Article Text

Objectives
Patients can fulfil clinical criteria for remission, yet still have evidence of synovitis detectable clinically and by ultrasound, and this is associated with structural damage. Stricter remission criteria may more accurately reflect true remission (no synovitis). This hypothesis was examined by studying patients using more stringent thresholds for clinical remission and determining their levels of ultrasound synovitis.
Methods Rheumatoid arthritis patients with a disease activity score in 28 joints (DAS28) ≤2.6 for at least 6 months were classified using standard and more stringent DAS28 and simplified disease activity index (SDAI) remission thresholds and the corresponding clinical and ultrasound imaging measures of synovitis recorded.
Results 128 patients (all DAS28 <2.6, median DAS28 1.70) receiving either disease-modifying antirheumatic drugs alone (n=66) or with a tumour necrosis factor blocker (n=62) were recruited. Of the 640 imaged joints, 5% had moderate or severe power Doppler (PD) activity, 8% were clinically swollen and 1% tender. In patients fulfilling DAS28, American College of Rheumatology or SDAI remission criteria, moderate or severe PD activity was present in 21%, 15% and 19%, respectively. More stringent DAS28 and SDAI criteria reduced the mean number of swollen and tender joints (p<0.001) but not the percentage of patients with PD activity: 32 patients had a DAS28 <1.17 but eight (25%) had significant PD activity.
Conclusion Using more stringent remission criteria resulted in reduced signs and symptoms of inflammation, but the percentage of joints with PD activity was not reduced, even in those without signs or symptoms. These data suggest that clinical criteria are sufficiently insensitive to detect low but clinically relevant levels of inflammation accurately.
Statistics from Altmetric.com
The outcome for patients with rheumatoid arthritis (RA) is improving and clinical remission is now a realistic therapeutic goal.1 The American College of Rheumatology (ACR) criteria,2 disease activity score in 28 joints (DAS28)3,–,5 and the simplified disease activity index (SDAI)6,–,8 are used to define the remission state. Both DAS28 and SDAI correlate with the opinions of rheumatologists as to what constitutes remission, with receiver operator curves of moe than 0.94.
It has recently been shown that the majority of patients in disease-modifying antirheumatic drug (DMARD) or combination tumour necrosis factor (TNF) blocker and methotrexate-induced clinical remission (according to DAS28 or ACR criteria) continue to have synovitis detectable by imaging.9 10 There is evidence that ultrasound is more sensitive than clinical examination for detecting synovitis.11 12 Ultrasound assessment of synovitis includes grey scale (GS; a measure of synovial thickness or hypertrophy) and power Doppler (PD; a measure of synovial vascularity, which may better reflect active inflammation). Furthermore PD activity has been shown to be the best predictor of subsequent joint damage in the affected joint in DMARD-treated patients in remission with an odds ratio of 12.21.13 As multivariate analyses were not included an independent predictive value was not definitively established. The failure of clinical examination to correlate with PD activity and grey scale synovial hypertrophy (GSSH) may be due to the fact that clinical scores are not stringent enough, ie, a patient may fulfil the current definitions of remission yet have clinical evidence of ongoing disease activity, for example, tender or swollen joints.14 It may therefore be expected that more stringent criteria (ie, the use of lower cut-points for DAS28/SDAI to define remission) would be associated with less PD activity and GSSH (imaging-detected synovitis). This would, for example, permit fewer (ideally zero) tender and swollen joints to be present in patients in remission and thus there would be a better correlation with the absence of structural progression. Alternatively it may be that clinical and biochemical assessments are insufficiently sensitive in low disease activity states, if so fulfilling more stringent criteria may not guarantee the absence of synovitis. As the relationship between clinical measures of remission and objective imaging synovitis is poorly described, either of these two explanations were possible. This study aimed to answer this question by assessing the accuracy of more stringent remission criteria for indicating the absence of inflammation, using ultrasound imaging assessment of synovitis as the gold standard.
Patients and methods
Patients
Consecutive patients with RA in clinical remission (DAS28 <2.6) were recruited in this cohort study, from the rheumatology outpatient clinic at Chapel Allerton Hospital, Leeds, UK. Patients were treated with either DMARD (n=66) or combination TNF blocker and methotrexate (n=62). Data are generated from the Leeds remission cohort, and data from the 66 DMARD and 50 TNF blocker-treated patients were included in Brown and colleagues9 13 and Saleem et al.10 Ethics approval was obtained from the Leeds Teaching Hospital Trust and written informed consent was obtained from all patients.
Inclusion criteria
Patients had to fulfil the following criteria: (1) RA classified according to ACR criteria; (2) age greater than 18 years; (3) clinical remission (DAS28 <2.6); (4) no flares of disease in past 6 months; (5) stable treatment for 6 months; and (6) no indication for a change in treatment.
Clinical and imaging assessments
Standard clinical assessments of disease activity, function and quality of life were performed. The dominant hand metacarpophalangeal joints 2–5 and wrist were scanned, imaging both the dorsal and palmer surfaces. Individual joints were scored for GSSH and PD using a validated semiquantitative method (0–3),12 15 ie, GSSH, 0: no synovial hypertrophy; 1: mild; 2: moderate; 3: severe; PD, 0: normal/minimal vascularity; 1: mild hyperaemia; 2: moderate; and 3: marked. The ultrasound scores were expressed per joint and as a total score (when scores in all joints in each patient were added together to produce a total score). See supplementary material available online only.
Definitions of clinical remission
All patients were required to fulfil DAS28 remission criteria.3 16 17 Other assessments of remission included in this study were the modified ACR remission criteria2 and the SDAI criteria for remission.6 18 ACR and EULAR propose that a patient be defined as in remission based on one of two definitions of remission: when their scores on the following measures are all 1 or less: tender joint count (TJC), swollen joint count (SJC), C-reactive protein (CRP; in mg/dl) and patient global assessment (0–10 scale), or when their score on the SDAI is 3.3 or less.19 All of these measures of remission were evaluated in this study.
In addition the patients were grouped into strict DAS28 and SDAI subcategories determined by the quartiles of the distribution of scores. Patients were also divided according to the presence or absence of objective clinical measures of inflammation, ie, swollen or tender joints and raised CRP.
Definitions of imaging remission
Several different indicators of imaging remission were examined: strict imaging remission was defined as the absence of both GSSH and PD activity in dominant hand metacarpophalangeal joints 2–5 and wrist (all GS=0 and PD=0). A less strict criterion was used to indicate low level imaging activity (all GS≤1 and PD≤1). In addition, remission criteria based solely on PD (absent (PD=0) or low level (PD≤1)) were included.
Statistics
The SPSS 17.0.2 software package was used for the analysis. Normally distributed continuous data were summarised with means and SD. Non-normally distributed continuous and ordinal data were summarised with medians and first and third quartiles, and were compared between groups using Mann–Whitney U tests and Jonckheere–Terpstra tests. Categorical data were summarised using absolute and relative frequencies, and were analysed using χ2 tests (Pearson's χ2 and linear by linear association). See supplementary material available online only for additional statistical information.
Results
Baseline characteristics
One hundred and twenty-eight RA patients in DAS28 remission were recruited. The mean age was 54 years (SD 14) and median disease duration was 8 years (1st to 3rd quartile 5–13). All patients had been in remission for at least 6 months (median 16 months (12–24)). Sixty-six patients had been treated with DMARD: 73% monotherapy, 15% dual combination therapy and 8% triple combination therapy. Sixty-two patients had been treated with combination TNF blocker and methotrexate (45% infliximab, 45% etanercept, 10% adalimumab). Ten per cent of patients were on low-dose prednisolone (median dose 5 mg per day) and 31% of patients were taking regular non-steroidal anti-inflammatory drugs (NSAID).
Clinical examination and imaging findings
Clinical scores of disease activity and imaging-detected synovitis
Disease activity score DAS28
Forty patients (31%) had swollen joints, 23 (18%) had tender joints and 46 (36%) had a detectable CRP (≥5 mg/dl). The median swollen and tender joint counts and CRP were all zero (1st to 3rd quartile SJC: 0–1; TJC: 0–0; CRP: 0–5.15). Sixty-five (51%) patients in DAS28 remission had detectable PD in at least one joint and in 27 (21%) this was moderate or severe (PD >1; all the patients with PD signal had GSSH). All further reference to PD activity assumes GSSH was also present. The median total GS score per patient was 3 (1–7) and the median total PD activity score per patient was 1 (0–2).
ACR remission criteria (modified)
Ninety-six patients (75%) in DAS28 remission also fulfilled the modified ACR remission criteria (table 1). Twenty patients (21%) in ACR remission had swollen joints and five patients had tender joints (5%). Patients fulfilling ACR remission criteria had fewer swollen and tender joints than those that did not (swollen joints: 0 vs 1; p<0.001, tender joints: 0 vs 1; p<0.001). Fulfilling ACR criteria for remission slightly increased the proportion of patients in strictly defined imaging remission compared with not fulfilling ACR criteria (18.8% vs 12.5%, p=0.417 for GS=0 and PD=0; 52.1% vs 40.6%, p=0.262 when PD=0 alone used as a criterion); this difference was larger when the less strict criterion of ‘low level activity’ was used (61.5% vs 40.6%, p=0.040 for GS ≤1 and PD ≤1; 84.4% vs 62.5%, p=0.009 for PD ≤1). Comparing patients in ACR remission with those not in ACR remission, there was no difference the proportion of joints scoring PD=1, PD=2 or PD=3. The sensitivity of ACR remission for PD=0 was 79% (95% CI 67% to 88%) with a specificity of 29% (19% to 42%); the sensitivity for PD ≤1 was 80% (71% to 87%) with a specificity of 44% (26% to 64%).
The relationship between clinical scores of remission, imaging detected synovitis and quality of life outcomes
Simplified disease activity index
Seventy-four patients (58%) in DAS28 remission met criteria for SDAI remission (table 1). Ten patients in SDAI remission (14%) had swollen joints and three patients (4%) had tender joints. Similar to ACR remission criteria, patients fulfilling SDAI remission criteria had fewer swollen and tender joints (median swollen: 0 vs 1 (p<0.001); median tender: 0 versus 0 (p<0.001)) but there was no difference in CRP. A greater proportion of patients in SDAI remission were in strict imaging remission when compared with patients not in SDAI remission (23.0% vs 9.3%, p=0.042 for GS=0 and PD=0; 54.1% vs 42.6%, p=0.200 for PD=0). Smaller trends were seen for low-level imaging activity. Comparing patients in SDAI remission with those not in SDAI remission, there was no difference in the proportion of joints scoring PD=1, PD=2 or PD=3. The sensitivity of SDAI remission criteria for PD=0 was 63% (50% to 75%) and the specificity was 48% (35% to 60%); for PD ≤1 sensitivity was 59% (49% to 70%) and specificity was 48% (29% to 68%).
The 2010 ACR/EULAR remission criteria
Twenty-nine of the patients (23%) met these criteria (table 1). The proportions of patients fulfilling the various imaging remission criteria were similar across the two groups.
More stringent remission scores and imaging-detected synovitis
Disease activity remission subcategories (DAS28)
Patients were divided into four subcategories (as explained in the Methods section: DAS28 <1.17, 1.17–1.70, 1.71–2.03, >2.03). As was to be expected, both SJC28 (p<0.001) and TJC28 (p<0.001) decreased with decreasing DAS28 (table 2). Importantly, more stringent DAS28 cut-points were not associated with a reduction in the amount or median score for either PD activity or GSSH (see figure 1). The proportions of patients in imaging remission did not increase consistently with decreasing DAS28 category; 9% of patients in the lowest category were in strictly defined remission (GS=0 and PD=0),. No clear trends were observed when looking at the proportion of joints with PD=1, PD=2 or PD=3 among the patients in each DAS28 category.

The relationship between stringent disease activity score in 28 joints (DAS28) subcategories of remission and total median power Doppler (PD) activity and total median grey scale (GS) synovial hypertrophy score per patients as detected by ultrasound. No significant difference was seen between the groups.
The relationship between stringent measures of remission, imaging-detected synovitis and function and quality of life outcomes
Disease activity remission subcategories (SDAI)
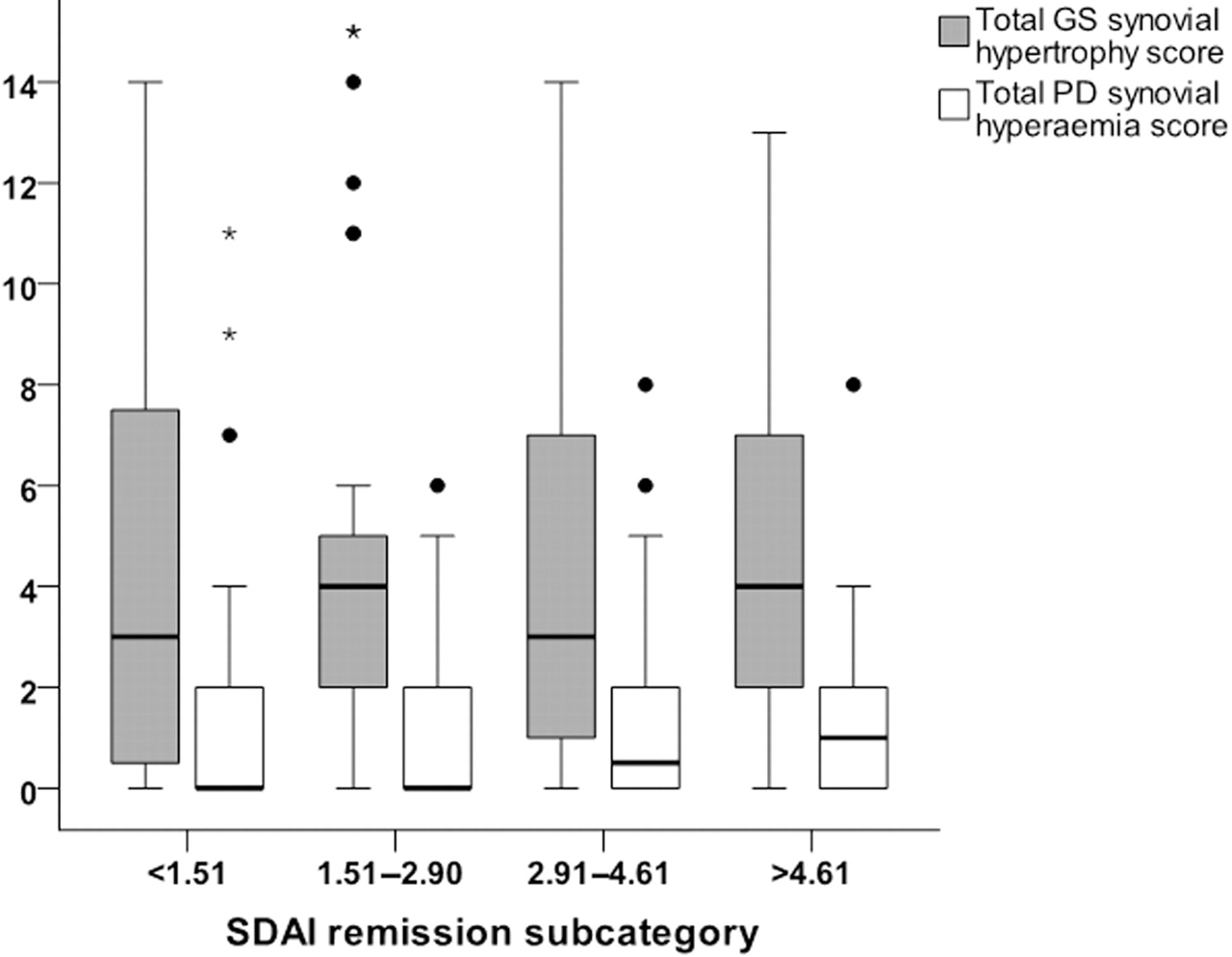
The patients were divided into SDAI remission subcategories (SDAI <1.51, 1.51–2.90, 2.91–4.61, >4.61). Both SJC28 (p<0.001) and TJC28 (p<0.001) decreased with decreasing SDAI (table 2). Lower remission SDAI thresholds were not associated with a decrease in the amount or median score for either PD activity or GSSH (see figure 2). Twenty-five per cent of patients in the lowest SDAI category were in strictly defined imaging remission.

{kind=link}
{kind=link}
The relationship between stringent simplified disease activity index (SDAI) subcategories of remission and total median power Doppler (PD) activity and total median grey scale (GS) synovial hypertrophy score per patients as detected by ultrasound. No significant difference was seen between the groups.
Clinical measures of disease activity and imaging-detected synovitis
Swollen joints
Eighty-eight patients (69%) in DAS28 remission had no swollen joints (SJC28=0). Patients with SJC28 >0 had higher GS scores (4.5 vs 3.0; p=0.052) and PD scores (1 vs 0; p=0.010) (table 3). SJC28 >0 was associated with the presence of a high individual joint PD score on ultrasound; a maximum PD score of 2 or above was seen in 30% of patients with at least one swollen joint compared with 17.5% of patients with no swollen joints (p=0.020).
The relationship between clinical measures of remission, imaging detected synovitis and function and quality of life outcomes
The sensitivity of a swollen joint for PD >0 was 13.1% (7.5% to 21.8%) with a specificity of 92.8% (90.1% to 94.8%); for PD ≤1 sensitivity was 20.0% (1.1% to 70.1%) and specificity was 92.0% (90.0% to 93.9%).
Tender joints
One hundred and five patients (82%) in DAS28 remission had no tender joints (TJC28=0).
The absence or presence of tender joints was not associated with differences in median total GS or PD scores. Similar proportions of patients with and without tender joints were in imaging remission according to the various criteria.
The sensitivity of a tender joint for PD >0 was 2.0% (0.4% to 7.8%) with a specificity of 99.3% (98.0% to 99.8%); for PD ≤1 sensitivity was 0.0% (0.0% to 53.7%) and specificity was 99.1% (97.8% to 99.6%).
C-reactive protein
Eighty-two patients (64%) had a normal CRP (table 3). Fewer patients with CRP=0 were in imaging remission (GS=0 and PD=0: 13% vs 24%, p=0.131) and fewer had only low-level joint activity (GS ≤1 and PD ≤1: 48% vs 72%, p=0.008). The sensitivity of a normal CRP for PD=0 was 58.7% (45.6% to 70.8%) with a specificity of 32.8% (22.1% to 45.5%); for PD ≤1 sensitivity was 59.4% (49.1% to 68.9%) and specificity was 24.1% (11.0% to 43.9%).
Agreement between clinical assessment and ultrasound findings in individual joints
See supplementary material available online only.
Comparison of treatment groups
See supplementary material available online only.
Discussion
Recent evidence has demonstrated that most RA patients in drug-induced (DMARD or biological agent) remission continue to have synovitis, detectable using ultrasound9 10 and that in DMARD-treated patients PD activity is predictive of subsequent radiographic deterioration.13 This suggests that current criteria may lack the necessary sensitivity for accurate remission assessment. Using patients in DAS28 remission from this previously published cohort of patients in remission, this study assessed the level of imaging inflammation in a cohort of patients treated with either DMARD or combination TNF blocker according to commonly used clinical remission scores. It demonstrated that the majority of patients in remission had at least mild PD activity, hence active inflammation, regardless of the composite remission criteria applied, and that approximately 20–30% had moderate or severe PD activity in at least one joint. Furthermore, when more stringent remission criteria were used, adopting tighter disease activity thresholds, there was no substantive improvement in the rates of imaging remission.
The DAS28 is widely used in clinical practice, is relatively easy to calculate (portable and web-based calculators are widely available) and DAS28 <2.6 is recommended by EULAR and ACR as a measure of remission.20 However, a DAS28 <2.6 may allow the presence of tender and/or swollen joints or raised levels of acute phase response, thus may not be a true measure of the absence of inflammation. The ACR remission criterion is a dichotomous score and is considered by some as too rigorous, although in the present study only a minority of those in ACR remission were also in strictly defined imaging remission (PD=0 and GS=0). The SDAI is considered a more stringent measure of remission as it allows for the least abnormalities of variables.21 In this study fewer patients fulfilling SDAI remission criteria had swollen joints (14%) compared with patients fulfilling DAS28 remission criteria (31%); however, mild PD activity was still present in approximately 45% and approximately 19% had moderate or severe PD activity (cf. 21% in DAS28 remission). However, more patients in SDAI remission were in imaging remission (PD=0 and GS=0) when compared with patients not in SDAI remission.
This study also aimed to determine whether the use of stricter criteria would be associated with a reduction in ultrasound-detected inflammation, ie, PD activity. The aim was to clarify whether clinical examination is accurate in patients with low levels of inflammation. However, even the use of more stringent criteria (which inevitably were associated with a reduced number of swollen and tender joints) was still associated with significant imaging-detected inflammation. This level of inflammation has previously been shown to predict subsequent structural deterioration in DMARD-treated patients in remission.15 Of particular interest, when a less stringent definition of imaging remission was used (GS ≤1 and PD ≤1), more patients fulfilled imaging remission criteria but the percentages differed to a substantive degree only for ACR remission (61.5%) versus non ACR-remission (40.6%); for SDAI remission (59.5% vs 51.9%) and the newer ACR/EULAR criteria (51.7% vs 57.6%) there was only a very small difference between groups. Furthermore, lowering the DAS28 threshold did not increase the proportion of patients in imaging remission. The relevance of this is unclear, especially as the threshold level of ultrasound-determined inflammation that is of importance for subsequent clinical and radiographic progression has not yet been established. The results show that despite clinically and biochemically normal findings, imaging-detected inflammation continues. Therefore current clinical remission criteria (that are partly based on clinically detected tender and swollen joints) are insufficiently sensitive to exclude (clinically important) levels of inflammation. Therefore, as clinical criteria cannot exclude the presence of active disease, the current remission criteria are more appropriate for defining low disease activity states.
The use of the term remission in other areas of medicine implies the absence of active disease. The rheumatological equivalent of this true remission would therefore not rely solely on clinical examination but would require imaging to confirm the absence of subclinical inflammation.
A potential limitation of this study is the number of joints assessed by ultrasound. There is published evidence that a reduced ultrasound joint assessment is good enough for assessing overall inflammatory activity.22 However, the ideal joint count in patients in remission, with none or minimal tender and swollen joints, is unknown. Another potential limitation could be that two rheumatologists performed the scans (see supplementary material available online only for intraobserver reliability). Furthermore, in patients treated with DMARD in clinical remission ultrasound scanning of the wrist and metacarpophalangeal joints of the dominant hand was sufficient to predict further structural damage. Also by masking clinical symptoms and signs, corticosteroids and NSAID could potentially alter the relationship between symptoms, signs and the level of synovitis. However, in the study only a minority of patients were taking corticosteroids and although 30% were on regular NSAID there was no significant difference between the number of swollen (p=0.4) or tender joints (p=0.1) and NSAID usage.
In conclusion, fulfilling standard and new remission criteria (DAS28, ACR, SDAI, 2010 ACR/EULAR) did not indicate the absence of subclinical inflammation, as measured by PD, nor was this lack of sensitivity improved by using more stringent thresholds for DAS28 or SDAI. As is clear from this study, this is the consequence of the inability of clinical examination to detect low, but (as previously shown) clinically important levels of inflammation objectively demonstrated by imaging.
This study provides additional evidence to support the use of imaging to ensure accurate disease activity assessment in patients with low disease activity state/remission.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Leeds Teaching Hospital Trust.
-
Provenance and peer review Not commissioned; externally peer reviewed.