Article Text

Abstract
Objective To obtain longitudinal data on growth/puberty in a large-scale, multi-national prospective cohort of juvenile systemic lupus erythematosus (SLE).
Methods Data from 331/557 (59.4%) patients ≤18 years old with juvenile SLE in active phase, with anthropometric data available at four follow-up visits, were studied.
Results There was a significant reduction in parent-adjusted height z score with time in females and males (p<0.0001), with a significant gender difference (p<0.0001) and with male height being most affected. Median body mass index z score peaked at 6 months and was still significantly above baseline after 26 months (p<0.01), with no gender difference. Standardised height reduction was inversely related to age at onset. Females with onset age <12 years had a median parent-adjusted height z score of −0.87 with no catch-up growth. At the end of the study, growth failure was seen in 14.7% of the females and 24.5% of the males. Height deflection (less than −0.25/year) was found in 20.7% of the females and 45.5% of the males. Delayed pubertal onset was seen in 15.3% and 24% of the females and males, respectively, and delayed/absent menarche was seen in 21.9%, while 36.1% of the females and 44% of the males had some degree of delayed pubertal development. Growth failure baseline determinants were previous growth failure (OR: 56.6), age at first visit ≤13.4 years (OR: 4.2) and cumulative steroid dose >426 mg/kg (OR: 3.6).
Conclusions The children at risk of having a negative effect on height and pubertal development are prepubertal and peripubertal children treated with >400 mg/kg cumulative dose of corticosteroids.
Statistics from Altmetric.com
Children represent 15%–20% of patients with systemic lupus erythematosus (SLE).1 Compared to adult-onset SLE, juvenile SLE is considered more severe, resulting in more intensive treatment2,–,4 and higher mortality.5 Growth failure and delayed puberty are unique features of juvenile SLE,6 7 caused by long-term disease activity, side effects of drugs and/or comorbid conditions. Delayed growth and puberty may result in irreversible damage, affect the patients' quality of life and add to the burden of coping with a chronic disease.7 During the last decades, decreasing mortality in juvenile SLE1 has redirected focus towards avoiding permanent damage.9 Concomitantly, the goal for the patients is no longer only to survive, but to grow and mature sexually into adulthood, with minimal loss of their physical, emotional and genetic potential. Due to the rarity of the disease and lack of large-scale cohort studies, knowledge of growth and pubertal development in juvenile SLE has been limited.7 10,–,12
The goal of this project, conducted by the Paediatric Rheumatology International Trials Organisation (PRINTO),13 was to obtain longitudinal data on growth and puberty in a large-scale cohort of juvenile SLE followed for 26 months. A secondary goal was to evaluate the possible determinants influencing anthropometric outcome data.
Methods
We extracted the data from a prospective, multi-centre study on 557 patients with juvenile SLE enrolled in 2001–2004.8 14 15 Inclusion criteria were a convenience sample of juvenile SLE,16 17 age younger than 18 years at enrollment and an active phase of disease, defined as either the need to start corticosteroids and/or new immunosuppressants or the need to receive a major dose increase in corticosteroid and/or immunosuppressant.14 15 The study population of the present study consisted of all 331 (59.4%) patients with anthropometric data available at baseline and at the three follow-up assessments (6, 12 and 24 months) (figure 1). Written or verbal informed consent was obtained from a parent or legal guardian according to the requirements of the local ethics committees.

Flow diagram of the juvenile systemic lupus erythematosus (SLE) study patients; F, females; M, males. Denominators refer to the number of patients with anthropometric data available at each time point.
Anthropometric data
Height (cm) and weight (kg) were measured at each visit with type of stadiometer specified (Harpenden, wall-mounted, sitting height or other). Height was preferentially measured in the morning by the same operator and with the same stadiometer throughout the study. Parents' height was required at baseline, with self-reported height being acceptable. Body mass index (BMI) was calculated as weight (kg) divided by height (meters) squared. Standardisation of height and BMI was performed with the least-mean squares method18,–,20 with age-adjustment according to chronological age (months), expressed as z score, using the WHO growth reference 2007.21 22 Parent-adjusted height z score was calculated as the difference between height z score for chronological age and target height (average of parents' height +6.5 cm for boys and −6.5 cm for girls).23 24 Growth failure was defined as parent-adjusted height z score <−1.525. Height deflection was defined as decreased height z score >0.25 per year26 compared to baseline (Δ height z score <−0.25/year).
Puberty and sexual maturation data
Female and male sexual maturity rating was assessed by clinical examination according to the Tanner methods27 28 and specified according to breast (B1–B5) and pubic hair (PH1–PH5) maturation in girls, and testis (T1–T5), penis (P1–P5) and pubic hair (PH1–PH5) in boys. Dates of female B2, PH2 and menarche and of male T2, P2 and PH2 were specified, together with menses type (regular, irregular or stopped) and testis volume (ml). Pubertal onset was defined as B2 in females or, in males, T2 and/or testis volume ≥4 ml. Pubertal onset age was calculated from the date of female B2/male T2. Delayed pubertal onset was defined as age at B2 ≥13 years or age at T2 ≥14 years.29 With the 95th percentile of menarche being at 14.5 years,29 delayed menarche was defined as age of menarche ≥15 years. Based on a normal tempo between B2–B5 and G2–G5 lasting 3–4 years,29 30 delayed pubertal tempo was defined as follows: (1) B2 for more than 1 year in a late-maturing girl (age at first visit ≥11 years), (2) B2 ≥2 years in a normal-maturing girl (age at first visit ≥9 years and <11 years), (3) B3 ≥1 year and age at first visit ≥12 years, (4) B3 ≥2 years and age at first visit ≥11 years and <12 years, (5) T2≥1 year and age at first visit ≥12 years, (6) T2 ≥2 years and age at first visit ≥10 years and <12 years, (7) T3 ≥1 year and age at first visit ≥13 years or (8) T3 ≥2 years and age at first visit ≥11 years and <13 years.6 Delayed puberty was defined as a delay in pubertal onset, pubertal tempo or menarche.
Statistics
Descriptive data were reported as medians and 1st, 3rd quartiles (1st, 3rd q) or frequencies. Longitudinal data were analysed with the repeated-measurements analysis of variance (Friedman test) with post hoc comparison tests adjusted with Bonferroni's correction. Patients were subgrouped according to age at disease onset: females <8 (prepubertal), 8–13 (peripubertal) and ≥13 (postpubertal) and males <14 (pre/peripubertal) and ≥14 (postpubertal) years and, for bivariate analyses of outcome in females, age <12 and ≥12 years (receiver operating characteristic (ROC) curve). Corticosteroids (oral or pulses), cyclophosphamide, azathioprine, ciclosporin A, methotrexate and other concomitant treatments were recorded. Cumulative corticosteroid dose, from baseline visit to the last available assessment, was calculated by the area under the curve with approximation of the trapezoidal rule. We evaluated the possible association between baseline disease characteristics (as detailed in table 1) and cumulative corticosteroid dose with growth failure and pubertal delay. In the bivariate analysis, comparisons of quantitative variables between two patient groups were made by the Student's t test or the Mann–Whitney U test, and comparisons of frequencies were made by the χ2 test or Fisher exact test, as appropriate. A logistic regression analysis was performed to evaluate the role of significant (p<0.05) baseline variables (table 1) plus cumulative steroid dose with growth failure or pubertal delay at the last assessment. OR, 95% CI, likelihood ratios and area under the ROC curve were reported. Data were entered in Access XP database and analysed by two of the authors (MR and AP) with Excel XP (Microsoft, Redmond, Washington, USA), Statistica 9 (StatSoft Corp., Tulsa, Oklahoma, USA) and Stata 7 (Stata Corporation, Texas, USA).
Baseline characteristics of 557 patients with juvenile systemic lupus erythematosus and comparison between included* and excluded patients of the growth study
Results
A total of 331 of 557 (59.4%) patients had complete height data at all four assessments, and 274 of these also had both parents' heights available (figure 1). No differences in baseline characteristics were found between included patients and patients with incomplete height data (table 1). Minor differences were found in the physician's global assessment of disease activity and damage and 24-h urine protein. For anthropometric data, included patients showed a higher frequency of baseline growth failure compared to those excluded. The only gender difference found among the 331 included patients was 24-h urine protein, being higher in males at baseline (data not shown).
Height and BMI
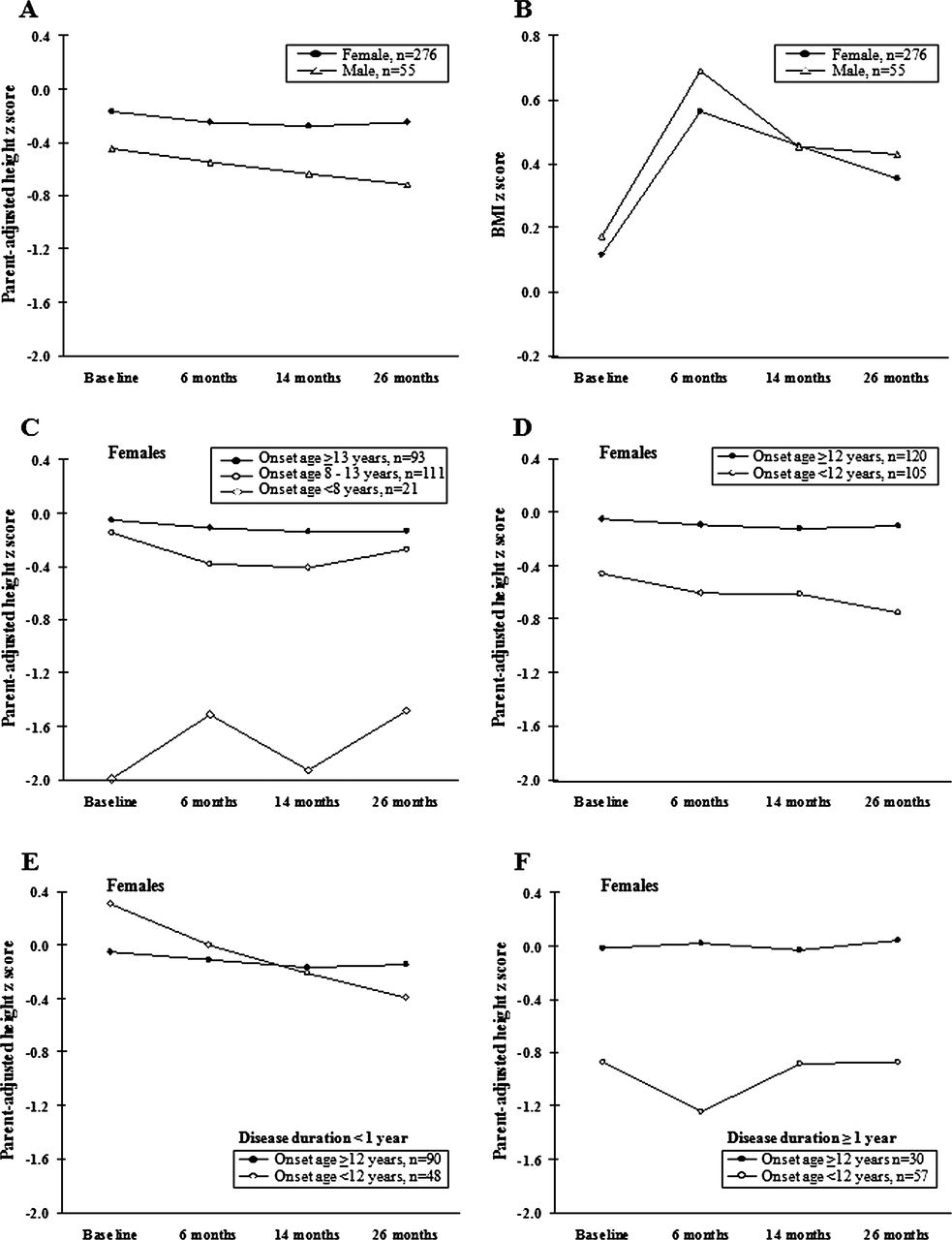
Throughout the study, height was measured with wall-mounted (70.8%) or Harpenden (22.4%) stadiometers. Anthropometric characteristics of 331 patients with complete height data are summarised in table 2. At baseline, female median parent-adjusted height z score was −0.17, while the corresponding male score was −0.45. During the following 26 months, a statistical significant reduction was seen in actual and in parent-adjusted height z scores, being more pronounced for males (see also figure 2A).

{kind=link}
{kind=link}
Longitudinal aspects of median parent-adjusted height z score and body mass index (BMI) z score in juvenile systemic lupus erythematosus according to gender (A–B), age at disease onset (C–F) and disease duration (E–F).
Longitudinal anthropometric characteristics in juvenile systemic lupus erythematosus, n=331
Median BMI increased significantly in both sexes, peaking at 6 months, with no gender differences. At the end of the study, BMI z scores were still significantly above baseline scores (table 2 and figure 2B).
Growth failure was observed in 16.9% of females and 22.4% of males at baseline, with no further increase during the study and no gender difference. Height deflection, expressed as Δ height z score <−0.25/year from baseline, was most pronounced during the first 6 months, but still present after 26 months in 20.7% of the females and 45.5% of the males.
Impact of age at disease onset on height
By subgrouping the females according to age at disease onset, three significantly different height patterns were seen (figure 2C). Prepubertal females (onset age <8 years) had significantly lower parent-adjusted height z scores, with baseline median score of −1.99 (−2.81, 0.22) remaining constant throughout the follow-up. Postpubertal females (onset age ≥13 years) had baseline scores near the age-matched reference and no further decrease. In contrast, peripubertal females (onset age 8–13 years) with baseline score of −0.15 (−1.02, 0.70) demonstrated a significant decrease with time, reaching the lowest levels at 14 months with parent-adjusted height z score of −0.41 (−1.25, 0.48).
To evaluate the effect of disease duration on height, we repeated the analysis by dichotomising patients according to age at onset <12 versus ≥12 years. Females with onset age <12 years had parent-adjusted height z score of −0.46 (−1.63, 0.64) at baseline and −0.75 (−1.56, 0.24) at 26 months, while older females kept closer to their age-matched reference (from −0.05 to −0.11 at 26 months) (figure 2D).
In females with short disease duration at baseline (median 0.2 years, n=138), there was no difference between onset age categories (figure 2E). However, females with onset age <12 years decreased in parent-adjusted height z score from 0.31 at baseline to −0.40 at 26 months, while females with disease onset ≥12 years kept closer to the reference (from −0.05 to −0.15). In contrast, females with longer disease duration at baseline (median 3.1 years, n=87) differed significantly according to onset age (figure 2F). With onset age <12 years, parent-adjusted height z score was low at baseline (−0.87) and remained low during follow-up. Females with disease onset ≥12 years remained at the normal age-matched reference throughout the study (from −0.02 to 0.04). The effect of onset age and disease duration on males was not statistically significant.
Puberty at last assessment
Table 3 shows the pubertal characteristics of the 276 females during the follow-up period. Of these 276 patients, some were not evaluable for pubertal characteristics as detailed on the online supplementary Table S1. A delayed pubertal onset was found in 15.3% (11/72 evaluable adolescents) with a median pubertal onset age (B2) of 11.9 years. The 203 excluded patients were as follows: in 114 patients, pubertal onset was already started at first visit, 15 patients were <13 years of age at last follow-up, and 74 were not informative with respect to pubertal onset.
Pubertal characteristics of the 147/276 (53.3%) evaluable females with juvenile SLE
The proportion of adolescents with delayed or absent menarche was 25/114 (21.9%), with a median age at menarche of 13.6 years in the subgroup of 104 girls with menarche appearing after disease onset. The 162 non-evaluable girls were 114 patients who had menarche before the disease onset and 48 who were too young at last visit to be informative (15 being <13 years and 33 being <15 years at the end of the study). Irregular menses or postmenarche amenorrhoea was registered in 48/104 (46.2%). For boys, a delayed pubertal onset was found in 6/25 (24%) and delayed puberty in 11 (44%). Median pubertal onset age (T2) was 13.4 (13.1, 14.4) years; PH2 and P2 was 13.1 (12.6, 14.2) and 13.4 (12.9, 13.9) years, respectively. Of the 55 boys, 30 were not evaluable for pubertal characteristics for the following reasons: 21 patients were ≥14 years and T3/4/5 at baseline, and 9 were <14 years at last available assessment (data not shown).
Anthropometric outcomes and predictors of growth failure and pubertal delay
At the end of the study, there was significantly more growth failure and height deflection in girls with onset age <12 compared to ≥12 years (table 4). For boys with onset age <14 years, the pattern was the same, although levels of significance were not reached. Growth failure in girls was strongly associated with delayed puberty and menarche (p=0.0005 and p=0.006, Fisher exact), but not with height deflection (p=0.37, χ2). Likewise, growth failure in boys was significantly associated with delayed puberty (p=0.01, Fisher exact), but not with height deflection (p=0.92).
Growth and pubertal outcome in juvenile systemic lupus erythematosus after 26 months according to age at disease onset
We evaluated the potential baseline determinants for the two most important outcomes: growth failure and pubertal delay. In the bivariate analysis of female patients, an association was found between growth failure at last available assessment and growth failure at baseline (OR: 74; 95% CI: 25.3 to 216.7), onset age (<12 versus ≥12 years; OR: 8.4; 95% CI: 3.1 to 22.6), age at first visit (≤13.4 versus >13.4 years; OR: 4.9; 95% CI: 2.1 to 11.1), disease duration (>16 versus ≤16 months; OR: 2.2; 95% CI: 1.1 to 4.7) and cumulative steroid dose (≥426 mg/kg) (OR: 5.0; 95% CI: 2.2 to 11.1). A statistical significant association was also found between cumulative steroid dose (>537 mg/kg; OR: 3.76; 95% CI: 1.30 to 10.89) and pubertal delay. For males, an association emerged between growth failure at last assessment and growth failure at baseline (OR: 52.5; 95% CI: 7.6 to 362.9) and cumulative steroid dose (≥310 mg/kg; OR: 8.2; 95% CI: 1.6 to 43.1). No baseline characteristic was associated with pubertal delay in males.
In the logistic regression model, baseline determinants for growth failure were growth failure at baseline (OR: 56.6; 95% CI: 20.8 to 154; p<0.0001), age at first visit (≤13.4 versus >13.4 years; OR: 4.2; 95% CI: 1.5 to 11.6; p=0.004) and cumulative steroid dose (≥426 mg/kg; OR: 3.6; 95% CI: 1.3 to 9.7; p=0.011); all these ORs were also adjusted for gender (OR: 2.6; 95% CI: 0.8 to 8.1; p=0.099). The area under the ROC curve was excellent: 0.95. The model was substantially unchanged when we excluded the 49 patients who presented with growth failure at baseline.
Discussion
Several authors have pointed to the importance of including growth and puberty when evaluating consequences of juvenile SLE,6 7 31 32 but studies are few.7 10 We present the results of the largest prospective, longitudinal study on growth and puberty in juvenile SLE. Although parent-adjusted height z score was significantly reduced with time in the whole cohort, girls with age at onset ≥12 years had a minor reduction in expected height, with values close to the reference, in patients with short and long disease duration. As median onset age was 12.4 years, a majority of female patients with juvenile SLE had a minor risk of growth disturbance.
In contrast, females with early-onset disease had a marked reduction in height score, most pronounced within the first years of disease and with little catch-up growth, resulting in significantly higher proportions of growth failure and height deflection in the prepubertal/peripubertal-onset group. In general, boys had similar parent-adjusted height scores as young girls. This marked difference in growth patterns according to onset age and gender has not previously been noted.
Although it has been claimed that juvenile SLE is more aggressive than adult-onset disease,2 3 33 only a few studies on outcome according to onset age have been performed.34,–,36 We did not find any indication of different disease characteristics or treatment according to gender or onset age. This may indicate that age is an independent risk factor for height deflection and growth failure in juvenile SLE. As peak height velocity occurs on average 2 years later in boys than girls28 and SLE onset age was the same, more boys will have disease onset before the pubertal growth spurt, possibly explaining why boys were more growth affected. In a 3-year follow-up study on 57 patients with newly diagnosed juvenile SLE from Italy and Brazil, there was 16% growth failure,37 very similar to 14.7% in females and 24.5% in males in our study.
The observed significant BMI increase with peak at 6 months and with no gender differences was probably due to the higher doses of corticosteroid used to control the active disease at baseline.
No associations were found between the baseline disease characteristics, treatments, growth failure and pubertal delay in males probably due to the small sample and possibly due to the marked difference in growth patterns between boys and girls, with boys having their growth spurt between T3/T4, while girls peak at B2/B3.27,–,29
Multi-ethnicity makes the results more general, but added difficulties to the analyses due to lack of national-based growth references. The 2007 WHO reference21 22 should be used with care in adolescents from different geographic origins.38 Therefore, it was crucial that parent-adjusted height scores were used, thus eliminating the genetic and environmental impact.
Definitions of delayed puberty are a challenge due to secular trends influenced by ethnic and socioeconomic factors.29 39 In a study on 30 Brazilian patients with juvenile SLE and 30 age-matched controls, mean menarcheal age was 13.1 years in patients with SLE versus 11.6 years in controls40. It is plausible that the median menarcheal age of 13.6 years found in our study also represents a delay in pubertal development; indeed 21.9% of the females with premenarcheal disease onset had a definite menarcheal delay (delayed or absent menarche).
Irregular menses or postmenarche amenorrhoea was present in almost half of the evaluable patients. Pubertal delay was found to be higher than the 11% found in a cross-sectional analysis from a partially overlapping cohort,7 emphasising the importance of keeping a longitudinal perspective when studying a chronic condition like SLE.
In the multivariate model, the determinants for growth failure were growth failure at first assessment, cumulative corticosteroid dose (never reported in the literature) and age at first visit; these findings suggest that once a patient has growth failure, it is more difficult to have catch-up growth, while for patient without growth failure, a careful monitoring of the corticosteroid treatment is crucial, especially in patients presenting at younger age.
Limitations of the study include the estimates of cumulative steroid dose and sexual maturation data reported by paediatric rheumatologists, and self-reporting for parent's height. In addition, the use of stadiometers was not standardised, although each patient acted as his/her own control. Moreover, for lack of country-specific information of menarcheal age in a reference population or among mothers or sister(s) of the patients, we could not compare our findings with a Kaplan–Meier curve. However, the large numbers of patients probably outweigh these limitations.
In conclusion, children with juvenile SLE experience a significant loss of height potential and delay in pubertal development over time. The children at risk of having a negative effect on height and pubertal development are prepubertal and peripubertal children treated with >400 mg/kg cumulative dose of corticosteroids. Greater attention should be given to the dose of corticosteroid administered over time in juvenile SLE, especially in boys and in younger girls.
Acknowledgments
The authors wish to thank all the participating physicians, patients with juvenile SLE and their families who devoted their time and patience to participate in the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Funding Funded by a grant from the European Union (contract no. QLG1-CT-2000-00514) and by IRCCS G. Gaslini, Genoa, Italy.
-
Competing interest None.
-
Ethics approval Ethics committees of participating centres as appropriate.
-
Provenance and peer review Not commissioned; externally peer reviewed.