's correction taking as significant a p value less than 0.005, the effect of SDAI and ACR/EULAR definitions is still significant.
Our study confirms the validity of the new definitions in an observational setting. Patients fulfilling the new criteria have less synovitis and disability; these better outcomes can be sustained over 12 months. However, these criteria exclude many patients with a virtual absence of the risk of developing functional impairment. Therefore, the new definition seems suitable to identify patients who might benefit from decreasing treatment, while DAS28 remission might still be indicated as a therapeutic target.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors GS contributed to study design, collected data, contributed to data interpretation and drafted the article. CAS contributed to study design, performed statistical analysis, contributed to data interpretation and revised the article. SMMV contributed to data interpretation and revised the article. CM and RC contributed to study concept and design and revised the article. All authors approved the final version to be published.
-
Competing interests None.
-
Ethics approval This study was approved by the ethics committee of the IRCCS Policlinico San Matteo Foundation of Pavia, Italy.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.