Article Text

Abstract
Introduction The previously reported randomised controlled trial of a consensus regimen of pulse cyclophosphamide suggested that it was as effective as a daily oral (DO) cyclophosphamide for remission induction of antineutrophil cytoplasm autoantibodies-associated systemic vasculitis when both were combined with the same glucocorticoid protocol (CYCLOPS study (Randomised trial of daily oral versus pulse Cyclophosphamide as therapy for ANCA-associated Systemic Vasculitis published de groot K, harper L et al Ann Int Med 2009)). The study had limited power to detect a difference in relapse. This study describes the long-term outcomes of patients in the CYCLOPS study.
Methods Long-term outcomes were ascertained retrospectively from 148 patients previously recruited to the CYCLOPS Trial. Data on survival, relapse, immunosuppressive treatment, cancer incidence, bone fractures, thromboembolic disease and cardiovascular morbidity were collected from physician records retrospectively. All patients were analysed according to the group to which they were randomised.
Results Median duration of follow-up was 4.3 years (IQR, 2.95–5.44 years). There was no difference in survival between the two limbs (p=0.92). Fifteen (20.8%) DO and 30 (39.5%) pulse patients had at least one relapse. The risk of relapse was significantly lower in the DO limb than the pulse limb (HR=0.50, 95% CI 0.26 to 0.93; p=0.029). Despite the increased risk of relapse in pulse-treated patients, there was no difference in renal function at study end (p=0.82). There were no differences in adverse events between the treatment limbs.
Discussion Pulse cyclophosphamide is associated with a higher relapse risk than DO cyclophosphamide. However, this is not associated with increased mortality or long-term morbidity. Although the study was retrospective, data was returned in 90% of patients from the original trial.
Statistics from Altmetric.com
Introduction
Granulomatosis with polyangiitis, formerly known as Wegener's granulomatosis,1 microscopic polyangiitis (MPA) and the renal-limited variant of MPA are associated with antineutrophil cytoplasm autoantibodies (ANCAs) and are often referred to, collectively, as ANCA-associated vasculitis. Treatment for these diseases is by immunosuppression. The introduction of immunosuppression with cyclophosphamide and glucocorticoids in the 1960s led to a dramatic improvement in prognosis, with 78% of patients achieving 5-year survival compared with a mortality of 80% at 1 year in untreated patients.2 However, these advances were achieved at the cost of treatment-related toxicity such as haemorrhagic cystitis, bladder cancer, lymphoproliferative disease, myelodysplasia and infertility due to the cumulative exposure to cyclophosphamide.3
Most trials performed in the last 20 years have aimed to minimise the amount of cyclophosphamide administered to reduce toxicity.4 Previous studies have suggested that pulse cyclophosphamide regimens are safe and impose lower cumulative cyclophosphamide exposure than daily oral (DO) cyclophosphamide regimens. However, this may be at the expense of an increased relapse rate.5 The European Vasculitis Study Group (EUVAS) undertook a controlled trial of 149 patients randomised to receive a consensus-designed pulse cyclophosphamide regimen or a DO cyclophosphamide regimen. The pulse cyclophosphamide regimen allowed administration of half the cumulative cyclophosphamide dose of the DO regimen but used the same glucocorticoid dose. The study suggested that there was no difference in remission rates for generalised ANCA-associated vasculitis at 18 months follow-up.6 This study had limited power to assess the effect of induction with pulse cyclophosphamide compared to DO on relapse rates and other longer-term events in patients with ANCA-associated vasculitis.
This study describes the long-term patient survival and relapse rates of patients recruited to the EUVAS study, investigating pulse versus DO cyclophosphamide. We also investigated in this long-term study whether there were differences in the renal function, immunosuppression use and adverse events between the two limbs.
Methods
Study population
One hundred and forty nine patients participated in the initial study with 18 months follow-up, which has been published in full previously.6 In brief, patients were recruited between 1998 and 2002 from 42 hospitals in 13 European countries and Mexico. Patients were eligible if they had a new diagnosis of granulomatosis with polyangiitis or MPA. The diagnosis was based on a clinical presentation compatible with ANCA-associated vasculitis and substantiated by positive ANCA serology and/or histology. Patients were excluded if they had a coexistent multisystem autoimmune condition, concurrent malignancy, active infection, pregnancy or aged below 18 or above 80 years. Patients in the pulse limb (n=76) of the study received three intravenous pulses of cyclophosphamide (15 mg/kg) given 2 weeks apart, followed by pulses at 3-week intervals (15 mg/kg intravenously or 5 mg/kg orally on three consecutive days at the physician's discretion) until remission and, then, for another 3 months. The DO cyclophosphamide group (n=72) received cyclophosphamide (2 mg/kg per day) until remission, followed by 1.5 mg/kg per day for another 3 months. Dose was reduced for age and renal function.
Both groups continued the cyclophosphamide regimens for 3 months after remission, after which, all patients received azathioprine (2 mg/kg per day orally) until month 18 for remission maintenance. Both groups also received prednisolone (1 mg/kg orally) tapered to 12.5 mg at the end of month 3 and to 5 mg at the end of the study (month 18). At the end of the study, further treatment was left to the treating physician's discretion (see reference number 6 for full treatment protocol details).
The primary end point was time to remission and defined as absence of clinical disease activity using Birmingham Vasculitis Activity Score BVAS.
Long-term follow-up
In order to determine long-term survival, participating physicians completed standardised data abstraction forms. This study was performed in accordance with the 1964 Declaration of Helsinki and subsequent amendments, and ethical approval was obtained by national and local ethics committees in accordance with national legislation. Data on survival, renal survival, relapse rate, immunosuppressive treatment, malignancy, venous thrombotic events and cardiovascular and cerebrovascular morbidity were recorded. Renal function, as measured by creatinine, was recorded at 5 years from trial entry and at last visit. Local investigators were asked to provide information regarding the cause of death and contributing factors. They were also asked to rate separately the likelihood that active vasculitis, immunosuppression or sepsis contributed to death on a scale of 0 (not related) to 5 (definite). Two authors (KW and OF) independently categorised the cause of death as being directly attributable or contributed to by vasculitis, infection, malignancy, cardiovascular, miscellaneous and unknown. In case of disagreement, a third author (DJ) adjudicated. Replies were collected from September 2004 until January 2007. Local investigators were not asked to classify relapses as major or minor. The long-term survival outcomes of all EUVAS trials have been published.7
Statistics
One patient from the DO limb was excluded from this study due to a later diagnosis of Churg–Strauss syndrome. All other patients were analysed according to the group to which they were randomised. Kaplan–Meier curves were plotted to visually assess between-group differences, and Cox proportional hazards regression was used to estimate treatment effects expressed as HR with 95% CI. The proportional hazards assumption was confirmed using log minus log plot of the cumulative survival estimates. For analyses in which first relapse was the outcome, patients were censored at last follow-up or death. For analyses in which death was the outcome, patients were censored at last follow-up. For those without long-term follow-up data, patients were censored at last follow-up in the original trial.
A priori, we hypothesised that pulse cyclophosphamide may have a different effect on the long-term relapses in patients at higher baseline risk of relapse due to the presence of antiproteinase 3 antibodies (PR3-ANCA). We therefore conducted a multivariable analysis of PR3-ANCA status and trial limb. We excluded statistical interaction between PR3-ANCA status and trial limb before conducting the multivariable analysis. Between-group differences in continuous parameters were assessed using the Mann–Whitney U test and expressed as median and IQR. For categorical variables, Fisher's exact test or χ2 test, as appropriate, were used.
A p value of <0.05 was considered significant for all analyses, and no adjustments for multiple testing were made. We used SPSS for Windows V.17 for all statistical analyses.
Results
One hundred and forty nine patients participated in the original trial, 76 patients in the pulse limb and 72 patients in the DO limb. Of these, 134 patients had data available in the long-term follow-up study, seven patients from the DO limb and seven from the pulse limb were missing at long-term follow-up, and one patient with Churg–Strauss syndrome was excluded. Of those patients in whom long-term outcome data were not returned, four were withdrawn during the original trial follow-up period. The median duration of follow-up was 4.3 years (IQR, 2.95–5.44 years).
Survival
Twelve patients in the DO and 13 patients in the pulse limb died during the follow-up, of whom eight in the DO and five in the pulse limb died during the 18 months follow-up of the original trial (figure 1). The median time to death was 2.23 years (IQR, 0.32–3.13). There was no significant difference in survival between the two limbs (figure 1 HR=1.04, 95% CI 0.47 to 2.29, p=0.92). Causes of death in the DO limb included active vasculitis (three patients), sepsis,4 malignancy,1 pulmonary fibrosis,2 gastrointestinal haemorrhage1 and coronary artery disease.1 In the pulse limb, deaths included active vasculitis,1 sepsis,3 cardiac causes,4 ruptured aortic aneurysm,1 malignancy,2 bowel perforation1 and unknown cause.1

Patient survival according to treatment allocation. There was no significant difference in mortality risk between patients randomised to pulse cyclophsophamide or daily oral (DO) treatment.
Relapse
Fifteen (20.8%) DO patients and 30 (39.5%) pulse patients had at least one relapse. During follow-up, there were a total of 54 relapses (12 renal) in the pulse limb and 21 relapses (10 renal) in the DO limb. In Cox regression analysis, the risk of relapse was significantly lower in the DO limb than in the pulse limb (HR=0.50, 95% CI 0.26 to 0.93; p=0.029) (figure 2). The relapse rate was 0.08/patient-year (95% CI 0.05 to 0.12) in the DO limb compared with 0.18/patient-year (CI 0.13 to 0.21) in the pulse limb (p=0.001). There were no differences in the treatment of relapse between the two treatment limbs.

Relapse-free survival in the two treatment arms. Using Kaplan–Meier survival analysis, there was a significantly increased risk of relapse during follow-up in patients randomised to pulse cyclophsophamide rather than daily oral (DO) treatment (p=0.029).
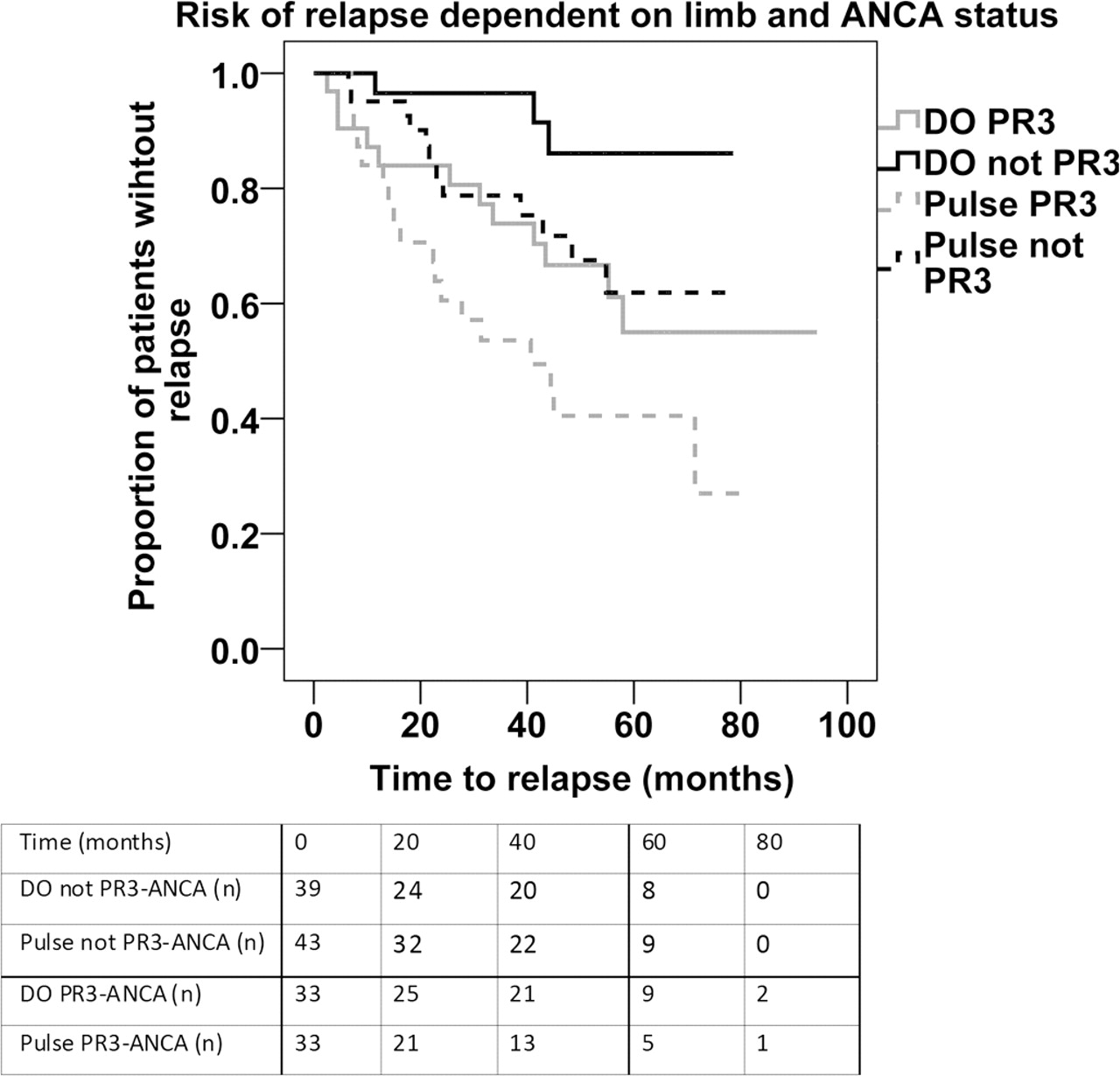
In a multivariable analysis including PR3-ANCA status and trial limb, both independently affected the risk of relapse (table 1, figure 3).

{kind=link}
{kind=link}
{kind=link}
Risk of relapse defined by PR3-ANCA status and trial treatment limb. In the multivariable analysis, trial limb and PR3-ANCA status were independent risk factors for relapse. The biological interaction between the two factors can be seen here in the stratification of risk of relapse. PR3-ANCA positive patients receiving pulse treatment had the highest risk of relapse, and daily oral (DO) treated patients who were not PR3-ANCA had the lowest risk of relapse. Those patients who were not PR3-ANCA and treated with pulse treatment and DO treated patients who were PR3-ANCA positive had an intermediate risk of relapse. PR3-ANCA, antiproteinase 3 antibodies
Factors associated with relapse in the multivariable analysis
Renal function
Despite an increased risk of relapse, there was no significant difference in renal function at last follow-up or end-stage renal failure (ESRF) between the two limbs. Ten (13%) pulse patients and eight (11%) DO patients developed ESRF. Eighty-three (42 pulse and 41 DO) patients did not have ESRF and had data on renal function available at last visit; in these patients, there was no difference in median creatinine at last follow-up (pulse limb, 117 (89–185) µmol/l; DO limb, 117 (105–144) µmol/l; p=0.92) (excluded from this analysis are 18 patients who developed ESRF, 14 patients who had no data abstraction forms returned and 32 patients who had no creatinine recorded at last visit).
Duration of immunosuppression
All patients had immunosuppression according to the trial protocol up to 18 months, beyond this, immunosuppression was left to the discretion of the investigator. Two patients had missing data on immunosuppression at the time of last visit. The 14 patients who did not return the questionnaires were excluded from the analysis. There was no difference in the median duration of steroid or antiproliferative agents beyond the end of the study between the two limbs (table 2). At 25 months, 36 DO and 44 pulse group patients were receiving azathioprine or an alternative immunosuppressive agent, and 42 DO and 40 pulse group patients were receiving steroids, respectively. At 48 months, this had reduced to 16 patients in the DO and 17 patients in the pulse group who are receiving azathioprine or an alternative immunosuppressive agent and 21 patients in the DO and 20 patients in the pulse group who are receiving steroids, respectively. Of the subgroup of patients who had a relapse, 13 pulse patients and 10 DO patients were receiving azathioprine or an alternative immunosuppressive agent and steroids at the time of first relapse. Five patients in the pulse group were receiving steroids only, and ten (33%) patients in the pulse group and five (33%) patients in the DO were not receiving any immunosuppression. Of the patients who had a renal relapse, 50% in both limbs were not receiving immunosuppression.
Duration of immunosuppression beyond the original study
Adverse events
Adverse events for the first 18 months were described in detail in the original publication.6 The long-term outcome questionnaire collected data on selected adverse events. There were no differences in adverse events between the two limbs (table 3).
Adverse events. There were no differences between trial treatment limbs in the incidence of adverse events beyond the original trial
Discussion
The last 20 years has seen the advent of clinical trials in ANCA-associated vasculitis that had aimed to reduce the cumulative dose of cyclophosphamide and associated toxicity. This study assessed the long-term outcome of patients recruited to the CYCLOPS Trial investigating the use of pulse cyclophosphamide compared with DO cyclophosphamide. Cyclophosphamide was given as per protocol and was continued for 3 months after remission in each limb. Pulse cyclophosphamide administered half the cumulative dose of cyclophosphamide and achieved similar remission rates and improvements in renal function at 18 months compared to that in the DO limb.6 After long-term follow-up, patient survival was similar between the two treatment limbs, despite an increased risk of relapse in patients treated with pulse cyclophosphamide. A previous meta-analysis of patients receiving cyclophosphamide using a pulse or DO regimen that included 143 patients also suggested a trend to increased relapse in patients treated with pulse cyclophosphamide.5
The pulse group received approximately 50% of the cumulative dose of cyclophosphamide that the DO group received in the original trial (DO 15.9 g (IQR, 11 g to 22.5 g) vs pulse 8.2 g (IQR, 5.95 g to 10.55 g)). It is assumed that the increased risk of relapse in the pulse group is due to less cyclophosphamide. It has previously been suggested that the risk for relapse is inversely associated with the cumulative cyclophosphamide dose received during the induction phase of treatment.8 9 In addition to the cumulative dose of cyclophosphamide, the administration schedule may affect outcome. There are suggestions that different T cell, dendritic cell and plasma cell subsets may have differing sensitivities to cyclophosphamide.10,–,12 In one murine model of asthma, administration of cyclophosphamide led to a paradoxical increase in airway inflammation with an associated reduction in regulatory T cells, interleukin 10 and TGFβ.13 It is interesting to speculate that pulse and DO cyclophosphamide regimens may have different effects on the depletion of regulatory and effector T cells or long- and short-lived plasma cells or on dendritic cell function in addition to the generally reduced immunosuppressive effect of less cyclophosphamide.
Our results are consistent with our original trial results6 and a previously published meta-analysis of pulse versus DO cyclophosphamide, which suggested an increased risk of relapse with pulse treatment.5 We also confirmed that PR3-ANCA at trial entry is a predictor of disease relapse.14 Although PR3-ANCA positive patients are at a higher risk of relapse than PR3-ANCA negative patients, they did not respond to pulse versus DO cyclophosphamide in an appreciably different manner in our subgroup analysis.
Although these results suggest that DO cyclophosphamide may be associated with a lower risk of subsequent relapse in patients with PR3-ANCA, this should be interpreted with caution. The original report of this trial demonstrated an increased risk of leucopaenia associated with the DO regimen, and in larger patient cohorts, leucopaenia has been demonstrated to be associated with increased mortality and infection.15 16 It should also be emphasised that the increased frequency of relapses was not associated with any increase in mortality or renal damage.
Patients at higher risk of immunosuppression-related adverse events—for example, older patients and those with more severe renal involvement—may benefit from the reduced incidence of leucopoenia seen with pulse cyclophosphamide even if there is an increased risk of subsequent relapse. Additionally, some of the benefits of lower cumulative cyclophosphamide exposure, such as a reduction in the rate of malignancy may not be realised for many years.17 There was no difference in malignancy between the two limbs; however, follow-up was relatively short to detect a difference.
The increased risk of relapse was not due to shorter duration of maintenance immunosuppression treatment. There were no differences between the two limbs in duration of steroid or antiproliferative treatment beyond the original trial. The median duration of antiproliferative use was 3 years, suggesting that irrespective of the induction regime used, relapse is perceived as a problem in all patients. We were unable to collect data on cumulative doses of immunosuppression. In another recent EUVAS trial, investigating maintenance treatment to reduce risk of relapse 72/156 (46%) of patients had a first relapse during the follow-up period (median, 39 months follow-up).18
It is interesting that in this study, PR3-ANCA positive patients had the highest risk of relapse with the pulse regimen. It is well known that MPO-ANCA patients relapse less often than PR3-ANCA patients,19 which may suggest that less cyclophosphamide is required for induction of remission in MPO-ANCA patients or that maintenance treatment can be stopped earlier. However, this must be interpreted with caution as there were only 15 episodes of relapse in the PR3-ANCA negative group (3 in the DO limb and 12 in the pulse limb) compared with 30 relapses in the PR3-ANCA positive group. Furthermore, we only adjusted for treatment and no other known risk factors for relapse.
There are limitations to this study. The original trial was not designed to assess the impact of the two regimens on a long-term relapse, and following the completion of the study, immunosuppression regimens were left to the treating physician. Despite this, there were no material differences on how patients were treated after the original study on the basis of their randomised treatment. This study still has limited power to address the question of relapse with only 45 relapses across both groups. However, the findings of the study are consistent with those of the previous meta-analysis.5 The current study was retrospective, with all the inherent potential biases associated with retrospective data collection. However, response rates to the questionnaire were good with 90% of data abstraction forms returned. Data abstraction forms were fully completed with only one returned questionnaire without complete information on relapse. Despite the retrospective nature of the study, it is unlikely that there was significant ascertainment bias.
Future studies should focus on biomarkers which predict relapse allowing tailoring of immunosuppression. Recent studies have suggested that a T cell signature predicting disease relapse may be identifiable at presentation. Validation of this signature in a clinical context would allow tailoring of immunosuppression in those at high and low risk of relapse.20
In conclusion, this study suggests that pulse cyclophosphamide is associated with an increased risk of relapse compared with DO cyclophosphamide but without a reduction in survival or increased renal impairment. The decision on which treatment regimen should be used must be based on the individual's risk of relapse along with their risk of adverse events secondary to cyclophosphamide.
Acknowledgments
In addition to the authors, the following investigators participated in the study: Department of Nephrology, Erasmus Hospital, Bruxelles, Belgium: D Abramowicz and M Wissing. Department of Nephrology, Edith Cavell Medical Institute, Bruxelles, Belgium: P Madhoun. Department of Nephrology, IMC de Tournai, Belgium: J Stolear.
Department of Medicine, Division of Nephrology, Helsinki University Central Hospital, Helsinki, Finland: A Ekstrand. Department of Nephrology, Charles University Hospital, Prague, Czech Republic: V Chabova and I Rychlik. Department of Nephrology, Hopital Docteur Duchenne, Boulogne sur Mer, France: P Bataille. Service de Rhumatologie, Centre Hospitalier du Mans, Le Mans, France: X Puechal. Cabinet de medecine interne et de néphrologie, Maubeuge,France: J Leblau. Department of Nephrology and Clinical Immunology, Hôtel Dieu, Nantes University Hospital, Nantes, France: VLM Esnault.
Rheumaklinik, Bad Bramstedt, Germany: WL Gross. Universitätsklinik Erlangen, Erlangen, Germany: S Weidner and H Rupprecht. Heinrich-Heine Universität, Düsseldorf, Germany: M Schneider and C Specker. Klinikum Mannheim, Mannheim, Germany: W Schmitt and F van der Woude. Dialysezentrum Paderborn, Germany: M Vischedyck. Department of Immunology, St. James Hospital, Dublin, Ireland: C Feighery. Nephrology Division, Department of Internal Medicine, University of Genoa, Genoa, Italy: G Garibotto. Ospedale San Carlo Borromeo, Milan, Italy: RA Sinico. Renal Unit, Ospedale S Maria delle Croci, Ravenna, Italy: M Santostefano. Department of Rheumatology, University of Vilnius, Vilnius, Lithuania: J Dadoniene. Department of Nephrology, Meander Medisch Centrum, Amersfoort, The Netherlands: EC Hagen. St. Antonius Ziekenhuis, Nieuwegein, The Netherlands: I Oudejans. Leiden University Medical Center, Leiden, The Netherlands: C Verburgh. Fundacio' Puigvert, Barcelona, Spain: J Ballarin. Hopital Clinic Y Provincal, Barcelona, Spain: E Mirapeix. Department of Nephrology, Hospital Doctor Josep Trueta, Girona, Spain: M Valles. Department of Nephrology, Huddinge University Hospital, Huddinge, Sweden: E Pettersson. Division of Rheumatology, Linköping University, Sweden: P Eriksson. Department of Nephrology, University of Lund, Lund, Sweden: D Selga and M Segelmark, Department of Nephrology, Malmo, Sweden: G Sterner. Department of Rheumatology, Karolinska Sjukhuset, Stockholm, Sweden: I Lundberg and E Svenungsson. Department of Immunology, University of Geneva, Geneva, Switzerland: C Chizzolini. School of Immunity and Infection, University of Birmingham, Birmingham, United Kingdom: D Adu. Department of Nephrology, Royal Devon Hospital, Exeter, United Kingdom: R de Souza.
References
Footnotes
-
Funding The CYCLOPS Trial was supported by the EU (Contract nos. BMH4-CT97-2328 and IC20-CT97-0019. This study was supported by a European League against Rheumatism grant and grants from Region Skåne, Sweden.
-
Competing interests None.
-
Ethics approval EUVAS – European Vasculitis Study Group.
-
Provenance and peer review Not commissioned; externally peer reviewed.