Article Text

Abstract
This study reviewed the effect of biological agents on participation in paid work among patients with rheumatoid arthritis (RA). A systematic literature search was performed to identify published articles reporting the effect of biological agents on employment status, sick leave and/or presenteeism. The quality of included articles was assessed according to the guidelines as proposed by the Dutch Cochrane Centre. Narrative summaries were used to present the data separately for randomised controlled trials (RCTs) as well as controlled and uncontrolled cohort studies. 19 studies (six uncontrolled cohorts, seven controlled cohorts and six RCTs) were included, in which 11 259 patients were treated with biological agents. Employment status improved in four out of 13 studies, absence from work in all 10 studies and presenteeism in seven out of nine studies that reported this outcome. For absenteeism and presenteeism the statistical significance of change or difference was not always provided and results within studies were sometimes conflicting when using different time frames or alternative outcomes. The large heterogeneity in terms of population, design, analyses and most important in outcome measures limits interpretation of the data. RCTs as well as cohort studies showed positive results of biological agents on both absenteeism and presenteeism compared with other disease-modifying antirheumatic drugs (DMARD), continuing the failing DMARD, the general population or the situation before the start of biological agents. The effect on employment status was more conflicting, but 50% of studies that addressed patients with early methotrexate-naive RA showed a positive result on employment status.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic inflammatory disease that can limit daily activities of patients, but can also restrict participation in major life areas including work participation.1,–,3 Worsening of the disease might finally result in withdrawal from the labour force, either because of official work disability, early retirement or self-perceived disability.1 2 4
The outcome of RA has changed since the introduction of biological agents. The addition of biological agents in treatment strategies for RA have improved the possibility of controlling disease activity5,–,10 and slowing the progression of joint damage.11 However, the prices of these drugs are high and several studies have proved that the use of these medications increases the overall (direct) healthcare costs of RA, despite savings in cost categories such as hospitalisation.3,12,–,14 On the other hand, it is known that the indirect costs of RA exceed direct healthcare costs. Beneficial effects of biological agents on work participation can therefore offer an opportunity to offset drug costs by savings in indirect costs.15 As such, it is pivotal to understand the effect of biological agents on work participation in terms of (short and long-term) absenteeism and work restrictions while at work (presenteeism) as this is the basis to calculate indirect costs. This study reports on a systematic review of published articles that aimed to quantify the effect of biological agents on three domains of participation in paid work that are relevant for productivity costs, encompassing presenteeism (reduced work input while at work), sick leave and employment status (work disability), independent of study design.
Methods
Search strategy
A systematic search of the literature (Pubmed and Embase/Medline) was performed to identify articles from 1971 to January 2011 (last updated 30 December 2010) that quantified the effect of antitumour necrosis factor (TNF) α treatment on presenteeism, sick leave and/or employment status in patients with RA. Search terms comprised three blocks that were combined. The first block addressed the disease (RA), the second the intervention (biological agents) and the third the outcome (work participation). Articles were limited to human studies in the Dutch, English, French or German language. The detailed search strategy is available in supplementary appendix 1, available online only.
Article selection
One author (MMtW) performed an initial screening of titles and abstracts, including only those reporting a direct effect of biological therapy on participation in paid work in RA patients. Full text articles of the selected titles were screened using the same inclusion criteria. If there was doubt as to whether a particular article should be included, the author discussed the article with the last author (AB) until consensus was reached. References of the retrieved articles were scanned for additional studies.
Quality assessment
The quality of selected articles was assessed using three checklists (for controlled cohort studies, uncontrolled cohorts and randomised controlled trials (RCTs)) from the Dutch Cochrane Collaboration (figure 1).16 Criteria had three answer options: yes (adequate information/approach); no (no adequate information/approach); or little information. Two criteria were added to the checklists as the authors considered these criteria to be important to interpret the results: available information on recall period for outcome measures (yes/no) and information on attribution of work outcome (due to arthritis or overall health, yes/no). The results of these extra questions are shown in the result tables under outcome measures. For ‘duration of follow-up period’, the authors defined a period of a minimum of 1 year as adequate when employment status was the work outcome and 6 months for absenteeism and presenteeism as the short-term outcome is economically less relevant.17 For RCTs original papers reporting primary outcomes were retrieved to check for additional information if data to answer specific criteria of the checklist were missing. Two authors (MMtW and AB) assessed the quality of the articles independently. Discrepancies between both authors were discussed until consensus was reached.

Quality checklists for cohort, randomised controlled trials (RCTs) and case–control studies. RA, rheumatoid arthritis.
Data extraction
Data were extracted by one author (MMtW) using a self-composed form including the following items: design (RCTs/controlled studies or uncontrolled cohort); population (eg, gender, age, number employed, disease duration); type of intervention; statistical methods; and results. Whenever possible absolute changes were presented to reflect differences between two groups (biological agent opposed to control) or two time points (before and after). The data extraction was checked by a second author (AG).
Statistical analysis
A meta-analysis to assess the overall effect of biological agents on work participation in RA could not be performed due to extended heterogeneity with respect to study populations, outcome measures and statistical analysis. Therefore, narrative summaries are provided.
Results
Study selection and inclusion
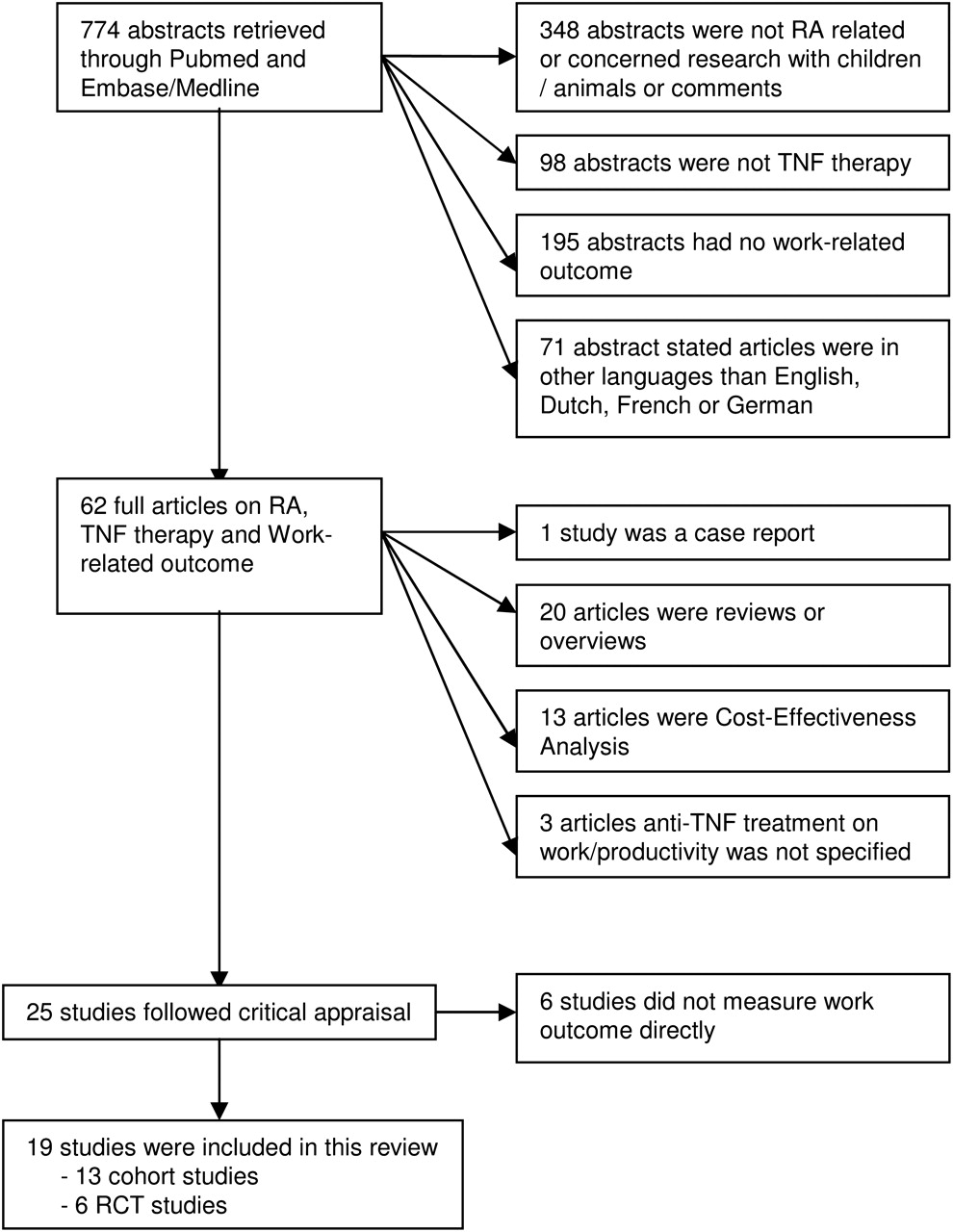
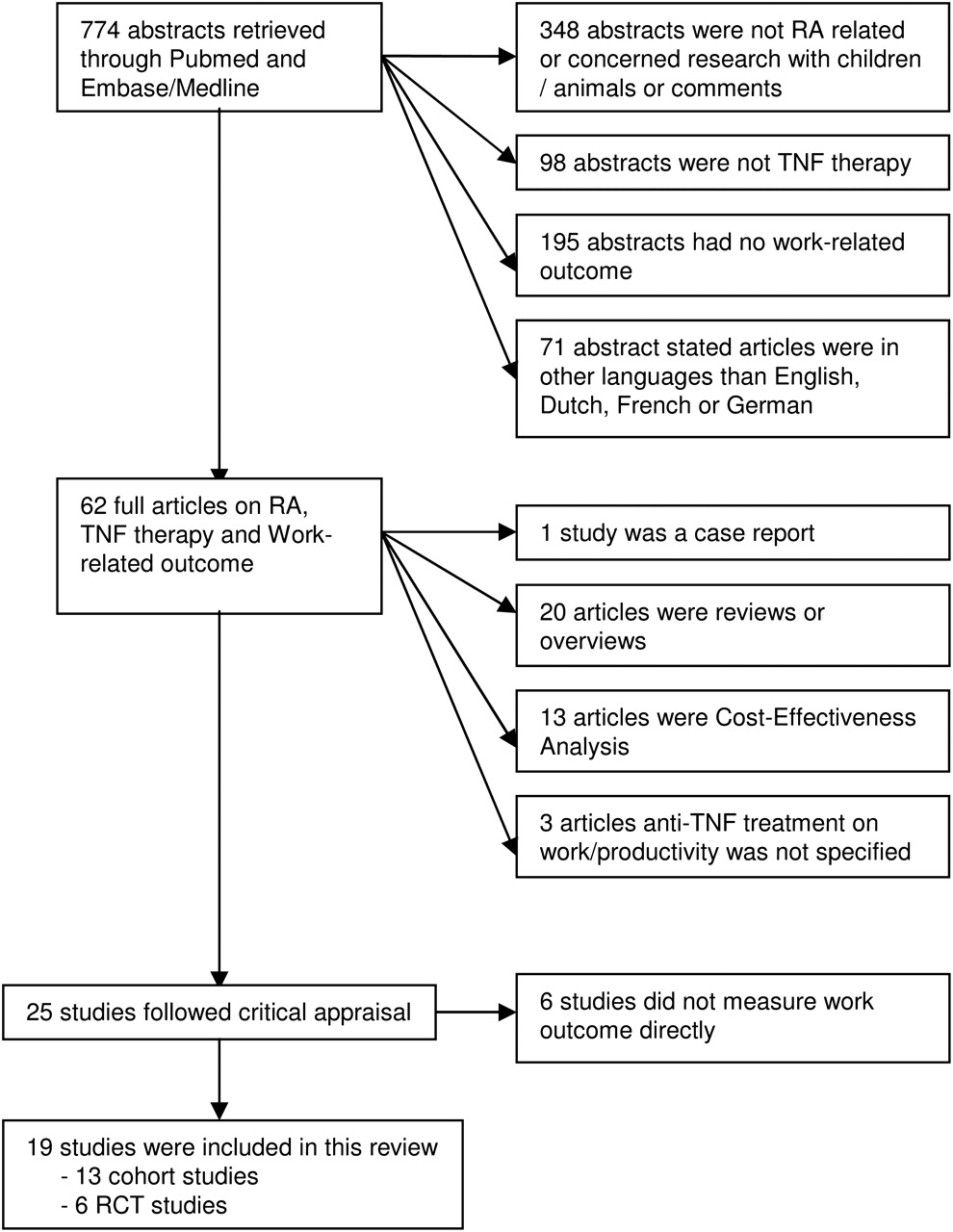
A total of 774 titles was identified after the electronic search. Sixty-two articles were selected for full text review as shown in the flowchart in figure 2. Eventually, 25 full text articles were selected for quality assessment. Six additional articles were excluded as they did not report the direct effect of biological agents on work productivity, but the relation between treatment response and work outcome independent of treatment assignment.2,18,–,22 Finally, 19 articles were included: six uncontrolled cohorts,23,–,28 seven controlled cohorts4,29,–,34 and six RCTs.10,35,–,39
{kind=link}
{kind=link}
Flowchart of study selection and inclusion. RA, rheumatoid arthritis; RCTs, randomised controlled trial; TNF, tumour necrosis factor.
Study results
In total 11259 patients were treated with biological agents: 8015 in cohorts and 3244 patients in RCTs. Ten studies (all controlled or uncontrolled cohorts) were single country studies with six performed in Europe and four in USA/Canada. Nine studies were multinational (three cohorts and six RCTs) with countries from Europe, USA, Canada and Australia. Almost all studies used self-reported outcome measures except for two controlled cohorts. In uncontrolled cohorts, patients had an average age of 51.6 years and average disease duration of 10.9 years. For the controlled cohorts this was 51.1 and 11.8 years, respectively, and for RCTs 50.5 and 4.5 years, respectively. The biological agents considered were TNFα inhibitors in 18 articles, etanercept in three, adalimumab in seven, infliximab in one, certolizumab pegol in one or different biologicals seen as a group in six articles. One study reported effects of abatacept on work.
Tables 1–3 show the results of uncontrolled cohorts, controlled cohorts and RCTs, respectively. Controlled cohorts are ordered by comparator: general population (n=1), or continuation of usual care with disease-modifying antirheumatic drugs (DMARD). RCTs are ordered by comparator: methotrexate in methotrexate-naive patients or methotrexate/DMARD continuation in methotrexate/DMARD or anti-TNF failures. Within each design, studies are ranked according to the date of publication. In the last column of these tables, the letters correspond to the criteria (figure 1) with a negative/inadequate quality score or with insufficient information (in brackets).
Characteristics and results of uncontrolled cohort studies reporting the impact of biological agents on work participation
Characteristics and results of controlled cohort studies reporting the impact of biological agents on work participation
Characteristics and results of RCTs reporting the impact of biological agents on work participation
Employment status
Employment status was the most frequently explored work outcome: nine out of 13 cohorts4,23,26,28,29,31,–,34 and five of six RCTs.35,–,37,39,40 Follow-up varied from 12 to 104 weeks.
One uncontrolled cohort study showed a temporary positive effect after 1 year treatment (mean +4.1 h/week), but this effect was lost after 5 years.23 The remaining two uncontrolled studies showed no effect.26 28 Two controlled cohorts showed that employed anti-TNF-treated patients worked an additional 0.61 years or that 20% more patients remained employed compared with the control group that started methotrexate/leflunomide or continued usual care, respectively31 34 Another controlled cohort study showed no effect of biological agents versus matched controls receiving usual care (DMARD), but a positive effect on employment status in patients with short disease duration (<11 years) was seen.29 The three remaining controlled cohorts, one of which used the general population as control, showed no effect.4 32 33
Two out of five RCTs showed a positive effect on employment status after 52 and 104 weeks of treatment with a biological agent, both in methotrexate-naive patients starting methotrexate monotherapy as the active comparator.35 39 One of these studies showed a significant positive effect (OR 1.554; 95% CI 1.004 to 2.405) on maintaining or gaining employment in patients receiving adalimumab plus methotrexate, but not for those receiving adalimumab monotherapy (OR 1.285; 95% CI 0.837 to 1.972).39 It is of note that in that study not only regaining employment but also remaining at work was contained in the definition of treatment success. A conflicting result on job loss was reported for abatacept in methotrexate or anti-TNF failures, when the response of the physical component of the short form 36 (SF-36) was mapped on job loss as seen in a historic population study.37 The two remaining RCTs (follow-up between 54 and 56 weeks) showed no effect of adalimumab or infliximab when compared to methotrexate in methotrexate failures.36 40
Absence from paid work
Absence from work was the outcome that most frequently showed a favourable effect of biological agents. Six out of 13 cohort studies25,–,28,30,32 and four of six RCTs35,38–,40 quantified the effect of biological agents on absenteeism. Follow-up varied from 12 to 104 weeks.
All cohort studies reported a reduction in absence from work. Four studies were uncontrolled25,–,28 and two controlled, one of which used a general population as comparator32 and one compared anti-TNF with usual care with DMARDs.30 In the uncontrolled studies improvements ranged from 0.5 days in 1 year in the total group (workers and non-workers),26 to 0.5 days in the past 2 weeks after 12 weeks in those with paid work.28 The general population controlled study reported a decrease of RR (decreased from 6.6 to 5.1) for being on sick leave during the first year after the initiation of biological agents when compared with general population data, but compared with 1 year before treatment no difference was noticed.32 This suggests patients returned to the sick leave rate before the increase of sick leave surrounding the initiation of biological agents. Moreover, only completers were included in this analysis.
All four RCTs assessing absenteeism showed a reduction by biological agents in absence from paid work compared with methotrexate monotherapy in naive patients35 39 40 or continuation of methotrexate in methotrexate failures.38 Reduction by biological agents in days of sick leave ranged from 2.1 days in the past 4 weeks38 to 18.7 days in 2 years,39 and more patients treated with infliximab had no days absent compared with the control group (78.9% vs 66.6%, respectively, p<0.01).40 In a trial in methotrexate failures, certolizumab pegol was not able to reduce absenteeism significantly after 24 weeks of treatment (RAPID 2), but after a 52-week follow-up (RAPID 1) a small but significant reduction in absenteeism was seen (a mean decrease of two work days).38
Presenteeism
Presenteeism was reported in five out of 12 cohort studies,24 25 27 28 30 and four of six RCTs.35 36 38 39 Follow-up varied from 24 to 144 weeks.
Three uncontrolled cohort studies showed an improvement in presenteeism ranging from 1.0 to 2.46 (0–10 on a visual analogue scale (VAS)).24 25 27 A last uncontrolled cohort showed conflicting results: positive when using an efficiency score on a VAS (improvement of -1.4 (SE 2.8)), but not when using extra hours needed to work to complete unfinished work as a surrogate for presenteeism.28 One controlled cohort study (follow-up of 52 weeks), in which controls continued usual care with DMARD, provided conflicting results. It showed that beneficial effects after 6 months of treatment with etanercept were not maintained after 1 year.30
Three RCTs reported a significant (small) improvement in presenteeism, two when comparing either etanercept or adalimumab with methotrexate monotherapy in methotrexate-naive patients35 36 or certolizumab pegol with continuing methotrexate in methotrexate failures.38 Improvements compared with methotrexate ranged from 1.4% using the work limitations questionnaire to three points on a VAS (0–10). A conflicting result was seen with adalimumab as the combination of adalimumab and methotrexate in early, methotrexate-naive patients reduced presenteeism significantly compared with methotrexate monotherapy (p<0.05), while adalimumab monotherapy was not able to improve presenteeism significantly.39 One of these studies estimated presenteeism indirectly by mapping health assessment questionnaire (HAQ) changes on presenteeism as measured in another trial.6 35
Discussion
This study reviewed all published articles that quantified the direct effect of biological agents on employment status, sick leave or presenteeism in patients with RA. As shown in table 4, biological agents have overall a positive effect on absence from paid work and presenteeism compared with the situation before the start (n=7), the general population (n=1), or similar groups starting or continuing usual care with DMARD (n=9), while the effect on employment status remains undecided.
Overview of the results
The main challenge of this review was the heterogeneity in study design, work-related outcomes and patients included, hampering comparability. While we specifically aimed to include studies from all designs, each has advantages and limitations. RCTs typically have low external validity and follow-up is often too short to be relevant with regard to work outcome. Moreover, several RCTs with biological agents were performed in DMARD-failing patients using a control group without active treatment. Of specific concern for RCTs was also that work participation was a secondary outcome in all but two studies.35 36 As a consequence, sample sizes could have been too small to show effects on employment status. Finally, in the analyses often the between-group differences were not tested or presented. Although uncontrolled cohorts may be more generalisable and more informative with respect to the duration of the effect on work outcome, the absence of a control group cannot exclude regression to the mean as a cause of improvement, because patients are likely to start with biological agents when the disease flares. Also, results of uncontrolled cohorts might not be different from the expected course of intensive DMARD treatment. While the inclusion of an RA control group could adjust for the effect of non-biological treatments (eg, non-biological DMARD), such studies cannot adjust for societal effects on the occurrence of sick leave and employment perspectives. This was shown in the study by Olofsson et al,32 who demonstrated that the risk of sick leave in patients, compared with the general population, decreased after the start of biological agents, but stabilised after 1 year on a level that was even higher than 1 year before the start of biological agents. Work outcomes can also be influenced by differences per country in legislation and changes in these legislations. Only this population study could take this into account.32
Almost all studies used different approaches to assess work outcome comprising self-composed questionnaires, validated instruments or existing databases reporting on work outcomes. Although 24 instruments are available to assess absence from work and/or presenteeism, only few a studies used one of these instruments (work productivity and activity impairment questionnaire, RA work impact scale, work productivity survey—RA, work limitations questionnaire, workability index and health and labour questionnaire).24 25 28 35 36 38 Even then, comparability remains limited as these instruments also differ in recall, concepts of absenteeism and presenteeism and whether or not impact on work should be attributed to RA or overall health. Moreover, some studies presented results on a group level (means/median) while others on the individual patient level (proportion of patients with sick leave or presenteeism). Also, most studies used different definitions to describe employment status such as: being employed, additional years worked, work disability rate (official or self-perceived) and job loss. For example, one study defined employment status as differences between groups in gaining or remaining employed.39 Another study reported on hours working per week, which made it unclear whether this referred to employment status (contract hours) or also included productivity loss due to sick leave.23 34 Of interest were two studies that had not included a work outcome measure, but mapped health effects of SF-36/HAQ on those of another study that included a work outcome measure as well as SF-36/HAQ. As such, they could indirectly compare the effect of biological agents on work.35 39 Last but not least, the clinical relevance of effects is difficult to interpret because no efforts have been made to define minimal relevant differences for work outcomes.
Six articles were excluded from this review because they quantified the relation between response measures (eg, disease activity score in 28 joints, HAQ, American College of Rheumatology/European League Against Rheumatism response) and work outcome as an indirect consequence of treatment with biological agents, independent of treatment allocation.2,18,–,22 These studies suggest that a main effect of biological agents on work participation is mediated by an improvement in disease. Whether biological agents have an additional effect compared with non-biological DMARDs, independent of the effect on improvement of disease activity and physical function, remains incompletely resolved because only few of the studies in this review compared TNF with intensive DMARD treatment.41
A last issue limiting comparability concerned the study populations. For example, inclusion was sometimes limited to those of working age (18–64 years) or to those being employed. Within studies, subgroups were often selected to report different outcomes. While results on sick leave and presenteeism were usually reported for those employed, measures on employment status were often reported for the total group. Also, populations differed in risk of change in work participation and therefore reversibility of restrictions in work participation. In longstanding DMARD-resistant RA, it is likely that a large proportion of patients already withdrew from work. This reduces the chance of biological agents further decreasing withdrawal rates. Moreover, return to work for persons with longstanding work disability is unlikely. In contrast, for patients with early active RA there might be ‘a window of opportunity’ for biological agents to reduce adverse work outcomes.37 This seems likely in this review in which two of the four studies in early methotrexate-naive patients,35 39 and a subgroup analyses of patients with shorter disease duration in a cohort study,29 showed positive effects on employment status.
Four studies (two uncontrolled studies27 28 and two RCTs38 39) assessed the effect of biological agents on unpaid work. All four studies showed improvement in unpaid work, but the change over time or differences between groups was only significant in three studies28 38 39 (see supplementary appendix 2, available online only).
The checklists of the Dutch Cochrane Collaboration had some limitations, specifically when trying to decide on the relative importance of the different criteria.16 First, and as discussed above, it is difficult to judge whether evidence from RCTs weighs more or less than evidence from controlled cohorts. Also within one type of design, the relevance of the individual criteria are not difficult to weigh out against each other. For example, the study of Zhang et al28 could be considered a good quality cohort study (almost no questions with no or less information), but the follow-up period of that article is only 12 weeks, making it economically less relevant. Finally, some attributes of the outcomes could not be appraised for quality. As the recall period and the disease attribution (overall health or RA specific) were considered important to interpret the results, these criteria were added. As expected, these criteria often received a negative score. It is difficult, however, to hypothesise how this would influence the results. Criteria that most often scored negatively were the assessment of appropriate confounders and incomplete follow-up of cohort studies (letters H and G). It was also striking that important determinants or confounders for work-related outcomes such as educational level and job-related characteristics were never reported as baseline characteristics nor added as explanatory factors in further analyses. In line with this, it is noteworthy to mention that the impact of treatment on mortality in employed patients should also be considered when trying to understand the incremental lifetime (economic) impact of biological agents on work outcome.
In conclusion, although no pooled effect size could be calculated due to the heterogeneity of all data, almost all studies showed positive results of biological agents on absenteeism and presenteeism compared with start/continue usual care with DMARD, the general population or the situation before starting biological agents. The effect on employment status was more conflicting, with only a fifth of the cohort studies reporting a positive result, opposed to 40% of the RCTs. It seems of interest that 50% of studies that assessed early methotrexate-naive patients showed a positive result on employment status. To enhance the comparability of studies, consensus on preferred outcome instruments and recommendations on the conduct and reporting of studies on work participation is recommended.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.