Article Text

Abstract
Background Systemic sclerosis (SSc) features autoimmunity, vasculopathy and tissue fibrosis. The renin-angiotensin and endothelin systems have been implicated in vasculopathy and fibrosis. A role for autoantibody-mediated receptor stimulation is hypothesised, linking three major pathophysiological features consistent with SSc.
Methods Serum samples from 478 patients with SSc (298 in the study cohort and 180 from two further independent cohorts), 372 healthy subjects and 311 control-disease subjects were tested for antibodies against angiotensin II type 1 receptor (AT1R) and endothelin-1 type A receptor (ETAR) by solid phase assay. Binding specificities were tested by immunoprecipitation. The biological effects of autoantibodies in microvascular endothelial cells in vitro were also determined, as well as the quantitative differences in autoantibody levels on specific organ involvements and their predictive value for SSc-related mortality.
Results Anti-AT1R and anti-ETAR autoantibodies were detected in most patients with SSc. Autoantibodies specifically bound to respective receptors on endothelial cells. Higher levels of both autoantibodies were associated with more severe disease manifestations and predicted SSc-related mortality. Both autoantibodies exert biological effects as they induced extracellular signal-regulated kinase 1/2 phosphorylation and increased transforming growth factor β gene expression in endothelial cells which could be blocked with specific receptor antagonists.
Conclusions Functional autoimmunity directed at AT1R and ETAR is common in patients with SSc. AT1R and ETAR autoantibodies could contribute to disease pathogenesis and may serve as biomarkers for risk assessment of disease progression.
Statistics from Altmetric.com
Systemic sclerosis (SSc) is an incurable heterogeneous multiorgan disease of unknown origin.1 Despite improvements achieved during the last decade, diffuse SSc has the highest mortality of all connective tissue diseases.2 A triad of vasculopathy, autoimmunity and fibrosis is a distinctive feature. According to the 30-year-old ‘vascular hypothesis’, vascular dysfunction leads to skin and visceral organ sclerosis.3 Patient survival and quality of life are often determined by vascular complications.4 ACE inhibitors reduce mortality from renal crisis.4 Endothelin-1 (ET-1) receptor blockers may improve the outcomes of patients with pulmonary arterial hypertension, the most important cause of death beside pulmonary interstitial involvement.5 6 Angiotensin II type 1 receptor (AT1R) blockers and ET-1 receptor blockers seem to alleviate some vascular manifestations of SSc beyond inducing vasodilation.7 8 The utility of these strategies and the increased levels of angiotensin II (Ang II) and ET-1 in SSc could implicate Ang II and ET-1 in the pathogenesis of SSc.9 10 Detrimental vasoconstrictor, proinflammatory, proproliferative and profibrotic effects of Ang II and ET-1 relevant to SSc pathophysiology are mediated by the functionally pleiotropic AT1R and endothelin-1 type A receptors (ETARs).11 12 Autoimmune agonistic antibody-mediated AT1R stimulation has been demonstrated in severe vasculopathies associated with allograft rejection and pre-eclampsia.13 14 The obliterative vascular lesions in these conditions resemble those in SSc. Many biological processes mediated by AT1R antibodies, such as increased oxidative stress and induction of antiangiogenic mediators, appear to be important in the pathophysiology of SSc.15 We reasoned that autoantibody-mediated vascular receptor activation could contribute to the pathophysiology of SSc and might serve as a diagnostic biomarker for detection of severe disease manifestations.
Methods
Patients and clinical manifestations
Serum samples from 298 consecutive patients with SSc referred to the Department of Rheumatology and Clinical Immunology, Charité University Hospital were collected between January 2004 and November 2008. In addition, 137 patients from the Department of Immunology and Rheumatology, University of Pecs and 43 patients from the Department of Rheumatology, University of Florence were studied as SSc independent cohorts. All patients with SSc were classified as having either limited SSc or diffuse SSc according to the LeRoy criteria, depending on the distribution of skin sclerosis before the initiation of the study.16 The first non-Raynaud symptom was considered as disease onset. Procedures standardised by the European Scleroderma Trials and Research (EUSTAR) group were used for clinical assessment.17 Patients with overlap syndromes including mixed connective tissue disease were included in the German cohort. Control serum samples were obtained from 372 healthy subjects and 311 control disease patients, including 208 patients with rheumatoid arthritis, 33 with morphea (localised scleroderma), 32 with primary Raynaud's phenomenon and 38 patients with primary Sjögren's syndrome (pSS). The diagnosis in each control group was made according to established criteria.18,–,22 Primary Raynaud's phenomenon was defined by the presence of this phenomenon with negative antinuclear antibody and capillaroscopy.
Solid-phase assay
A sandwich ELISA (CellTrend GmbH, Luckenwalde, Germany) was developed to measure anti-AT1R and anti-ETAR autoantibodies. The microtitre 96-well polystyrene plates were coated with extracts from Chinese hamster ovary cells overexpressing the human AT1R or the human ETAR, respectively. To maintain the conformational epitopes of both receptors, 1 mM calcium chloride was added to each buffer. Duplicate samples of a 1:100 serum dilution were incubated at 4°C for 2 h. After washing steps, plates were incubated for 60 min with a 1:20 000 dilution of horseradish peroxidase-labelled goat anti-human IgG (Jackson, West Grove, Pennsylvania, USA) used for detection. In order to obtain a standard curve, plates were incubated with test serum samples from an anti-AT1R autoantibody-positive or anti-ETAR autoantibody-positive index patient. The ELISA was validated according to the Food and Drug Administration's ‘Guidance for Industry: Bioanalytical Method Validation’. The interassay variability was 7% and the intra-assay variability was 6%. Persons who were unaware of the patients' characteristics performed the assays.
Binding specificity and functional studies
All experiments were conducted with IgG isolated from patient serum samples as previously described.13 The beads-antibodies complexes consisting of protein G agarose beads and either patient IgG or healthy donor IgG were incubated overnight with lysates derived from human dermal microvascular endothelial cells (HMECs). The immunoprecipitates were separated by 8–10% sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE) under reducing conditions, electroblotted on nitrocellulose membranes and probed with either anti-AT1R antibodies (LifeSpan Biosciences, Seattle, Washington, USA) or anti-ETAR antibodies (Abcam, Cambridge, Massachusetts, USA). Blots were visualised by an enhanced chemiluminescence system. For signal transduction and gene expression studies, HMECs were stimulated with Ang II, ET-1, patient IgG or control IgG in the presence or absence of AT1R blocker (valsartan), AT2R blocker (PD123319), ETAR blocker (BQ-123) or ETBR blocker (BQ-788). Protein extraction, SDS-PAGE and membrane treatment were performed as described previously.13 Membranes were probed with a phospho-extracellular signal-regulated kinase (ERK) 1/2 antibody (Cell Signaling, Danvers, Massachusetts, USA). Whole cell mRNA extracted with the RNAeasy kit (Qiagen, Hilden, Germany) according to the manufacturer's protocol was reverse-transcribed and analysed by the MxPro Mx3005P QPCR Systems (Agilent, Santa Clara, California, USA). Primers were designed using Primer3 software and provided by TIB Molbiol (Berlin, Germany) with the sequences: transforming growth factor β1 (TGFβ1) forward 5′-GCA-ACA-ATT-CCT-GGC-GAT-AC-3′ and reverse 5′-GAA-CCC-GTT-GAT-GTG-CAC-TT-3′; EEF1A1 forward 5′-GTT-GAT-ATG-GTT-CCT-GGC-AAG-C-3′ and reverse 5′-GCC-AGC-TCC-AGC-AGC-CTT-C-3′.
Triplicate experiments with 4–10 different patient IgG preparations were performed in all functional studies.
Statistics
Receiver operating characteristic (ROC) curves were plotted for the sensitivity of the AT1R and ETAR antibody detection tests against 1 minus the specificity for all control diseases studied and the respective cut-off values were determined. Continuous data are presented as means or medians as indicated. Comparisons between groups were performed with the Mann–Whitney U test for continuous variables. The χ2 test was used to identify an association between SSc symptoms and the presence of the antireceptor antibodies. RRs were calculated to determine associations with individual organ involvements, assessed according to EUSTAR criteria for individual clinical assessment.17 Kaplan–Meier analysis for SSc-related mortality based on the determined cut-off values was performed in a prospective follow-up study of 186 patients during the mean observation period of 48 months after detection of antibodies.
Results
Diagnostic value of anti-AT1R and anti-ETAR autoantibodies in SSc
Demographic data, clinical manifestations, disease duration and serology for all cohorts studied are shown in table 1. Of the 298 patients with SSc from Charité University Hospital, 175 had limited SSc and 123 had diffuse SSc. Patients with SSc had higher levels of both anti-AT1R and anti-ETAR autoanti- bodies compared with all control groups (figure 1A,B and table 1). Anti-AT1R and anti-ETAR antibody levels (p=0.001) were also higher in patients with rheumatoid arthritis and those with pSS than in healthy subjects. ROC curve analysis set an optimal cut-off at 9.23 units for the detection of anti-AT1R antibodies had 85.1% sensitivity and 77.9% specificity for the diagnosis of SSc compared with healthy subjects (figure 1C). An optimal cut-off set at 10.4 units for the detection of anti-ETAR antibodies had 83.7% sensitivity and 77% specificity for the diagnosis of SSc (figure 1D). Patients with SSc were older than the control groups. Thus, separate analysis in age-matched SSc and control cohorts were conducted (see table 1 in online supplement). Again, levels of both antibodies were higher in patients with SSc than in sex- and age-matched control groups. ROC curve analysis revealed similar results providing an optimal cut-off at 9.5 units for the detection of anti-AT1R antibodies with 83% sensitivity and 67% specificity for the diagnosis of SSc compared with healthy subjects. An optimal cut-off set at 10.4 units for the detection of anti-ETAR antibodies had 82% sensitivity and 75% specificity for the diagnosis of SSc. Thus, data in age- and sex-matched cohorts were almost identical to analysis in unmatched cohorts.

Diagnostic value of anti-AT1R and anti-ETAR autoantibodies in systemic sclerosis (SSc). (A) Anti-AT1R and (B) anti-ETAR autoantibodies serum levels in healthy subjects (N), patients with rheumatoid arthritis (RA), SSc, primary Sjögren syndrome (pSS), morphea (M) and primary Raynaud's phenomenon (PRP). Mean levels are shown as lines; p<0.001 when levels in SSc patients were compared with healthy subjects or patients with each of the control diseases. Receiver operating characteristic analyses for anti-AT1R and anti-ETAR autoantibodies compared with healthy controls in (C) non-matched and (D) sex- and age-matched cohorts. AT1R, angiotensin II type 1 receptor; ETAR, endothelin-1 type A receptor.
Demographic characteristics of the patients with systemic sclerosis (SSc) and control patients with rheumatoid arthritis (RA), primary Raynaud's phenomenon (PRP), morphea as well as healthy subjects and anti-AT1R and anti-ETAR antibody levels for each group studied
Comparison of autoantibody values obtained in patients from our centre with two independent SSc cohorts from two different European regions and EUSTAR centres (Hungary and Italy) showed similar values (see figure and table 2 in online supplement).
Coincident occurrence and binding specificities of anti-AT1R and anti-ETAR autoantibodies
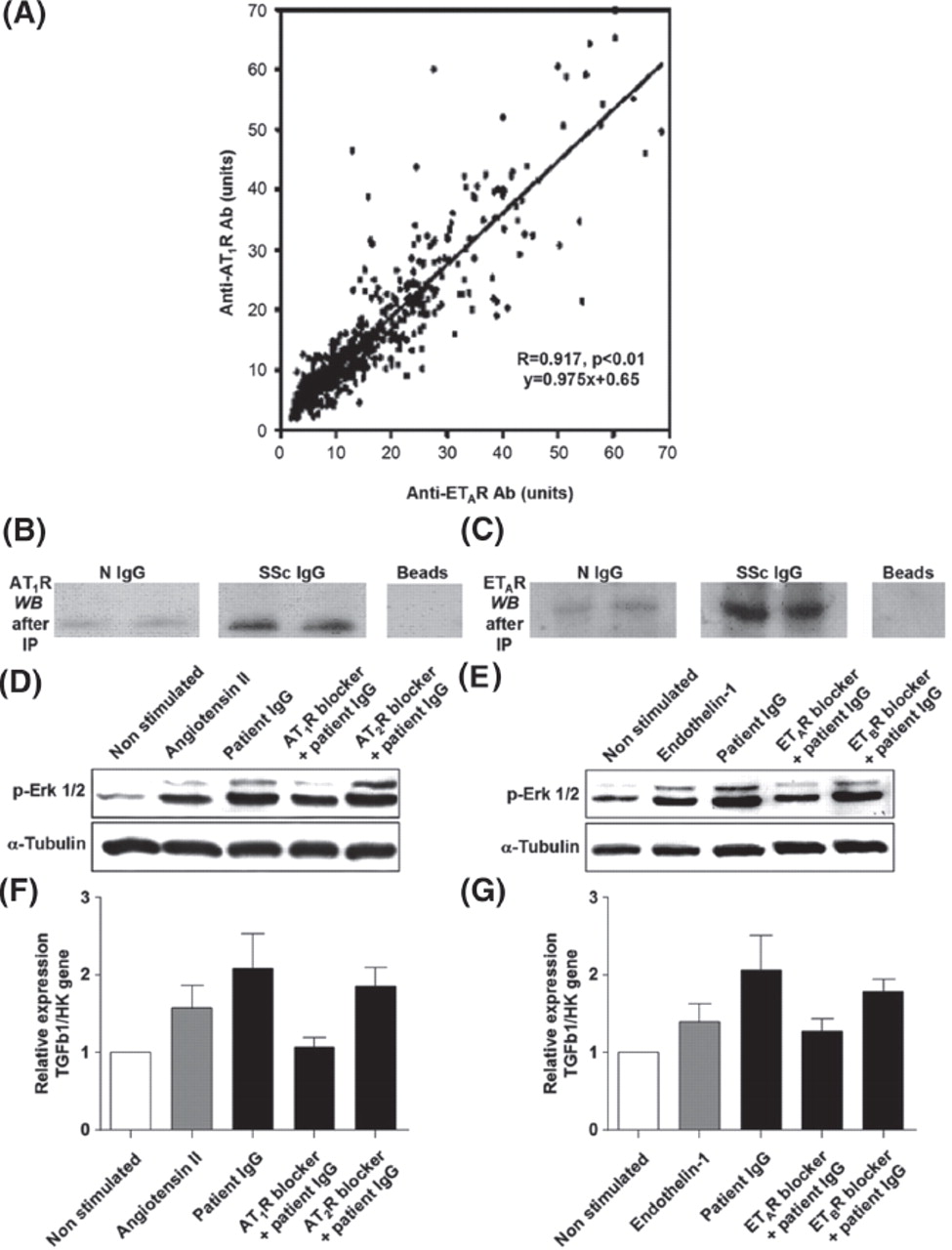
A strong correlation between anti-AT1R and anti-ETAR autoantibodies was present in patients with SSc (R=0.917, p≤0.01, figure 2A). We found only a very weak association between patient age and respective autoantibody levels (R=0.172, p=0.003 for anti-ETAR autoantibody and R=0.142, p=0.014 for anti-AT1R autoantibody) not present in controls and age-matched patients with SSc. We also observed a weak correlation between duration of SSc and anti-AT1R autoantibody levels (R=0.191, p=0.001) or anti-ETAR autoantibody levels (R=0.214, p<0.001), respectively.
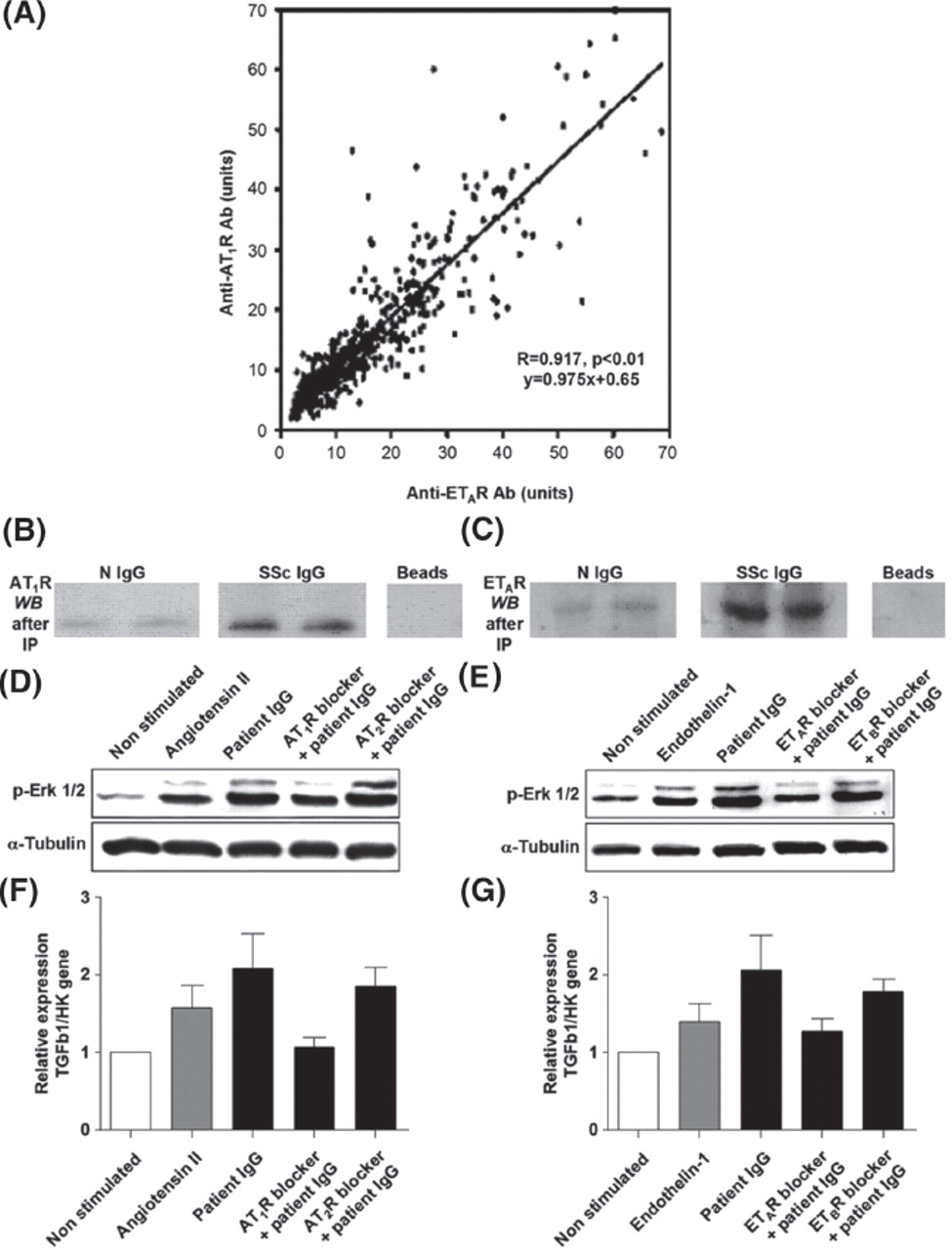
Coincident occurrence, binding specificities of anti-AT1R and anti-ETAR autoantibodies and their biological effects in human microvascular endothelial cells. (A) A strong correlation between anti-AT1R and anti-ETAR autoantibodies is found (R=0.917, p<0.01, slope=0.975). Immunoprecipitates of human dermal microvascular endothelial cell lysates with IgG purified from patients with systemic sclerosis (SSc IgG) but not from healthy controls (N IgG) can be specifically detected by immunoblotting with (B) commercially available AT1R antibodies and (C) ETAR antibodies after immunoprecipitation. Beads indicate negative control. Anti-AT1R autoantibodies (D) stimulate phosphorylation of ERK1/2 (p-ERK) and (F) increase TGFβ transcripts similar to natural ligand in microvascular endothelial cells, which can be blocked by AT1R-blocker, but not by AT2R-blocker. Anti-ETAR autoantibodies (E) stimulate phosphorylation of ERK1/2 (p-ERK) in microvascular endothelial cells and (G) increase TGFβ transcripts similar to natural ligand which can be blocked by ETAR-blocker, but not by ETBR-blocker. AT1R, angiotensin II type 1 receptor; ETAR, endothelin-1 type A receptor; ERK, extracellular signal-regulated kinase; TGFβ1, transforming growth factor β1.
The interaction and binding specificity of both anti-AT1R and anti-ETAR autoantibodies with the native human AT1R and ETAR expressed in endothelial cells was assessed in immunoprecipitation experiments. IgG from patients with SSc tested positive for anti-AT1R and anti-ETAR autoantibodies in solid phase assay precipitated both AT1R and ETAR while, in contrast, IgG from autoantibody-negative healthy subjects failed to immunoprecipitate both AT1R and ETAR (figure 2B,C).
Biological effects of anti-AT1R and anti-ETAR autoantibodies in human microvascular endothelial cells
We also examined whether anti-AT1R autoantibodies and anti-ETAR autoantibodies could initiate canonic signalling mediated by ERK1/2 in vitro by means of microvascular endothelial cells. Natural ligands and both autoantibodies induced phosphorylation of ERK1/2, which peaked at 10 min (figure 2D,E). Specificity was confirmed by AT1R and/or ETAR blockade and lack of effect of AT2R and/or ETBR pharmacological antagonists. Stimulation with anti-AT1R autoantibodies increased gene expression of profibrotic cytokine TGFβ similar to Ang II (figure 2F), which was blocked by the AT1R blocker valsartan. Anti-ETAR autoantibodies induced in vitro a stronger expression of TGFβ transcripts than ET-1 (figure 2G). Specificity was again confirmed by ETAR blockade and lack of effect of ETBR blockade.
Anti-AT1R and anti-ETAR autoantibody levels and SSc-related manifestations
We identified quantitative differences in cut-offs for levels of both anti-AT1R and anti-ETAR autoantibodies for each disease manifestation and determined RRs for development of specific manifestations in relation to antibody levels (figure 3A with corresponding table) in the Berlin cohort. While lower positive levels of autoantibodies were associated with anti-topo I positivity and renal crisis, patients with high anti-AT1R and anti-ETAR autoantibody levels had a high risk for diffuse SSc and for the development of late complications such as pulmonary hypertension, lung fibrosis and digital ulcers. Such patients also had a higher likelihood of dying from SSc-related complications.

{kind=link}
{kind=link}
{kind=link}
Relationship between anti-AT1R and anti-ETAR autoantibody levels and systemic sclerosis (SSc)-related manifestations and overall survival according to antibody status. (A) RRs for each of the clinical and serological manifestations were stratified according to specific cut-offs for anti-AT1R (black lines) and anti-ETAR autoantibodies (grey lines). Details of receiver operating characteristic analysis including cut-offs, the area under the curve (AUC) and the corresponding sensitivity (Sens) and specificity (Spec) are shown in the table for each manifestation studied. (B) Kaplan–Meier analysis of cumulative survival with number of patients at risk followed up to 48 months after anti-AT1R and anti-ETAR autoantibody testing in 186 patients with SSc. Vertical spikes represent censored patients. AT1R, angiotensin II type 1 receptor; ETAR, endothelin-1 type A receptor; PAH, pulmonary arterial hypertension.
We next tested whether or not anti-AT1R and anti-ETAR autoantibody levels were predictive of SSc-related mortality in a prospective study; 186 patients were followed for 48 months after antibody testing. During the observation period 20 patients died and 18 had anti-AT1R and anti-ETAR autoantibodies (p<0.001, figure 3B). The causes of death were isolated pumonary hypertension (n=6), severe lung fibrosis (n=4), cardiac left ventricular involvement with arrhythmias (n=4) and renal crisis (n=1). High levels of anti-AT1R and anti-ETAR antibodies predicted disease-related mortality.
Discussion
We have developed two standardised solid phase assays based on preservation of native receptor configuration feasible for large-scale diagnostic screening, and identified a high prevalence of autoantibodies directed against AT1 and ETA receptors in patients with SSc. Specific binding of autoantibodies to respective receptors expressed on HMECs was demonstrated by immunoprecipitation. Both autoantibodies were biologically active as they induced direct receptor-mediated ERK1/2 phosphorylation as well as increased profibrotic TGFβ gene expression in HMECs. The biological effects of both autoantibodies could be attenuated by the respective receptor antagonists, providing an additional level of evidence for a specific link between autoantibody binding and receptor activation. High levels of autoantibodies against these receptors were associated with more severe disease manifestations and predicted SSc-related mortality. Anti-AT1R and anti-ETAR autoantibodies may contribute to the pathogenesis of SSc and could represent a link between autoimmunity, endothelial injury and fibrosis. Timely detection of these antibodies raises the prospect for early risk stratification.
Antibody-mediated platelet-derived growth factor receptor (PDGF-R) activation has recently been described in patients with SSc, implicating the role of functional autoantibodies in fibroblast activation by means of prolonged induction of reactive oxygen species.23 The study used a smaller cohort of patients with SSc (n=46) than in our study and did not focus on clinical features. This concept is now largely questioned by two independent studies.24 25 The most significant barrier to the general use of anti-PDGF-R autoantibodies in clinical practice at present is the lack of a standardised assay and the time-consuming setting of the bioassay which precludes screening of larger patient cohorts and investigation of their impact on disease progression.26
We have introduced a diagnostic tool which can provide quantitative antibody binding assessment and is feasible for routine clinical use. The number of cases in our study is sufficient to provide relevant clinical information and depict all relevant aspects of disease heterogeneity. Our hypothesis was also retested in an additional 180 patients from two independent European cohorts from Hungary and Italy. While the finding of autoantibodies against ETAR in human disease is first reported here, anti-AT1R autoantibodies have also been associated with pre-eclampsia and refractory vascular rejection.13 14
In patients with SSc, the presence of anti-AT1R autoantibodies was highly coincident with the presence of anti-ETAR autoantibodies. However, despite this apparent overlap, we were able to demonstrate specific binding of autoantibodies to respective receptors expressed on HMECs by immunoprecipitation. In line with this, the natural ability of antibodies to bind multiple antigens has been described and is currently exploited in engineering ‘two-in-one’ designer antibodies.27 Anti-AT1R and anti-ETAR antibodies have similarities to antiendothelial cell antibodies since endothelial cells express both receptors28 and we have shown biological effects in endothelial cells. In addition to vascular cells, AT1R and ETAR are expressed in fibroblasts, epithelial and immune cells. According to broad target receptor distribution, anti-AT1R and anti-ETAR antibodies are present in the wide spectrum of SSc disease manifestations and are associated with both fibrotic and vascular complications. In contrast, SSc-specific antibodies against cellular components such as kinetochore proteins, topo I and ribonuclear proteins are strongly associated with clinical subsets and patients rarely have multiple antibodies.29 However, there is no evidence for the involvement of these antibodies in disease pathology.
At present we cannot completely rule out the role of B cell hyperreactivity in the generation of target receptor autoantibody responses. B cell hyperreactivity is common in connective tissue diseases, yet we obtained lower levels of receptor antibodies in patients with pSS or RA. Anti-AT1R antibodies occurred in the majority of renal transplant patients in the absence of sensitisation against a panel of alloantigens, a hallmark of B cell hyperreactivity, and humoral responses that would implicate an AT1R antigen-specific response.13 Nevertheless, our aim was not to describe a unique and specific diagnostic tool for the primary diagnosis of SSc in general. Rather, we envisage the use of both receptor autoantibodies as biomarkers for detection of fast disease progression, as demonstrated in the prospective part of the study.
We detected high-titre receptor antibodies in few healthy and disease control serum samples; however, their IgG usually did not induce receptor-mediated ERK1/2 signalling. Interestingly, IgG from one control subject inhibited ERK1/2 signalling which could be enhanced by pharmacological receptor blockers. ERK1/2 phosphorylation is a crucial functional read-out for AT1R since both classical G protein-mediated and G protein-independent effects of ligand binding lead to activation of the mitogen-activated protein kinase pathway.30 Similar phenomena are described in thyroid pathology where some thyroid stimulating hormone receptor antibodies may activate the receptor while others either block or have no influence on signal transduction.31 Whether this also applies to patients with SSc is an extremely complex receptor biology issue to be addressed in future studies.
Our data suggest that simultaneous agonistic antibody-induced AT1 receptor and ETA receptor canonic signalling and downstream gene expression independent of endogenous ligands (Ang II and ET-1) warrant close attention, particularly in patients with SSc. Ang II and ET-1 induce collagen synthesis via target receptor stimulation in fibroblasts.9 12 32 Anti-AT1R and anti-ETAR autoantibodies could participate in fibrogenesis via induction of TGFβ expression. The associations between the increased levels of AT1R and ETAR autoantibodies for fibrotic complications such as lung fibrosis were remarkable, but a little less pronounced than for vascular complications.
Both AT1R and ETAR can be blocked pharmacologically with accessible and tolerable agents. Clinical studies based on antibody detection in different stages of SSc are warranted and could either confirm or refute direct pathophysiological involvement of anti-AT1R and anti-ETAR autoantibodies in SSc.
Acknowledgments
The Bundesministerium für Bildung und Forschung, by sponsoring the German systemic sclerosis Network (DNSS) and the Deutsche Forschungsgemeinschaft through numerous grants to the various investigators, supported the study. The authors are indebted to Professor M Aringer from Carl Carus University Dresden, Professor M Worm from the Charité Berlin, Dr K Egerer and the Charité Laboratory for the detection of anti-topo I, anti-U1RNP and anticentromere antibodies, Dr T Haeupl and Claudia Brueckner from the Medical Faculty of Charité, PD Dr Axel Pruß from the Department of Charité Institute of Transfusion Medicine, Dr Peter Klein-Weigel and Dr Gutsche-Petrack from DRK Berlin-Köpenick for providing samples. The authors also thank Professor J Schneider-Mergener for linear epitope mapping and Dr H D Orzechowski for providing them with HMEC cell line for the in vitro experiments.
References
Supplementary materials
Web only data
Files in this Data Supplement:
Footnotes
↵* EUSTAR investigators
-
Funding CellTrend provided support for the study by their unrestricted serum analyses. The study was also supported by the intramural grant of Charité Universitätsmedizin Berlin, by the Bundesministerium für Bildung und Forschung (BMBF)-funded German Systemic Sclerosis Network (DNSS, BMBF Fkz 01 GM 0310, C6, TP6) and German Scleroderma Foundation (DSS).
-
Competing interests HH is owner of the company CellTrend that has developed the assays together with GR, DNM and DD. Actelion, Pfizer and GSK have provided lecture fees for GR and DD. GR is member of the advisory board for Actelion, GSK and partially for Pfizer and she has received lecture fees from these companies. DD received travel grants from Actelion and lecture fees from Pfizer.
-
Ethical approval Written informed consent to use serum samples for research purposes was obtained from each patient. The institutional review boards of Charité University Hospital, Berlin and University Hospitals in Florence and Pecs approved the study.
-
Provenance and peer review Not commissioned; externally peer reviewed.