Article Text

Abstract
Background Structural damage of the spine in ankylosing spondylitis (AS) is associated with worse physical function and impaired spinal mobility. Knowledge about predictors of new syndesmophyte formation is limited.
Objectives To assess the development of new syndesmophytes at the level of individual vertebral bodies and to assess predictors for this development.
Methods Clinical and radiological data from 132 patients from the Outcome in Ankylosing Spondylitis International Study for whom complete sets of radiographs were available at baseline and at 2- and 4-year follow-up were used. Univariable and multivariable logistic regression analyses were performed to identify predictors associated with development of new syndesmophytes within 4 years.
Results At baseline, 81 (61%) patients had syndesmophytes. New syndesmophytes developed in 44 (33%) patients within 2 years and in 63 (48%) patients within 4 years. The RR of developing new syndesmophytes was 5.0 (95% CI 2.5 to 10.2) at 4 years in patients with existing syndesmophytes as compared with patients without. In the univariable analysis, older age, worse functional status, male gender, erythrocyte sedimentation rate and existing syndesmophytes were associated with development of new syndesmophytes at 4 years. In the multivariable logistic regression analysis, only the presence of existing syndesmophytes was a significant predictor (OR 18.72, 95% CI 6.44 to 54.42). When existing syndesmophytes were taken out from the model, age (OR 1.07, 95% CI 1.03 to 1.11) and male gender (OR 3.98, 95% CI 1.47 to 10.77) were statistically significant contributors.
Conclusion In AS, patients with existing syndesmophytes are prone to develop new syndesmophytes over time.
Statistics from Altmetric.com
Introduction
Ankylosing spondylitis (AS) is a chronic rheumatic disease characterised by inflammation of the sacroiliac joints and spine and the formation of new bone. One of the hallmarks of AS is the formation of syndesmophytes at the vertebral bodies that may form bridges (ankylosis). When consecutive vertebrae are ankylosed, it may lead to the appearance of a ‘bamboo spine’. Structural damage of the spine is an important outcome measure in AS and is associated with worse physical function and limitation of spinal mobility.1,–,5 Both for clinical practice and for study purposes it is important to know which factors predict radiographic progression in AS. Radiographic damage, in general, is found to be more severe in men and in patients with hip involvement.1,6,–,8 Conflicting results exist with respect to the relation between disease duration and radiographic damage. Some studies reported an association between disease duration and radiographic damage,1 7 9 whereas others failed to demonstrate such an association.10 11
The modified Stoke Ankylosing Spondylitis Spine Score (mSASSS) is a well-validated scoring system for the quantification of structural spinal changes and is currently the preferred method.12 13 It has been demonstrated that changes in the mSASSS are mainly due to the growth of syndesmophytes and ankylosis, which are the most frequent radiographic features of progression in AS.11 However, knowledge about predictors of new syndesmophyte formation in individual patients is limited. Two studies suggested that the presence of syndesmophytes is the best predictor of radiographic progression,11 14 but long-term prospective data on the development of new syndesmophytes and its predictors are currently lacking.
The objectives of this study were to assess the development of new syndesmophytes and/or bridges at the level of individual vertebral bodies and to assess the predictors for development of new syndesmophytes and/or bridges in a prevalence cohort of patients with AS during a 4-year follow-up period.
Methods
The Outcome in Ankylosing Spondylitis International Study is a prevalence cohort including 217 consecutive patients with AS from The Netherlands, Belgium and France that started in 1996.15 16 Patients were followed at regular intervals. For the present study, demographic and clinical data obtained at baseline, and conventional radiographs of the spine obtained at baseline and at 2- and 4-year follow-up were used. The radiographs were scored according to the mSASSS in a chronological time order by a trained expert who was blinded to the demographic and clinical data.17 In the mSASSS, the anterior parts of the cervical and lumbar spine at a lateral view are scored for squaring and/or erosion and/or sclerosis (1 point), syndesmophyte (2 points) and bridging syndesmophyte (3 points). The total score ranges from 0 to 72.12
In the present analysis, we were interested in the formation of new syndesmophytes, which may also include bridging syndesmophytes, at individual vertebral levels. Therefore, a ‘new (bridging) syndesmophyte’ was defined as the development of a syndesmophyte (mSASSS 2 points) or a bridge (mSASSS 3 points) at a vertebral level that was previously uninvolved or with signs of squaring, erosion or sclerosis at baseline only (mSASSS 0 or 1, respectively). A new bridge developing from two existing syndesmophytes during follow-up was considered as the same process and not counted as a ‘new’ syndesmophyte, that is, the syndesmophytes were already present, but only increased in size to form a bridge.
For calculation of the total mSASSS, missing values were substituted by the mean of the score at the other vertebral levels of the same spinal segment of the patient, if the number of missing scoring sites was ≤3.11 13 When more than three scoring sites were missing at a spinal segment at any time point, the patient was excluded from the study. For all analyses at the individual vertebral level, missing values at follow-up were considered as unchanged and substituted by the last observation.
Descriptive statistics were used to calculate the mean with SD for continuous data, and frequencies were calculated for dichotomous data. Independent t tests or non-parametric tests, as appropriate, were used to compare differences between the groups for continuous data and χ2 tests were used for dichotomous data. Univariable and multivariable logistic regression analyses were performed to identify predictors associated with the development of new (bridging) syndesmophytes within 4 years. In the multivariable logistic regression analysis (backward regression method), two models were tested, one with and one without the presence of syndesmophytes at baseline. Interactions between the variables were explored by additional analyses that included the main effect variables and the interaction term for each interaction studied. All analyses were performed using SPSS V.16.0. The significance level was set at 0.05.
Results
For 132 of the 217 patients, complete sets of radiographs with ≤3 vertebral levels missing per spinal segment were available at baseline and at 2- and 4-year follow-up. Baseline characteristics of the total group, as well as by stratification for the presence or absence of existing syndesmophytes, are shown in table 1. In total, 81 (61%) patients had syndesmophytes at baseline. In the group with existing syndesmophytes at baseline, significantly more men were present; patients were older, had longer disease and symptom duration, showed worse function and disease activity, and had higher levels of C reactive protein. One patient at baseline and two patients at 2- and 4-year follow-up had the maximum mSASSS score of 72.
Characteristics of the total group of patients at baseline, stratified for the presence or absence of syndesmophytes at baseline, and comparisons between groups of patients with and without new (bridging) syndesmophytes at 4 years
Progression in mSASSS and development of new syndesmophytes and/or bridges
Progression in the mSASSS score was relatively linear for the total group, but also for the groups with or without existing syndesmophytes at baseline separately (table 2). However, in the group of patients without existing syndesmophytes, the mSASSS was significantly lower and showed less progression over time.
Progression in mSASSS over time for the total group and stratified for the presence or absence of existing syndesmophytes at baseline
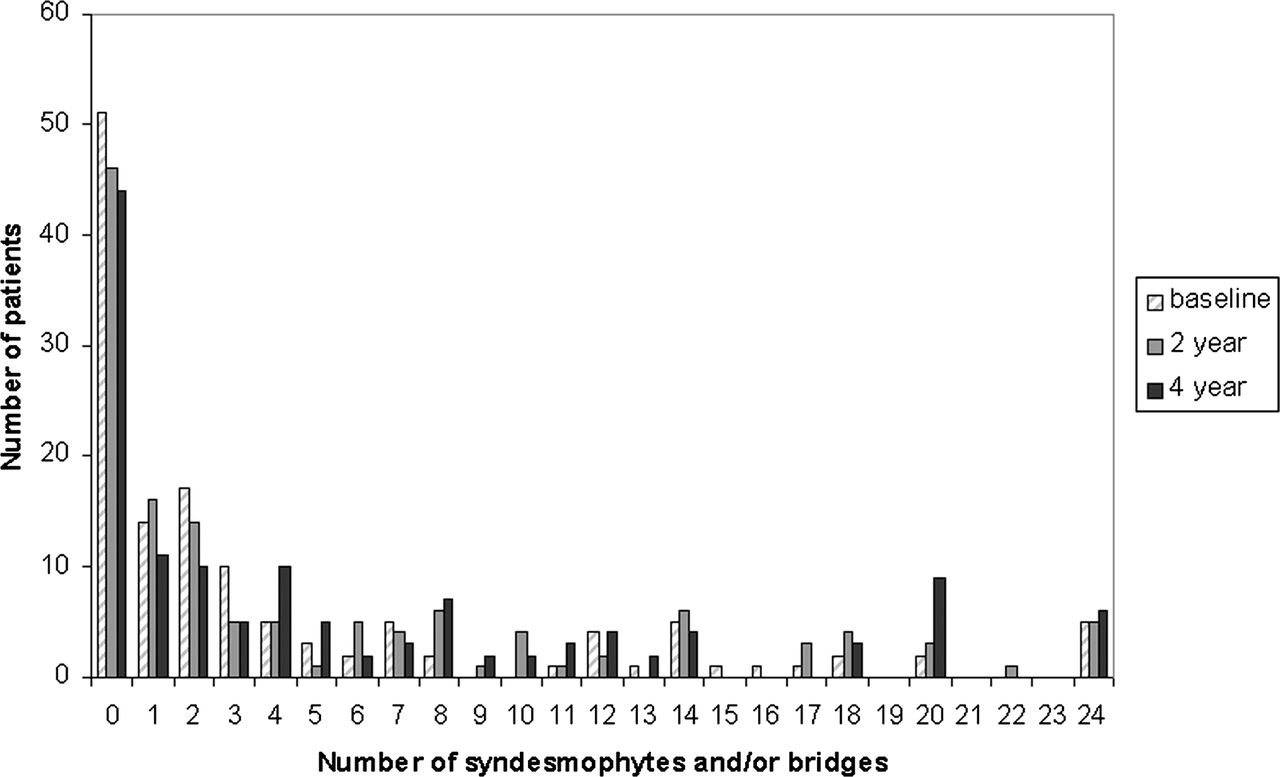
New syndesmophytes and/or bridges developed in 44 (33%) patients within 2 years and in 63 (48%) patients within 4 years. Figure 1 shows the number of syndesmophytes and/or bridges per patient at baseline, 2 years and 4 years. In the group of patients with existing syndesmophytes at baseline, the radiographic progression affected a substantial proportion of the patients; more than half of the patients (51%) had one to three vertebral levels with either a syndesmophyte or a bridge at baseline, but this decreased to 43% at 2 years and 32% at 4 years, indicating progression towards more than three vertebral levels affected with either a syndesmophyte or bridge during follow-up. Moreover, involvement of multiple vertebral levels also increased, for example, at least 10 vertebral levels were affected with either a syndesmophyte or a bridge in 23 (28%) patients at baseline, in 29 (36%) patients at 2 years and in 34 (42%) patients at 4 years.
Table 3 shows the mean number of syndesmophytes and bridges per time point for the total group, and separately for the groups with or without existing syndesmophytes at baseline. In the total group, new syndesmophytes or bridges occurred at a rate of 0.91 per 2 years from baseline to 2 years and at a rate of 0.73 per 2 years from 2 to 4 years. In the group of patients without existing syndesmophytes at baseline, the mean progression rate was 0.12 per 2 years from baseline to 2 years and 0.25 per 2 years from 2 to 4 years. In the group of patients with existing syndesmophytes at baseline, however, the mean progression rate was 1.42 per 2 years from baseline to 2 years and 1.02 from 2 to 4 years. The rate of development of new syndesmophytes at either the cervical spine or the lumbar spine was not significantly different at any time point.

{kind=link}
The number of syndesmophytes and/or bridges per patient at baseline, 2 years and 4 years.
Number of syndesmophytes and/or bridges per time point in the total group, and stratifi ed for the presence or absence of existing syndesmophytes at baseline
The risk of progression and determinants of new syndesmophytes and/or bridging
In the group of patients with existing syndesmophytes at baseline, 39 (48%) patients at 2 years and 56 (69%) patients at 4 years developed new syndesmophytes and/or bridges in previously uninvolved vertebral levels or in sites with signs of squaring, erosion or sclerosis at baseline (mSASSS score of 0 or 1, respectively). In the group of patients without existing syndesmophytes at baseline, five (10%) patients at 2 years and seven (14%) patients at 4 years developed new syndesmophytes in previously uninvolved vertebral levels or in sites with signs of squaring, erosion or sclerosis at baseline (mSASSS score of 0 or 1, respectively). Bridging did not occur in the latter group. The RR of developing new (bridging) syndesmophytes was 4.9 (95% CI 2.1 to 11.6, p<0.01) at 2 years and 5.0 (95% CI 2.5 to 10.2, p<0.01) at 4 years for patients with existing syndesmophytes as compared with patients without.
Table 4 shows the number of patients, mean symptom duration and disease duration per total number of new syndesmophytes and/or bridges at 2 and 4 years. Within 2 years up to 10 and within 4 years up to 16 new syndesmophytes and/or bridges developed in single patients. However, the majority of the patients with new syndesmophytes developed ≤3 new syndesmophytes and/or bridges within the 4-year time frame. Overall, the symptom and disease duration since diagnosis were more or less equally distributed over the total number of new syndesmophytes and bridges that had developed. Interestingly, even in patients with a mean symptom duration of 44 years, new syndesmophytes developed. In the seven patients without syndesmophytes at baseline who developed new syndesmophytes during 4 years of follow-up, the mean symptom duration was 22.0 years (SD 12.3, range 7.0–39) and the mean disease duration since diagnosis was 10.7 years (SD 4.5, range 6.0–17.0) at baseline.
Number of patients, mean symptom duration and disease duration per total number of new syndesmophytes and/or bridges at 2 and 4 years
Table 1 also shows the comparisons between the groups of patients with and without new syndesmophytes and/or bridges within 4 years. Patients with new syndesmophytes and/or bridges at 4 years were significantly older, had a worse functional status, were more frequently men, had higher levels of erythrocyte sedimentation rate (ESR) and had more frequently syndesmophytes and/or bridges at baseline. In the univariable logistic regression analysis to identify predictors for the development of new syndesmophytes and/or bridges at 4 years (table 5), except for ESR, the same variables were statistically significant. Subsequently, two prediction models were tested. In the first model, all variables with p values below 0.10 in the univariable analysis were included. The only significant predictor was the presence of baseline syndesmophytes (OR 18.72, 95% CI 6.44 to 54.42). In the second model, the presence of syndesmophytes at baseline was taken out. Only age (OR 1.07, 95% CI 1.03 to 1.11) and male gender (OR 3.98, 95% CI 1.47 to 10.77) were statistically significant contributors. Interaction between the variables was not found.
Univariable and multivariable analysis of the development of new (bridging) syndesmophytes at 4 years
Discussion
In this prevalence cohort of consecutive patients with AS, nearly half of the patients developed new syndesmophytes and/or bridges within 4 years. The progression rate was significantly higher in patients with existing syndesmophytes as compared with those without. Although the progression rate seemed to be relatively linear at the group level, in individuals large differences were found, ranging from 0 to 16 new syndesmophytes and/or bridges per patient within 4 years. Only the presence of (bridging) syndesmophytes at baseline was found to be a strong predictor for the development of new syndesmophytes and/or bridges within 4 years.
In our study, new syndesmophytes and/or bridges were found in 33% of the patients within 2 years (48% in the group with existing syndesmophytes at baseline vs 10% in the group without) and in 48% of the patients within 4 years (69% vs 14%). Similar results with respect to new syndesmophyte formation were found in two other studies.11 14 In the first study, 31% of a total group of 116 patients developed new syndesmophytes within a 2-year period, in 44% of the patients with (bridging) syndesmophytes at baseline and in 19% of the patients without (bridging) syndesmophytes at baseline.11 In a second retrospective study with a mean follow-up of 3.8 years, 58% of a total group of 146 patients developed new syndesmophytes.14 The mean number of new syndesmophytes was 1.8 per patient, which is comparable to a mean number of 1.6 per patient after 4 years in our study. The limitations of this study, however, were the retrospective design and not for every patient radiographs and clinical data were available at all time points. Our prospective study in which the data were systematically collected confirms that the progression rate of developing new syndesmophytes is faster in patients with syndesmophytes and/or bridges at baseline.
This study indicates that radiographic progression occurs in a selected group of patients. The presence of syndesmophytes at baseline was found to be the only significant predictor for the formation of new syndesmophytes over time. Only when the presence of syndesmophytes at baseline was taken out from the model, age and male gender were modest, but statistically significant predictors for the formation of new syndesmophytes over time. None of the other demographic or clinical variables could predict the development of new syndesmophytes. With this observation, it is suggested that a subgroup of patients exists in which syndesmophytes can appear and that this subgroup of patients can only be recognised by the presence of syndesmophytes. Once the syndesmophytes are present, the development of new syndesmophytes seems to be a continuing process. It is, however, arguable whether the presence of baseline syndesmophytes should be considered as a true predictor because the patient already exhibited the features that the model wants to predict. In fact, syndesmophytes at baseline may be seen as an autoregressive predictor; the ominous presence of baseline damage itself evokes an extension of damage over time.18 Furthermore, for daily clinical practice the presence of baseline syndesmophytes will not be a helpful predictor. A substantial proportion of these patients did not show progression within 4 years in our study. Moreover, the time at which progression occurs seems to be unpredictable. Our study confirms earlier observations that although at the group level radiographic progression is close to linear, in individuals the rate of progression varies strongly, with some patients showing no progression at all whereas other patients show bursts of rapid change in a short period of time.14 19
It is commonly believed that patients who show no spinal damage after a disease duration of approximately 10 years will most likely never develop radiographic abnormalities of the spine.20 In our study, six out of seven patients without existing syndesmophytes at baseline who developed new syndesmophytes during 4 years of follow-up had a symptom duration of more than 10 years (range 14–39 years) when the first syndesmophyte(s) appeared. Moreover, even after a symptom duration of 44 years, patients may still have a (rapid) growth of new syndesmophytes (table 4). Brophy et al19 also found that periods of rapid change in progression can occur at any time in the course of the disease, even after 10 years of the disease.
With respect to the reading of the radiographs, the following points should be noted. First, the radiographs were read by one expert only. In trials, it is common practice to have the radiographs read by two independent readers after which consensus is reached or average scores are used. However, for the present study it was practically difficult to deal with differences between readers at each individual vertebral level. Therefore, we decided to use the data from one expert reader only. The same data set was read several times by this expert in previously conducted studies.4 13 17 Second, the radiographs were read in chronological order. It is known that the order in which films are evaluated influences the results.17 In our study, we found an increase of 2.5 in the mSASSS in 2 years time, which is higher than the average of 0.9–1.0 progression in the mSASSS found in several trials of AS that used paired reading.21,–,23 The greater signal found when reading films in chronological order could be due to true progression or due to ‘noise’, for example, by expectation bias. On the other hand, the disadvantage of paired reading is the possibility of negative scores, which are considered a measurement error, since repair probably does not occur in AS. We deliberately chose to use chronological reading to increase the ability to detect changes in our study. Also in rheumatoid arthritis, scoring in chronological order is frequently used to answer epidemiological questions.24 25 For trial purposes, however, paired reading is recommended by regulatory authorities in order to prevent any possible bias.
The true cause of structural damage in AS still remains unknown. Two main hypotheses have been put forward suggesting that both inflammatory and mechanical components play an important role in local new bone formation.26 27 Using MRI investigations it has been shown that sites with active inflammation appear to be more prone to later development of syndesmophytes.28,–,32 However, most syndesmophytes appeared at sites without apparent inflammation and not all inflammatory lesions automatically lead to syndesmophytes. An interesting observation in this context is that trials with tumour necrosis factor α blocking agents failed to demonstrate a reduction in the development of new syndesmophytes.21,–,23 It is questionable whether low-grade inflammation may still be present, which is undetectable by MRI, or whether there is a role for a non-inflammatory pathway, for instance, by mechanical stress. In the past few years several hypotheses have been postulated, suggesting that inflammation and new bone formation are in fact partly uncoupled in AS.26 27
In conclusion, the development of new syndesmophytes in AS occurs in general at a slow rate, but in individuals a large variation can be found. The rate of progression is significantly faster in patients with existing syndesmophytes as compared with those without. Unlike in rheumatoid arthritis, radiological progression in AS cannot be predicted by variables classically associated with disease severity and disease activity. Patients with existing syndesmophytes are prone to develop new syndesmophytes and/or bridges over time, although it is arguable whether this should be considered as a true predictor.
References
Footnotes
-
Funding SR was supported by the Fundação para a Ciência e Tecnologia (FCT) grant SFRH/BD/68684/2010.
-
Competing interest None.
-
Ethics approval The study was approved by ethics committee from Maastricht University Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.