Article Text

Abstract
Background Hand osteoarthritis (HOA) is a common disease that affects up to 40% of adults and may severely impair their health-related quality of life (HRQL).
Objectives To assess how HRQL has been evaluated in HOA, focusing on a comparison of HRQL impairment in HOA and rheumatoid arthritis (RA), differences between erosive and non-erosive HOA and differences between OA of the thumb base (TB) and interphalangeal (IP) OA.
Methods A systematic review of the literature.
Results The authors screened 167 articles and retained 33. The outcome subsets usually reported were pain, function and stiffness. Overall HRQL was rarely assessed and the tools used differed greatly. Aesthetic damage was never studied in published articles, although this is a major complaint in daily practice. Three articles compared symptomatic HOA and RA; whereas pain and subjective health did not differ significantly, there is conflicting evidence of the difference between disability and stiffness between these groups. Two papers compared erosive and non-erosive HOA and found divergent elements concerning functional impairment; patients with erosive HOA reported more aesthetic damage. Three papers compared TB and IP OA with divergent results in terms of pain and function.
Conclusion Overall HRQL is a broad concept involving domains beyond pain, function and stiffness. Few data are presently available on HOA, but it seems to have almost as great an impact as RA on HRQL. Further studies on HRQL in patients with HOA are required. Aesthetic damage should also be assessed with specifically designed tools.
Statistics from Altmetric.com
Introduction
The epidemiology of hand osteoarthritis (HOA) is complex because there is no agreed definition of the disorder. HOA is a widespread disease for which the estimated prevalence varies depending on whether a radiological or clinical definition is used. Cohort studies have shown that up to 51% of women over the age of 65 years suffer from radiologically-defined HOA,1 and symptomatic disease is present in 20–40% of patients with radiological HOA.2,–,4
Primary HOA usually involves the distal interphalangeal (DIP), proximal interphalangeal (PIP) and first carpometacarpal (CMC) joints. DIP joints are the most prevalent site of radiological involvement, followed by CMC and PIP joints. The distribution of the sites of symptomatic HOA varies from one population-based study to another.2,–,5
Erosive HOA is a special entity that affects interphalangeal (IP) joints. It is a radiologically defined subset of HOA characterised by erosion of the subchondral bone plate in the centre of the joint. It may be accompanied by painful inflammatory flares.6 7
The contribution of HOA to the impairment of health-related quality of life (HRQL) is unclear. We need to know more about this common disease in order to improve its management. HRQL is a very wide multidimensional concept covering several domains. The World Health Organization (WHO) defined quality of life as ‘an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns. It is a broad ranging concept affected in a complex way by the person's physical health, psychological state, level of independence, social relationships, and their relationship to salient features of their environment’.8,–,10
It is important to assess the health and quality of life of patients with rheumatic diseases for health service research, epidemiological studies, clinical trials and clinical practice. It should be used to evaluate the benefits of healthcare and target therapeutic interventions. It is also relevant for the preoccupations of individual patients since physiological measures are often poorly correlated with well-being.
The consensus work of the Outcome Measures in Rheumatology Clinical Trials Group (OMERACT) recommended pain, physical function and patient global assessment as key outcomes in knee, hip and hand OA in clinical trials.11,–,13 Although these outcomes are of major importance for assessing health, they do not adequately reflect HRQL in all its dimensions.
The Osteoarthritis Research Society International (OARSI) recommended measuring HRQL in HOA.14 However, it was not clear how HRQL should be assessed. There are some potentially useful instruments, all of which require validation. These include the Short Form 36 Health Survey (SF-36),15 16 the Sickness Impact Profile,17 the Nottingham Health Profile18 19 and EuroQol.20 21 Utility could be measured using the EuroQol or Health Utilities Index.20,–,23
This study reviews the published reports on the evaluation of HRQL in HOA.
Methods
Objective and outcome assessments
The primary aim was to provide an overall picture of the assessment of HRQL in HOA. The secondary aim was to focus on the following questions:
1. How comparable is HRQL in HOA and rheumatoid arthritis (RA)?
2. Does HRQL differ in erosive and non-erosive HOA?
3. Do thumb base (TB) and IP OA have different effects on HRQL?
Literature search
We systematically reviewed the published literature in English or French using the MeSH thesaurus in the MEDLINE database (PubMed). The selection was performed by one researcher. The search was restricted to adult humans without any date restriction (included articles published until June 2009). The search request combined ‘osteoarthritis’ and [‘hand’ or ‘hand joints’] and [‘hand strength’ or ‘disability evaluation’ or ‘pain measurement’ or ‘health status indicators’ or ‘pain’], not ‘orthopaedic procedures’. Additional research using ‘quality of life’ yielded no more references.
Relevant articles were selected in a five-step approach: (1) references identified by titles and abstracts were screened to exclude articles not dealing with the topic of interest; (2) clinical trials were excluded; (3) reviews and case reports were excluded; (4) the full paper of selected articles was reviewed and off-board papers were excluded; (5) references of the finally selected articles were hand-searched for additional relevant publications.
Each article was analysed using a standard format to assess the quality and extract the data. Extracted data were as follows: study design, primary/secondary outcomes, sample size, demographic data (gender, age, ethnicity, laterality, age at menarche, menopausal status, menopause duration, hormonal substitution duration, pregnancies, weight, size, body mass index, occupation, manual leisure, quantification of tobacco consumption, treatments for HOA), assessed joints (one or both hands, IP and/or TB), diagnosis (clinical, radiological), symptom duration, assessed outcomes (pain, function, stiffness, aesthetic, mood, fatigue, global HRQL, others) and tools used for outcome assessment.
Statistical analysis
Descriptive statistics were used to calculate means and SDs or medians and range for continuous variables and numbers and percentages for categorical variables.
No meta-analysis was performed because most articles lacked homogeneous data, particularly the definition of HOA, patient inclusion and exclusion criteria, and standardised outcome assessments and tools for assessing overall HRQL.
The levels of evidence of our results are given as proposed by the Cochrane Collaboration group24: strong (consistent findings among multiple high quality randomised clinical trials); moderate (consistent findings among multiple low quality randomised clinical trials and/or controlled clinical trials and/or one high quality randomised clinical trial); limited (one low quality randomised clinical trial and/or controlled clinical trial); conflicting (inconsistent findings among multiple trials: randomised clinical trials and/or controlled clinical trials); no evidence from trials (no randomised clinical trials or controlled clinical trials).
Results
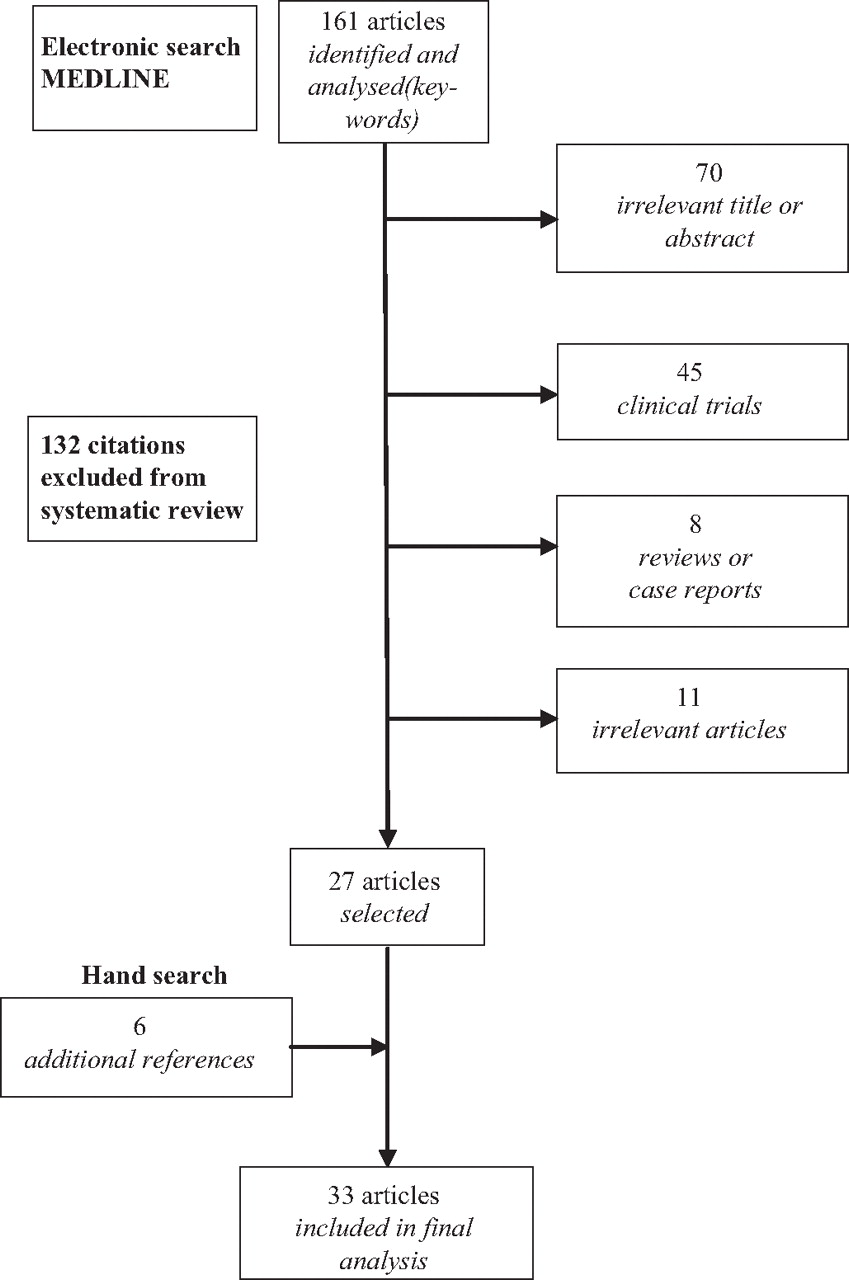
One hundred and sixty-one articles were identified and analysed, of which 134 were not included in the review. A hand search provided six additional relevant references, giving a total of 33 articles (figure 1).
{kind=link}
Flow chart of search strategy.
Demographic data are presented in table 1.
Demographic data
Outcomes
Three outcomes were usually used: pain (23 articles, 12 tools), function (30 articles, 23 tools) and stiffness (10 articles, 5 tools) (see table S1 in online supplement15 16 28 30 31 33 34 36 39 40 55 58–88). As several studies used the same cohorts, the summing up of the number of used tools takes into account each tool only once, and not the number of times each tool was used.
Three tools were developed specifically for HOA:
Two composite scores: AUSCAN (Australian Canadian osteoarthritis hand index) and SACRAH/M-SACRAH/SF-SACRAH (Score for Assessment and quantification of Chronic Rheumatic Affections of the Hand, its shortened modified version and its short form) are composed of three subscales: pain, function, stiffness and a global score. The initial SACRAH was developed to assess hands both in RA and HOA.
One strictly functional index: FIHOA (Functional Index for Hand Osteoarthritis).
One score, the Cochin index, was initially built for RA and subsequently validated in HOA.
Overall HRQL was rarely assessed and, when it was, a great number of heterogeneous tools were used including SF-36, AIMS2 (revised and expanded Arthritis Impact Measurement Scales), HAD (Hospital Anxiety and Depression scale) and global fatigue on a visual analogue scale (VAS) (see table S1 in online supplement).
Self-reported functional limitation in symptomatic HOA is reported in table S2 in the online supplement.
HOA versus RA
Three articles included symptomatic HOA and RA: Leeb et al (69 HOA, 103 RA), Goodson et al (10 HOA, 10 RA) and Slatkowsky-Christensen et al (190 HOA, 194 RA) (table 2).36 46 52
Hand osteoarthritis (HOA) versus rheumatoid arthritis (RA): outcomes assessment
Pain
There is moderate evidence that there is no difference in pain level between patients with RA and those with HOA. VAS,46 52 ‘pain’ subscale scores of SF-3652 and SACRAH36 were not statistically different between groups (p>0.05).
Function
There is conflicting evidence regarding the difference between patients with RA and those with HOA. The Cochin index46 and SACRAH ‘function’ subscale scores36 were not statistically different in the two sets of patients (p>0.05). M-HAQ,52 which is less specific for assessing hand problems, was less affected in HOA than in RA. Concerning hand strength, the available data are very heterogeneous. Hand strength can be measured in several ways: grip strength was assessed with a Jamar dynamometer (kg), an electronic dynamometer (Newtons) or in mm Hg. Pinch strength was measured with a Jamar hydraulic gauge (kg) or an electronic dynamometer (Newtons). Data were also collected differently: one or several measures (in the case of several successive measures, the highest or the mean value was used), both hands or one hand, and tripod pinch (thumb-index-middle finger) or thumb-index finger for pinch strength. Data in HOA are sparse and conflicting. Goodson et al found that grip strength was not statistically different in HOA and RA (p=0.19), except for the left hand (p<0.05); pinch strengths were comparable in HOA and RA (p>0.05)46 whereas data from a larger scale study suggested that grip strength could be higher in HOA than in RA.52
Stiffness
Evidence is limited. The ‘stiffness’ subscale of SACRAH36 was not statistically different between patients with HOA and RA (p>0.05). On the other hand, morning stiffness was longer in patients with RA.36
Overall HRQL
The evidence is also conflicting. Slatkowsky-Christensen et al52 demonstrated that HOA and RA patients had quite similar scores for all the assessed dimensions of subjective health. Nevertheless, patients with RA had poorer general health (SF-36) and greater fatigue than patients with HOA, whereas HOA patients reported poorer mental health. Another study36 found that the total score of SACRAH and patients' global assessment for HOA and RA patients were not statistically different.
Erosive and non-erosive HOA
One published study27 compared erosive and non-erosive HOA (10 erosive HOA (1 man/9 women), 14 non-erosive HOA (1 man/13 women), age 70 years (range 53–90) and 69 years (range 50–89), respectively; table 3). The demographic data were similar in the two groups, except for symptom duration. Neither group showed any statistical difference in grip strength, although dexterity was significantly impaired in erosive HOA (no numerical data in the original article). Other parameters of HRQL were not studied.27
Erosive and non-erosive hand osteoarthritis (HOA): outcomes assessment
We carried out a prospective cross-sectional study of successive outpatients presenting at the HOA Clinic of Saint-Antoine Hospital (101 patients (10 men, 90 women), mean (SD) age 63.8 (8.7) years with radiographic data available for 88 patients (38 erosive HOA, 50 non-erosive HOA), unpublished data). The demographic data were similar in the two groups. Inflammation and pain at rest in erosive HOA joints were no greater than in non-erosive HOA. However, patients with erosive HOA reported more aesthetic damage (scored by VAS) and functional impairment (higher FIHOA scores).54
Therefore, there is limited evidence that patients with erosive and non-erosive HOA are similar in terms of pain, stiffness and overall HRQL. One study reported that aesthetic damage seemed more important in patients with erosive HOA.
There is conflicting evidence regarding higher functional impairment in patients with erosive HOA than in those with non-erosive HOA.
Thumb base and interphalangeal OA
Three authors compared OA of the TB and IP: Dreiser et al (51 TB OA, 41 IP OA, gender and age by groups not detailed), Spacek et al (67 TB OA (6 men, 61 women), 49 IP OA (3 men, 46 women), mean (SD) age 62.71 (7.89) and 61.29 (6.55) years, respectively, similar demographic data) and Bijsterbosch et al (20 TB OA (5 men, 15 women), 138 IP OA (26 men, 112 women), mean (SD) age 59 (5.7) and 60.7 (7.6) years, respectively, similar demographic data) (table 4).28 38 56
TB OA and IP OA: outcomes assessment
There is moderate evidence that patients with TB OA and those with IP OA do not differ with respect to hand pain, function and overall HRQL. However, multivariate analysis in the study by Bijsterbosch et al (after adjustment for age, gender, BMI, family effects and number of symptomatic hand joints) showed significant differences in AUSCAN total scores of 7.4 (95% CI 1.8 to 13.0), suggesting a more severe impairment in TB OA than in IP OA; the same pattern was found for AUSCAN pain and function subscales scores.56 Thus, the evidence is conflicting.
Discussion
This review of published studies on HRQL in HOA neither compares nor recommends any of the tools presently used to assess HOA. It simply provides an overall picture of the way in which HRQL has been assessed in HOA. Few data on this important issue are presently available, and very little attention has been paid to aesthetic aspects although they are a major concern of patients with HOA.
HOA is a widespread disease, but remarkably little attention has been paid to its effect on HRQL. Its influence has clearly been underestimated and its global dimension, as described by the World Health Organization, is rarely assessed.8,–,10 OMERACT recommended pain, physical function and patient global assessment as the key outcomes in OA,11,–,13 and OARSI advised that HRQL should be measured in HOA.14 While pain, function and stiffness are usually well reported, it is still not clear how overall HRQL should be assessed, in part because of the many and varied tools that are used. The aesthetic aspect is never studied, although this is a major complaint in clinical practice. We still lack a specific tool with which to assess this issue.
Levels of evidence of our results are given as proposed by the Cochrane Collaboration group.24 As we voluntarily excluded randomised clinical trials from the systematic search, the levels of evidence cannot be strong but only moderate, limited or conflicting.
The assessment of the methodological quality of the studies as proposed by the Cochrane Collaboration method was not applicable to our articles. The methodological quality of cross-sectional and case–control studies could be assessed but, after discussion with several experts in the field, we were not able to find any standardised guidelines to assess the methodological quality of validation studies. As a report on quality based only on one part of the studies did not make sense, we decided not to include this assessment in the final text.
Three authors compared the clinical burdens of HOA and RA and found no difference between them in terms of pain. The available data on disability and stiffness are conflicting. Little is known about impairment of HRQL in patients with HOA and RA. Impairment seems to be similar in most dimensions of subjective health, according to the SF-36 health survey. Total SACRAH values in patients with HOA and RA were not statistically different, but this composite algo-functional score does not address overall HRQL.36 46 52 However, a selection bias must be taken into account in interpreting these results. Indeed, all patients were recruited from a rheumatology outpatient department and represented probably the worst cases of HOA. No population-based study has compared HOA and RA. The results could be different in population-based comparisons results; this has still to be investigated.
Two authors compared erosive and non-erosive HOA. No statistical difference was found in grip strength, although dexterity was significantly impaired in erosive HOA.27 Inflammation and pain at rest were similar in patients with erosive and non-erosive HOA, but more functional impairment was noted in erosive HOA. It is noteworthy that patients with erosive HOA reported more aesthetic damage since erosive HOA often leads to nodal deformations.54
More recently, a critical article by Bijsterbosch et al89 described the clinical burden of erosive HOA and its relationship to nodal HOA (presented at EULAR 2009). Compared with patients with non-erosive HOA, those with erosive HOA experienced more pain, more functional limitation, less satisfaction with hand function and aesthetics and worse hand mobility. HRQL was similar for the two groups. Patients with erosive HOA had more nodes, and a higher number of nodes was associated with a worse outcome. After correction for the number of nodes, only hand mobility and patient satisfaction remained different between the groups. These findings suggest that the higher burden in erosive HOA is not only due to the erosive disease itself, but mainly to the nodal character of the disease.
Three authors compared the clinical outcomes in TB OA and IP OA and found no differences in pain and function.28 38 56 However, multivariate analysis by Bijsterbosch et al suggested that TB involvement in symptomatic HOA is associated with more pain and functional disability, and with a higher AUSCAN total score.56 The definition of TB OA and IP OA is nevertheless confusing since some authors consider the most symptomatic site while others take isolated symptomatic sites only; this could lead to misunderstanding in interpreting the results. Again, it would be useful to compare aesthetic impairment in these two populations, but no such study has ever been done.
Dahaghin et al90 searched the literature for articles on the association of radiographic HOA with pain and functional impairment. Radiographic HOA and hand pain were positively linked, but evidence for a link between radiographic HOA and hand functional impairment was inconsistent. More severe radiographic HOA or an increasing number of hand joints with radiographic HOA seemed to be positively associated with more frequent or more severe pain.
Dziedzic et al91 reviewed how hand disability was assessed in HOA and rated the scores identified according to the OMERACT filter92 on the basis of their validity, discrimination and feasibility. The five instruments that performed well were: HAQ, AIMS1/2, FIHOA, the Cochin scale and AUSCAN.
Stamm et al93 reviewed questionnaires measuring function in patients with HOA using the International Classification of Functioning, Disability and Health (ICF).94 The ICF describes functioning as the complex interplay of the health components ‘body functions’, ‘body structures’, ‘activities and participation’ and ‘contextual factors, such as environmental and personal factors’. HAQ, AUSCAN, the Cochin scale, FIHOA, SACRAH and AIMS2-SF were analysed. AUSCAN and SACRAH had the lowest diversity ratio and AIMS2-SF the highest, as well as the greatest percentage of linked ICF categories. The authors suggested that one instrument with a low diversity ratio (for disease-specific aspects) and another instrument with a high diversity ratio (for broader aspects of functioning) should be included when selecting instruments for comprehensive measurements of functioning in HOA. In another study they also recommended using both a self-report instrument used generally in various cases of arthritis and a self-report instrument specific for HOA in order to comprehensively assess hand functioning in these patients.50
Ortiz et al95 reviewed the use of generic quality of life instruments in randomised controlled trials of rheumatic diseases with special emphasis on their responsiveness. Questionnaires were assessed for their truth, discrimination and feasibility within the context of the OMERACT filter.92 Most studies also included a disease-specific measure.
Carr96 emphasised the importance of measuring the wider personal and social consequences of OA on both populations and individual patients using disease-specific and generic measures of handicap. The World Health Organization definition of handicap94 was used to describe this wider impact of disease in patients with OA (not specifically HOA) and RA. Patients with OA reported handicap in six areas of their lives: functional and social activities, relationships, socioeconomic status, emotional well-being and body image. The prevalence was similar to that reported by patients with RA, but patients with OA reported more severe handicap than those with RA in each of the six areas and the differences were statistically different for all dimensions except functional and social handicap.
As often occurs in systematic reviews, we encountered several problems when comparing the results of different studies. One of the main problems was the different definitions of HOA, study population (gender, age), study design (population survey, clinical study, validation or evaluation of an instrument), outcome assessments and measuring instruments.
We may have missed some relevant articles because they used different keywords, had an unclear title or abstract or were not indexed in PubMed (Medline). However, our findings suggest that the impact of HOA may have been underestimated and highlight the importance of going beyond pain, function, stiffness and hand strength when assessing the clinical impact of HOA. The few available data that compare HOA and RA indicate that HOA has a high impact on HRQL. However, there are too few specific studies on HRQL in patients with HOA. Further studies should assess the true extent by which HRQL is reduced in HOA, which seems higher than anticipated or classically considered using standardised tools. Aesthetic damage, one of the major complaints of patients with HOA, remains unexplored. It certainly deserves more attention. We need a specific tool for exploring this issue in HOA.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Web Only Data
Files in this Data Supplement:
Footnotes
-
Provenance and peer review Not commissioned; externally peer reviewed