Article Text

Abstract
Objectives To compare the persistence of measles, mumps, rubella, diphtheria and tetanus antibodies between patients with juvenile idiopathic arthritis (JIA) and healthy controls.
Methods Measles, mumps, rubella (MMR) and diphtheria–tetanus toxoid (DT)-specific immunoglobulin G antibody concentrations were compared between 400 patients with JIA and 2176 healthy controls aged 1–19 years. Stored patient samples from the period 1997–2006 were obtained from one Dutch centre for paediatric rheumatology. Healthy control samples had been evaluated previously in a nationwide cohort. Participants had been vaccinated according to the Dutch immunisation programme. Antibody concentrations were measured by ELISA (MMR) or multiplex immunoassay (DT).
Results Corrected for age and the number of vaccinations, lower vaccine-specific geometric mean antibody concentrations (GMC) were found in patients with JIA against mumps, rubella, diphtheria and tetanus (p≤0.001). Measles-specific GMC were higher (p<0.001) compared with healthy controls. The prevalence of protective antibody concentrations was significantly lower in patients for mumps (OR 0.4; 95% CI 0.3 to 0.6), rubella (OR 0.4; 0.3 to 0.7), diphtheria (OR 0.1; 0.06 to 0.2) and tetanus (OR 0.1; 0.05 to 0.3). Seroprotection rates against measles did not differ between patients and healthy controls (OR 1.4; 0.8 to 2.5). Methotrexate and glucocorticosteroid use did not affect pathogen-specific GMC or seroprotection rates.
Conclusions Patients with JIA had lower antibody concentrations and seroprotection rates than healthy controls against mumps, rubella, diphtheria and tetanus, but not measles. In these patients, regular assessment of antibody concentrations and further research on responses to other (booster) vaccines are warranted.
Statistics from Altmetric.com
Vaccination has greatly reduced the burden of childhood infections.1 Outbreaks of vaccine-preventable infections occur predominantly in communities with low vaccination coverage, as demonstrated by poliomyelitis outbreaks.2 After vaccination, the maintenance of long-term antibody responses is essential for protective immunity against pathogens. Waning antibody concentrations may place vaccinated individuals at risk of infections.3 4 For example, measles outbreaks have occurred in vaccinated individuals with waning immunity demonstrated by low antibody avidity and lack of protective neutralising antibody concentrations.5
Effective vaccination is vital in juvenile patients with rheumatic diseases, who are at increased risk of infections due to the immunosuppressive effect of the disease or its treatment.6 7 Patients with juvenile idiopathic arthritis (JIA) are generally vaccinated according to national immunisation programmes. Although effective in healthy subjects, the duration of humoural immunity and of protection against vaccine-preventable diseases after vaccination are poorly defined in JIA.8
The aim of this study was to analyse the persistence of vaccine-specific antibody concentrations in patients with JIA in comparison with healthy age-matched controls. Two types of vaccines were evaluated; the live-attenuated measles, mumps and rubella (MMR) vaccine and the diphtheria–tetanus (DT) toxoid containing composite vaccine.
Methods
Study design
Antibody concentrations against measles, mumps, rubella, diphtheria and tetanus were assessed in a retrospective cohort of patients with JIA and compared with a historical cross-sectional cohort of age-matched controls. The JIA cohort included patients born between 1979 and 2003. The control cohort was collected from a Dutch nationwide cross-sectional study performed in 1995–6.9
Setting and participants
Patients were recruited from a tertiary centre for paediatric rheumatology (Wilhelmina Children's Hospital, University Medical Centre Utrecht, The Netherlands). Four hundred and sixteen patients with an available blood sample at an age between 1 and 19 years obtained in the period 1997–2006, and with a confirmed JIA diagnosis according to the International League of Associations for Rheumatology criteria,10 were eligible for inclusion; 2460 controls from the historical cohort aged between 1 and 19 years were eligible. Children in the control cohort had no known contraindication for vaccination and will be further referred to as healthy controls. Controls born before the introduction of measles vaccination in 1976 or individuals who reported more than the conventional amount of vaccinations were excluded. This study was approved by the medical ethics committee and informed consent was obtained.
The MMR vaccination schedule has undergone several changes over the years. Therefore, participants were subdivided into an early birth cohort (1976–85) and a late birth cohort (1986–2003). Analyses focused on the latter cohort, because this cohort resembles the current situation: all children born since 1986 received the MMR vaccine (Dutch National Institute of Public Health and the Environment (RIVM)/the Dutch Vaccine Institute (NVI), Bilthoven, The Netherlands) at the age of 14 months and 9 years. In the earlier cohorts, children received the measles monovaccine at 14 months and either a MMR vaccination at the age of 4 years (children born between 1983 and 1985) or a rubella vaccination (RIVM, Bilthoven, The Netherlands) in girls at the age of 11 years (children born between 1976 and 1983). Vaccinations against diphtheria and tetanus (RIVM/NVI, Bilthoven, The Netherlands) are administered four times during the first year of life, and subsequently at the ages of 4 and 9 years.
Outcomes
Antigen-specific antibodies
The primary outcomes were MMR and DT-specific immunoglobulin G (IgG) antibody concentrations and the percentage of patients with antibody concentrations above levels that are considered protective (ie, seroprotection rate).
Virus-specific IgG serum antibodies against measles (strain Edmonston), mumps (strain Jeryl Lynn) and rubella (strain HPV77) were quantified using an ELISA.11,–,14 The lower limit of quantitation (LLOQ) was 0.02 IU/ml for measles, and 3.0 IU/ml for rubella. As no international reference serum for mumps exists, an inhouse reference of the RIVM laboratory was used to measure antibody concentrations in local RIVM units (RU). The LLOQ for mumps was 4.0 RU/ml.13 15 Serum antibodies against diphtheria and tetanus were measured with the toxin binding inhibition assay in healthy controls and by multiplex immunoassay in patients.16,–,18 These methods are excellently correlated (Pearson's correlation coefficient r≥0.95).16 The LLOQ used for both diphtheria and tetanus was 0.01 IU/ml. Concentrations below the LLOQ were set to 50% of this limit.17
The cut-off value for seroprotection was 0.2 IU/ml for measles and 10 IU/ml for rubella conform to international standards.19 The minimum protective level for mumps was determined using a panel of sera from 1-year-old children resulting in a value of 45 RU/ml.15 The minimum protective level for DT antitoxin antibodies was 0.01 IU/ml according to the WHO.20
Covariates
The vaccination data from healthy controls were obtained from the previous nationwide study.21 The vaccination data of patients were retrieved from parents and the national vaccination registration database. When vaccination data could not be retrieved, participants were considered to be vaccinated, given the high vaccination coverage (>95%) in The Netherlands.22 To correct for potential confounders, the following clinical data at the moment of blood sampling were collected from medical charts: JIA type, disease duration, disease activity and medication use. JIA disease activity was measured using standard validated core set criteria.23 JIA disease was considered active when the physician's global assessment measured on a 0–10 cm visual analogue scale was above 1 cm in combination with either an erythrocyte sedimentation rate greater than 20 mm/h or one or more active joint. The use of glucocorticosteroids, methotrexate and anti-tumour necrosis factor alpha (TNFα) therapy was documented.
Statistical analysis
Antibody levels were expressed as geometric mean antibody concentrations (GMC). Antibody concentrations were compared between patients and healthy controls using the Student's t test. Subsequently, multivariable linear regression analysis was performed to correct for age and the number of vaccinations. Logistic regression analysis, via the same two-step approach, was performed to test for differences in seroprotection rates between patients and controls. The regression analyses were performed separately in the two birth cohorts.
Preplanned subgroup analyses were performed in patients only to assess antibody levels and seroprotection rates by JIA subtypes, medication use, gender and disease activity by multivariable linear and logistic regression analyses including all four covariates. For these analyses JIA was divided into: oligoarticular JIA, polyarticular JIA, systemic JIA and other subtypes including psoriatic and enthesitis-related JIA (table 1). No differences were detected in the distribution of JIA subtypes, medication use, gender and disease activity between the birth cohorts (data not shown). Therefore, these analyses were performed in the total JIA cohort.
Baseline characteristics of patients and controls
Statistical analyses were performed using SPSS version 17.0. Statistical significance was designated as a two-tailed p value less than 0.05.
Results
Sixteen patients and 168 healthy controls were excluded for an aberrant number of measles or mumps vaccinations, 116 healthy controls born before 1976 were also excluded. In total, 400 patients with JIA and 2176 healthy controls were included (table 1). Seven hundred and fifty-five (35%) healthy controls and 37 (9%) patients were from the early birth cohort (1976–85). Although age-matched, healthy controls were significantly younger, making correction for age obligatory in all analyses. The cohort 1976–85 consisted predominantly (>80%) of subjects aged 12 years and older, the cohort 1985–2003 consisted of 80% of subjects less than 12 years. The time interval between vaccination and blood sampling did not differ significantly between patients and controls. Patients were vaccinated significantly more frequent than healthy controls. Vaccination history could not be retrieved on the MMR vaccination in 27 (7%) patients and 280 (13%) healthy controls. Data on DT vaccination were lacking for 45 (11%) patients and 313 (14%) healthy controls. Regarding medication use, 93 (23%) patients used methotrexate (median dose 10 mg/m2 per week) and 28 (7%) used glucocorticosteroids (median dose 10 mg/day). Five patients used high-dose steroids (≥20 mg/week). Eight (2%) patients received anti-TNFα therapy.
JIA versus healthy controls
Antibody levels
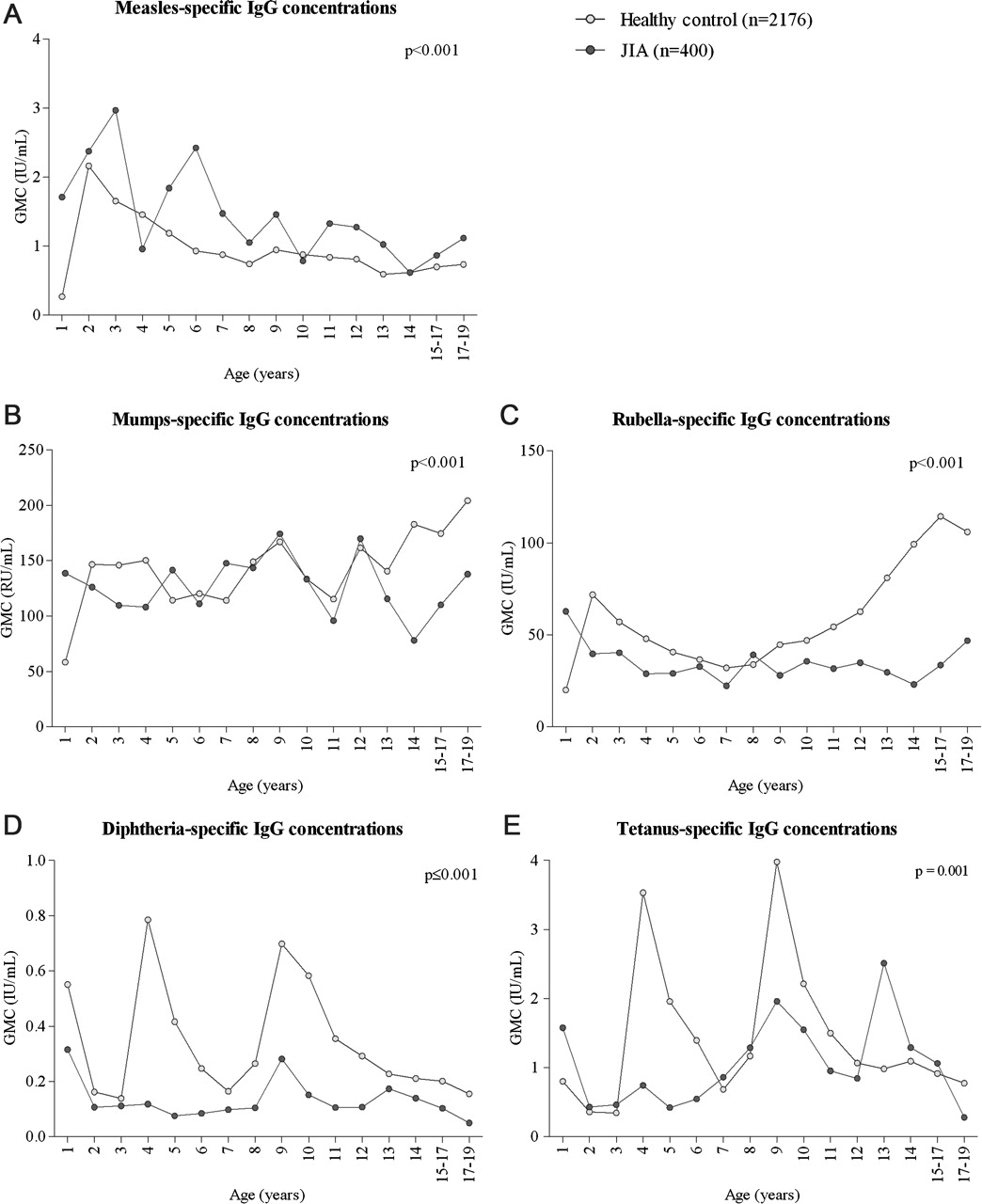
Corrected for age and the number of vaccinations, vaccine-specific GMC against measles were higher in patients with JIA (p<0.001), whereas GMC against mumps (p<0.001) and rubella (p<0.001) were lower (figure 1A–C). The MMR results were similar for the most recent birth cohort and the early cohort. GMC against diphtheria and tetanus were lower in patients in both birth cohorts (p≤0.001, figure 1D–E). As differences were most pronounced in older subjects, we analysed whether differences could also be detected in subjects under 12 years in the 1985–2003 cohort. In younger subjects, similar higher GMC for measles and lower GMC for rubella, diphtheria and tetanus were found (p<0.001) in patients, whereas no differences were detected between patients and controls for mumps-specific antibodies (p=0.197).

(A–E) Measles, mumps, rubella, diphtheria and tetanus serology in juvenile idiopathic arthritis (JIA) patients and healthy controls. Vaccine-specific antibody concentrations are depicted in 1-year age groups. Each group reflects 15–35 patients and 56–250 healthy controls. The results of patients above the age of 15 years are combined into 2-year age groups due to small patient numbers. GMC, geometric mean concentrations.
The effect of the MMR booster at 9 years on virus-specific antibody concentrations was small in both patients and healthy controls (figure 1A–C). Regarding the DT booster, a marked rise in DT-specific antibody levels was observed in healthy controls both after 4 and 9 years of age. In contrast, no increase in DT antibodies was detected after the age of 4 years in patients with JIA despite DT booster vaccination in 93% (figure 1D–E). As diphtheria and tetanus vaccines are administered in conjunction with polio vaccination (DTP vaccine), the responses against polio serotypes 1, 2 and 3 were tested. Similarly, the polio-specific antibody responses were markedly lower in patients compared with healthy controls for each serotype (data not shown). In patients aged 9–11 years a modest DT-induced increase in antibody concentrations was detected; markedly lower than in healthy controls.
Seroprotection rate
Adjusted for age and the number of vaccinations, the seroprotection rates against mumps, rubella, diphtheria and tetanus were significantly lower in patients with JIA compared with healthy controls (table 2). The odds rate for protection against these pathogens varied from 0.03 to 0.4 in patients compared with healthy controls. In contrast, seroprotection rates against measles did not differ between patients and controls (OR 1.4; 95% CI 0.8 to 2.5).
OR for seroprotection in JIA patients in comparison with healthy controls
JIA subgroup analyses
Associations between JIA subtypes, medication use, gender and disease activity
As expected, more JIA patients with polyarticular and systemic JIA used immunosuppressive medications; 37% of polyarticular and 35% of systemic JIA patients used methotrexate versus 8% of other JIA types (p<0.001). Thirty per cent of patients with systemic JIA used glucocorticosteroids compared with 1–7% of other subtypes (p<0.001). Relatively more patients with polyarticular (63%) and systemic JIA (65%) had active disease at the time of sampling compared with other subtypes (37%; p<0.001). Eight patients used anti-TNFα treatment; five had systemic JIA and three polyarticular JIA.
Antibody levels in relation to JIA subtypes, medication use, gender and disease activity
Patients with systemic JIA showed significantly lower antibody concentrations against measles (p=0.025), mumps (p=0.018) and tetanus (p=0.027). A similar trend was observed for rubella (p=0.077), in contrast to diphtheria (p=0.316; figure 2A–F). Regarding medication use, methotrexate use and glucocorticosteroid use did not have any effect on pathogen-specific GMC (figure 3A–E). There was a weak negative correlation between the methotrexate dose and antibody concentrations against mumps (r=−0.15), rubella (r=−0.29), diphtheria (r=−0.28), tetanus (r=−0.23) but not for measles (r=0.04). This was significant for rubella (p=0.009) and diphtheria (p=0.007). There was no association between the glucocorticosteroid dose and antibody concentrations. The number of patients using anti-TNFα treatment was too small to assess the effect on GMC. Gender did not influence antibody concentrations. Higher antibody concentrations were observed in patients with high disease activity; this reached statistical significance only for measles-specific antibodies (p=0.024; data not shown).

Vaccine-specific seroprotection rates and antibody concentrations in juvenile idiopathic arthritis (JIA) subtypes. (A) For each vaccine the percentage of patients with antibody concentrations above the protective level are indicated in the four JIA subtypes. In comparison with oligoarticular JIA patients, systemic JIA patients had lower seroprotection rates against measles (p=0.021), mumps (p=0.036) and rubella (p=0.028). Other JIA types had lower mumps-specific seroprotection rates (p=0.024). (B–F) The vaccine-specific antibody concentrations per JIA subtype are indicated. Patients with systemic JIA had lower antibody concentrations against measles (p=0.025), mumps (p=0.018), rubella (p=0.077) and tetanus (p=0.027), in contrast to diphtheria (p=0.316). *p<0.05. GMC, geometric mean concentrations; OJIA, oligoarticular juvenile idiopathic arthritis; PJIA, polyarticular juvenile idiopathic arthritis; SoJIA, systemic onset juvenile idiopathic arthritis.

{kind=link}
{kind=link}
{kind=link}
Vaccine-specific antibody concentrations versus medication use. (A–E) Each graph depicts vaccine-specific antibody concentrations in patients with or without methotrexate (MTX), glucocorticosteroids or anti-tumour necrosis factor alpha (TNFα) treatment. GMC, geometric mean concentrations.
Seroprotection rates in relation to JIA subtypes, medication use, gender and disease activity
Patients with systemic JIA had a lower prevalence of protective antibody levels against measles (p=0.021), mumps (p=0.036) and rubella (p=0.028) (figure 2A). For diphtheria and tetanus, seroprotection rates did not differ between JIA subtypes. Medication use, gender and disease activity did not influence seroprotection rates. There was no relation between the methotrexate dose and seroprotection rates. Too few seronegative patients used high-dose steroids to analyse correlations between the dose and seroprotection.
Discussion
Patients with JIA had lower mumps, rubella, diphtheria and tetanus-specific antibody concentrations in comparison to age-matched healthy controls. The responses towards booster vaccinations were markedly lower in patients. Moreover, the prevalence of protective MMR and DT-specific antibody levels was significantly lower in patients with JIA, except for measles. Patients with systemic JIA had the lowest antibody concentrations and seroprotection rates. The use of glucocorticosteroids or methotrexate did not influence the antigen-specific antibody concentration or seroprotection rates.
Numerous studies analysed vaccine responses in patients with rheumatic diseases. Responses were generally comparable with healthy controls, although some studies found lower antibody concentrations.8 The follow-up in these studies was a maximum of 2 years. Our cross-sectional approach enabled us to analyse the long-term persistence of antibodies in a large JIA cohort, revealing previously undetected clear differences between patients and healthy controls. Another interesting difference between our results and the literature is that we found higher antibody concentrations in patients with active disease. Most studies found no effect of disease activity24,–,29 or lower antibody concentrations in patients with active disease during vaccination.30 31 We cannot explain the higher antibody concentrations in patients with active disease. Possibly, non-specific immune activation during active disease, as seen in patients with systemic lupus erythematosus (SLE), plays a role. In these patients, increased total IgG and anti-tetanus IgG levels were detected before SLE exacerbations.32
Previous studies analysed the effect of immunosuppressive drugs at the time of vaccination on antibody responses, whereas we could analyse the effect on the persistence of antibody concentrations. In previous studies methotrexate did not influence the response to MMR vaccination in 10 patients with JIA.33 Glucocorticosteroids lowered the GMC but not the response rate to tetanus vaccinations in 40 juvenile patients with rheumatic diseases.29 We found that methotrexate and glucocorticosteroid use did not influence humoural immunity. The weak negative correlation between the methotrexate dose and antibody concentrations implies that high-dose methotrexate could negatively affect antibody concentrations although the methotrexate dose was not related to seroprotection.
A limitation of our study was that we had no data on infection rates but measured antibodies as surrogate markers for protection against infections.34 Antibody levels are considered good correlates of protection against diphtheria, tetanus (>0.01 IU/ml) and rubella (10 IU/ml).34 In contrast, for measles, cellular immunity can protect against infections despite waning measles-specific antibodies.35 Cellular immunity has been shown for tetanus,36 mumps37 and rubella,38 although their protective effect is unknown. For mumps, no certain correlate of protection is internationally accepted.37 Therefore, we measured lower antibody concentrations in patients with JIA, yet we do not know whether this led to increased (susceptibility of) MMR or DT infections.
Another limitation was missing vaccination data. A complete vaccination history could not be retrieved for 7–11% of patients and 13–14% of healthy controls. However, excluding these participants did not influence the results, except for the fact that lower mumps-specific antibody concentrations in the birth cohort after 1985 failed to reach significance. As the number of vaccinations was lower in healthy controls, one might suggest that the natural infection rate was higher in controls. It is known that natural infection induces greater antibody concentrations of longer duration.39 The high antibody concentrations against measles, mumps and rubella in older subjects, who predominantly originate from the early birth cohort, could be explained by the higher more frequent occurrence of natural infections.39 To prevent confounding by differences in herd immunity or natural infection rates, participants were subdivided into an early birth cohort (1976–85) and a late birth cohort (1986–2003). In the late birth cohort, natural infection rates in the population were negligible due to high vaccination coverage.22 For mumps antibodies, indeed the differences between patients and controls disappeared in subjects from the late birth cohort aged under 12 years. However, the seroprotection rate for mumps remained lower in patients. Also for rubella, diphtheria and tetanus antibody concentrations and protection rates remained significantly lower in patients under 12 years. Therefore, differences in natural infection rates and vaccination coverage cannot be the sole explanation for lower humoural immunity in patients with JIA.
An interesting question then remains as to why patients with JIA have lower vaccine-specific antibody concentrations? Vaccine-dependent effects or intrinsic immunological defects in rheumatic diseases could be potential explanations. Regarding the former, it is known that the persistence of antibody concentrations may be affected by the vaccine type, such as live-attenuated organisms (eg, MMR), or toxoid vaccines (eg, DT).21 36 We tested two different vaccine types with similar lower antibody concentrations and seroprotection rates in patients with JIA. Therefore, it is less plausible that the vaccine itself is fully responsible for the differences between patients and healthy controls. Yet there is a partial vaccine-dependent effect, because measles antibodies were higher in patients. We cannot explain this exception for measles. Similar results were described in a retrospective study including 18 vaccinated patients with SLE and 11 healthy controls. Patients showed lower antibody concentrations and seroprotection rates than healthy controls for tetanus, but not for measles.40 A potential explanation lies in the immunogenetic basis of the immune response to measles.41 The heritability of the immune response to measles is higher (89%) than for mumps (39%) and rubella (46%).42 The genetic determinants of measles vaccine-induced immune response were found in polymorphisms in the HLA gene that have also been associated with JIA.43 44
Regarding intrinsic immunological defects in rheumatic diseases, a minority of patients with rheumatic diseases have primary immunodeficiencies;45 B cells may be involved in the pathogenesis of JIA,46 and disturbed T-cell homeostasis characteristic of premature ageing of the immune system has been described in JIA.47 This immunosenescence may result in low vaccination responses, as seen in the elderly.48
As a result of high herd immunity, infections with mumps, rubella, diphtheria and tetanus do not occur frequently despite lower antibody levels and seroprotection rates in patients with JIA. However, the risk of infections increases when patients travel into areas with low herd immunity. Moreover, in countries in which immunity is almost solely acquired through vaccination, the persistence of immunological memory after vaccination is crucial to maintain herd immunity. The lower vaccine-specific antibody levels enforce a more pro-active approach in vaccinating juvenile patients with rheumatic diseases. We strongly suggest measuring antibodies against vaccine-preventable diseases regularly in these patients to detect waning immunity. Although responses to booster vaccinations were low, a booster could maintain seroprotective antibody concentrations. In addition, 9-year-old patients responded moderately to the DT booster vaccine, whereas no response was detected in 4-year-old patients. Possibly, patients with JIA could benefit from additional booster vaccinations at older ages.49 This may ultimately prevent infections in vulnerable patients. Further research is warranted on explanatory mechanisms and on responses to other (booster) vaccines.
Acknowledgments
The authors would like to thank Ton Marzec (National Institute of Public Health and the Environment) for performing the measles neutralisation assays and Cuno Uiterwaal for his input on the statistical analysis.
References
Footnotes
-
Funding MWH received fees from the Dutch Arthritis Association (project number 07-02-403). Funders were not involved in the study design; in the collection, analysis and interpretation of data; in writing of the report; or in the decision to submit the article for publication.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The protocol for JIA patients was approved by the medical ethics committee of the University Medical Centre Utrecht (protocol number 07-068). The nationwide study in healthy controls was approved by the medical ethics committee of The Netherlands Organisation for Applied Scientific Research (TNO), Leiden, The Netherlands.
-
Provenance and peer review Not commissioned; externally peer reviewed.