Article Text

Abstract
Objective To identify a core set of preliminary items considered as important for the very early diagnosis of systemic sclerosis (SSc).
Methods A list of items provided by European League Against Rheumatism (EULAR) Scleroderma Trial and Research(EUSTAR) centres were subjected to a Delphi exercise among 110 experts in the field of SSc. In round 1, experts were asked to choose the items they considered as the most important for the very early diagnosis of SSc. In round 2, experts were asked to reconsider the items accepted after the first stage. In round 3, the clinical relevance of selected items and their importance as measures that would lead to an early referral process were rated using appropriateness scores.
Results Physicians from 85 EUSTAR centres participated in the study and provided an initial list of 121 items. After three Delphi rounds, the steering committee, with input from external experts, collapsed the 121 items into three domains containing seven items, developed as follows: skin domain (puffy fingers/puffy swollen digits turning into sclerodactily); vascular domain (Raynaud's phenomenon, abnormal capillaroscopy with scleroderma pattern) and laboratory domain (antinuclear, anticentromere and antitopoisomerase-I antibodies). Finally, the whole assembly of EUSTAR centres ratified with a majority vote the results in a final face-to-face meeting.
Conclusion The three Delphi rounds allowed us to identify the items considered by experts as necessary for the very early diagnosis of SSc. The validation of these items to establish diagnostic criteria is currently ongoing in a prospective observational cohort.
Statistics from Altmetric.com
Systemic sclerosis (SSc) is an incurable disease associated with a high morbidity and mortality.1 When the disease has already evolved to a proliferative vasculopathy associated with systemic fibrosis and significant organ damage, the diagnosis of SSc is well established. The American College of Rheumatology (ACR) or Leroy criteria have been provided for the classification of established disease and are also used in practice for the diagnosis of SSc.2 3 However, the ACR criteria perform poorly for the diagnosis of early patients before the disease has produced organ damage.4 5 Therefore, Leroy and Medsger6 proposed potential criteria for the classification of very early SSc, defined by patients with features of SSc who do not fulfil the ACR or LeRoy classification criteria for SSc, consisting of Raynaud's phenomenon, scleroderma-type nailfold capillary pattern and scleroderma selective antibodies.7 Nevertheless, these criteria have not yet been formally validated and are not as yet widely used, as they require autoantibody assessment and nailfold capillaroscopy, which are not yet available in most day-to-day rheumatological offices. Therefore, it is relevant to know which variables are regarded by experts in the field of SSc as necessary to diagnose SSc as early as possible.
Subsequently, there is a need for a core set of practical items to diagnose SSc as early as possible to be able to initiate treatment as early as possible. This study aimed to identify a core set of preliminary criteria necessary for the very early diagnosis of SSc. To this end, a three-round Delphi exercise was performed among experts in the field of SSc.
Methods
In June 2008, experts in the field of SSc from 171 European League Against Rheumatism (EULAR) Scleroderma Trial and Research (EUSTAR) centres were asked to participate in a web-based Delphi exercise. The Delphi exercise was performed between November 2008 and January 2009. The Delphi method is a consensus method for medical and health service research.8 Such methods attempt to assess the extent of agreement (consensus measurement), and to resolve disagreement (consensus development), based on available evidence and supplemented by expert opinion. As opposed to the nominal group technique (expert panel) and to a consensus development conference, a web-based Delphi exercise enables the participation of experts without geographical limitations. In the Delphi procedure participants can give their opinions independently and confidentially without the pressures of face-to-face meetings. Many potential problems related to group dynamics are thus bypassed. Importantly, participants are allowed to change their opinion in consecutive rounds of the process as they are presented with systematic feedback from the results of the previous rounds.
To ensure security and confidentiality, each participant received a personal e-mail invitation, allowing individual access to the questionnaire on a webpage specifically designed and programmed for the present Delphi study. The participants completed the questionnaires online.
In the first step, experts from the EUSTAR centres were asked independently to provide a list of up to 20 items (‘criteria’) they considered as the most important to diagnose very early SSc. These lists were mailed back to the researchers. The different items were then categorised into different domains (eg, skin, vascular or laboratory domains) and aggregated with the removal of duplicates by six independent investigators (JA, VR, CM, VS, IM and IHT) to obtain a final list of items subjected to a Delphi exercise in three rounds. In the case of any uncertainty, a seventh independent investigator (MMC) adjudicated.
In round 1, the EUSTAR participants were asked to choose the items (criteria) they considered as the most important for the very early diagnosis of SSc in clinical practice (‘yes’/‘no’).
In round 2, the participants were asked to re-rate the items accepted after the first round. In order to provide an inclusive and non-restrictive list of criteria, we arbitrarily a priori decided that items were accepted automatically if selected by 30% or more of the participants in round 1 and 40% in round 2.
In round 3, experts rated the clinical relevance and pertinence of the selected items. The clinical relevance of the selected items was rated with a view to get the best face validity for the very early diagnosis of SSc on a numerical 10-point scale (from no (score of 1) to high (score of 10) relevance, a mean score ≥8/10 was arbitrarily a priori considered as relevant). The importance of items was rated in view of the importance in leading to an early referral process (pertinence).
Variables selected after round 2 with clinical relevance of 8/10 or greater and/or considered by experts as important to trigger an early referral process constituted the optimal core set criteria. The core set items were considered as essentials and permitting the very early diagnosis of SSc. Finally, the whole assembly of EUSTAR centres ratified with a majority vote the results in a final face-to-face meeting at the beginning of 2009.
Results
Response rate
Of all 171 invited EUSTAR centres, 110 physicians from 85 centres provided lists of items they considered important for the very early diagnosis of SSc. The 1270 initial items were categorised and aggregated to a condensed list of 11 domains containing 121 items to be submitted to the Delphi procedure. Ninety-two physicians (84%) participated in round 1 of the Delphi exercise. Eighty (73%) participated in round 2, 75 (67%) in round 3 and 68 (63%) completed all three rounds.
Items selected after Delphi rounds 1 and 2
After the first round, 13/121 criteria were selected by 30% or more of the participants based on their importance for the very early diagnosis of SSc (table 1). These 13 items were then rated by the participants in the second round and eight criteria were selected by 40% or more of the participants based on their importance for the very early diagnosis of SSc (table 1).
Results of Delphi rounds 1 and 2
These first two Delphi rounds resulted in a preliminary list of three domains containing eight criteria: skin domain (puffy fingers, puffy swollen digits turning into sclerodactily, skin oedema); vascular domain (Raynaud's phenomenon, nailfold capillaroscopy examination with presence of a scleroderma pattern of vascular abnormalities) and laboratory domain (positivity of antinuclear, anticentromere and antitopoisomerase-1 antibodies).
Results of Delphi round 3
Clinical relevance of the selected criteria
Five of the eight items were considered by the experts to have high clinical relevance to get the best combined sensitivity/specificity for the very early diagnosis of SSc (figure 1), with a mean score of 8/10 or greater (abnormal capillaroscopy with scleroderma pattern 8.7±1.8, antitopoisomerase-1 antibodies 8.4±1.7, puffy swollen digits turning into sclerodactily 8.3±2.0, anticentromere antibodies 8.1±1.7 and Raynaud's phenomenon 8.0±2.1). The clinical relevance of the three remaining items was 5.7±2.4, 6.4±1.9 and 5.9±1.9, respectively, for antinuclear antibodies, puffy fingers and skin oedema.

Ratings of clinical pertinence after Delphi round 3 (lines: numerical scale from 1 to 10, columns: percentage of voters).
Pertinence of the items for referral
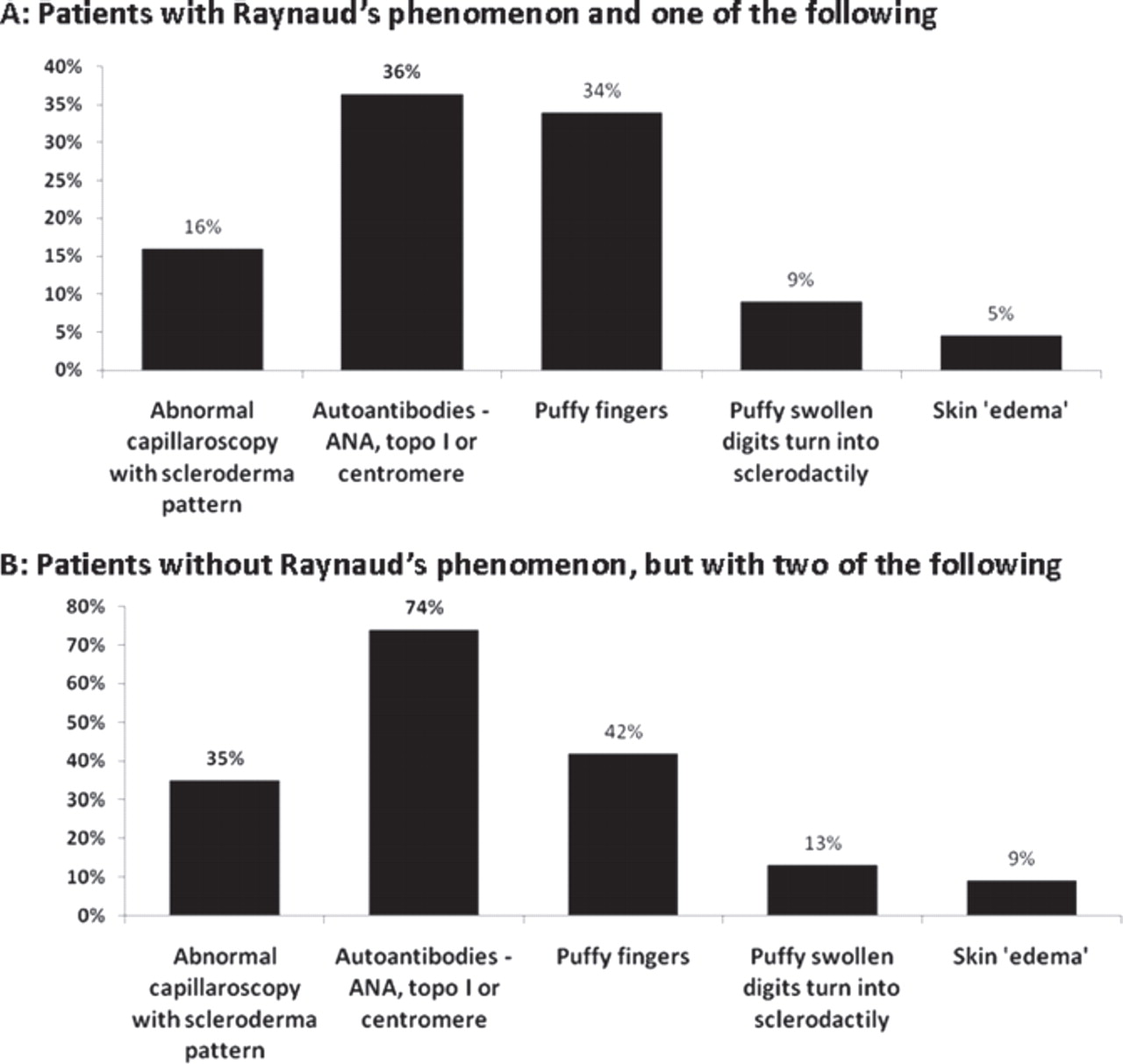
To define the items (clinical manifestations) giving rise to a suspicion of very early SSc and that would suggest that a patient should be referred for expert evaluation, participants were then asked to rate four proposals for early referral, answering the question ‘As a specialist in diagnosing SSc, who would you like to see to be referred to you by, for example, family physicians for very early diagnosis of SSc?’ The results are provided in figures 2 and 3. It is noteworthy that Raynaud's phenomenon as a single manifestation and Raynaud's phenomenon in combination with puffy fingers were considered to be major signs, which should trigger referral to a specialist for the very early diagnosis of SSc (figure 2). The preferred signs leading to referral in association or not with Raynaud's phenomenon were puffy fingers and autoantibodies (figure 3A,B).
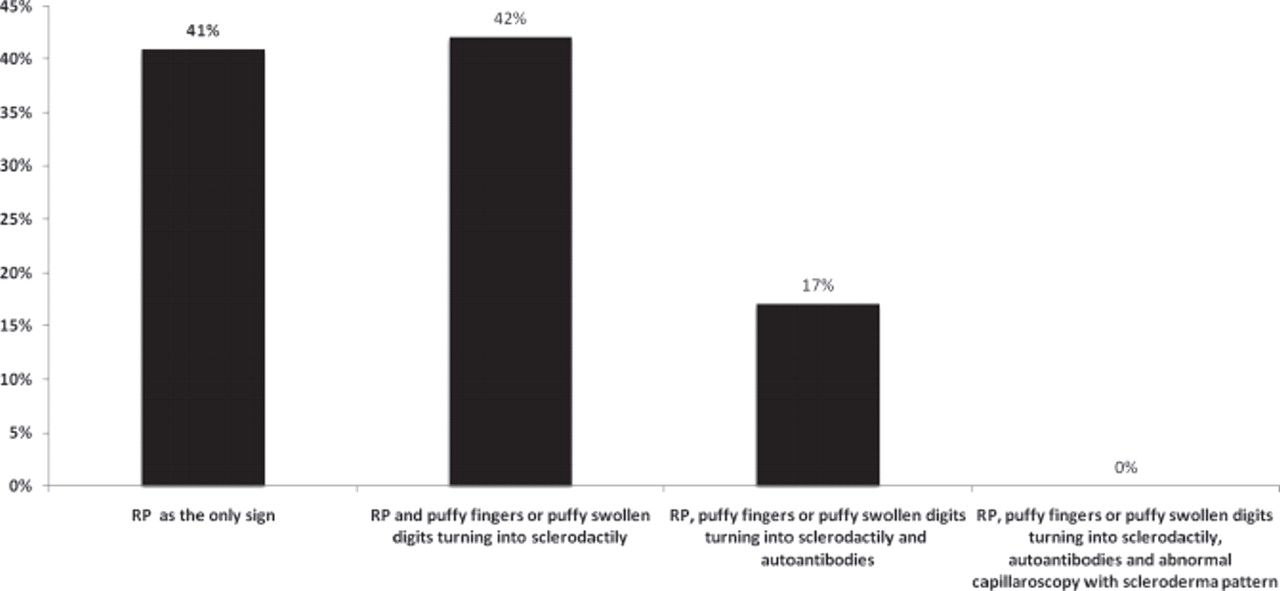
Answers from participants to the question: ‘As a specialist in diagnosing SSc, who would you like to see to be referred to you for very early diagnosis of SSc?’. SSc, systemic sclerosis. RP, Raynaud's phenomenon.
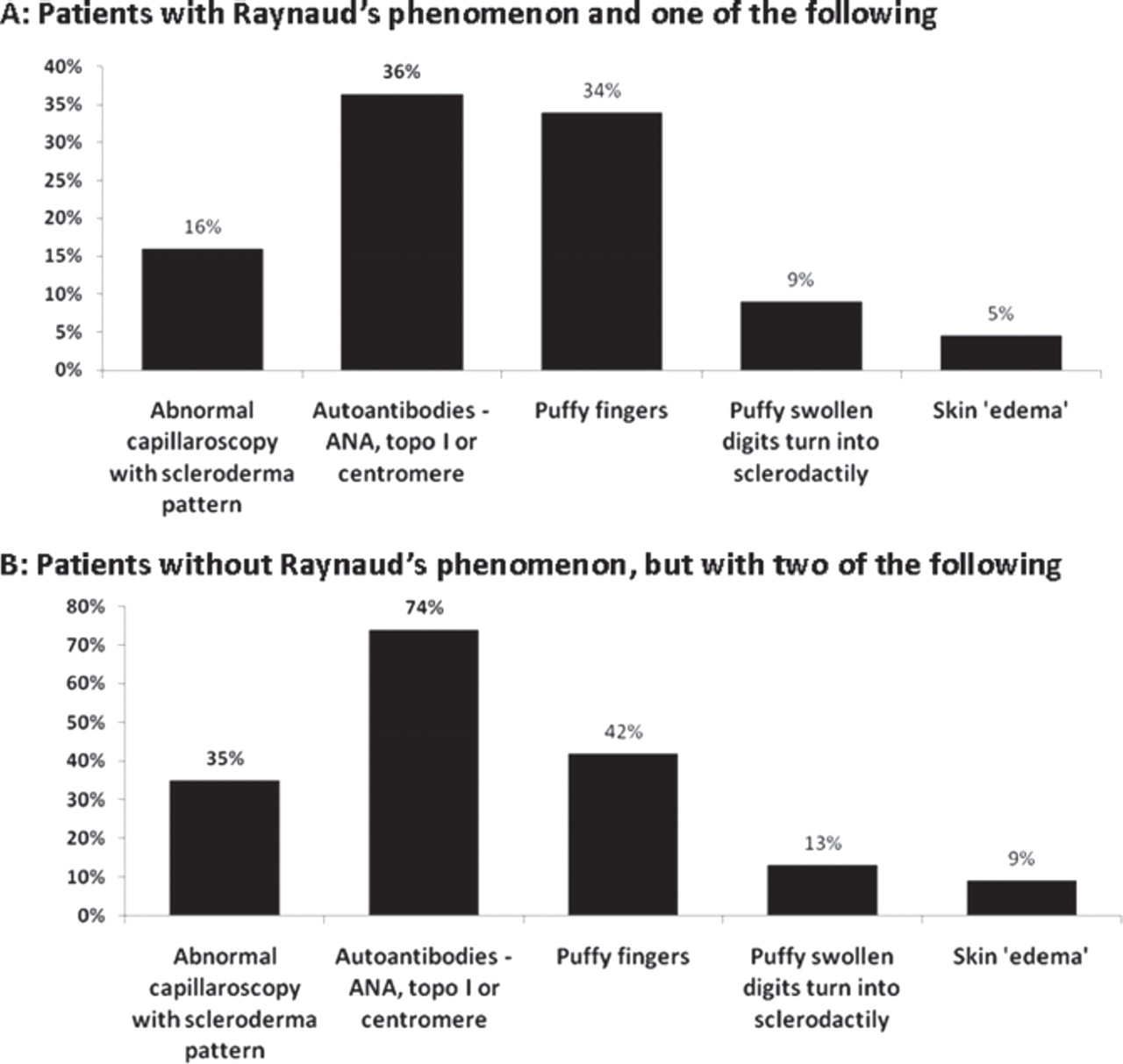
Answers from participants to the question: ‘As a specialist in diagnosing SSc, who would you like to see to be referred to you for very early diagnosis of SSc?’ considering or not the presence of Raynaud's phenomenon. ANA, antinuclear antibodies; topo I, topoisomerase I antibodies; SSc, systemic sclerosis.
The results of the three rounds were presented during a final face-to-face meeting of the EUSTAR assembly in January 2009, which led to a final consensus with majority vote, thus corroborating the face validity of the Delphi (table 2). Accordingly, Raynaud's phenomenon, puffy fingers and positivity of antinuclear antibodies were regarded as ‘red flags’, and nailfold capillaroscopic ‘scleroderma type’ abnormalities and specific SSc antibody positivity as necessary tools to confirm the suspicion of very early SSc. Figure 4 shows this as an algorithm to guide the physician in practice toward a definite diagnosis of SSc.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A behavioural flow chart for patients in whom the very early diagnosis of systemic sclerosis (SSc) should be considered is proposed. Red flags should trigger the differential diagnosis of SSc and guide the general practitioner to send the patient to the referral centre where capillaroscopy and specific autoantibodies are ordered and the diagnosis of very early SSc is made. HRCT, high resolution CT; PFT, pulmonary function tests.
Final list of criteria determined and ratified by the EUSTAR assembly
Discussion
A definition of ‘very early SSc’ as a state characterised by Raynaud's phenomenon, puffy fingers, disease-specific autoantibodies and pathognomonic microvascular alteration detected by capillaroscopy (requiring at least two, or better, all four items to be present) has recently been proposed.9 These parameters were also considered as the main clinical features to define the phase before skin becomes really involved.10 These items differ from the early SSc criteria as proposed by LeRoy and Medsger6 in the extent of cutaneous signs of scleroderma.
Our data confirm these previous proposals and refine them among a large number of experts in an international forum. We clearly identify a set of preliminary items for the very early diagnosis of SSc that can be the substrate for a full validation of the definition in a cohort of patients. This exercise solidly establishes the face validity of the definition, leaving content, criterion, reliability, reproducibility, feasibility and discrimination for further research.
The procedures allowed us to identify three different domains (skin, vascular and laboratory domains) containing the following items related to symptoms/signs, laboratory examinations and nailfold capillaroscopy examination: Raynaud's phenomenon, puffy fingers/puffy swollen digits turning into sclerodactily, antibodies (antinuclear, anticentromere and antitopoisomerase-I antibodies) and abnormal capillaroscopy with scleroderma pattern. Raynaud's phenomenon, puffy fingers and antinuclear antibodies were considered by the whole assembly of EUSTAR as ‘red flags’ for the general practitioner leading to the suspicion of very early SSc, and should prompt the general practitioner to refer the patient to a specialist for the definitive diagnosis of very early SSc (figure 4).
The item puffy fingers turning into sclerodactily, a more specific sign of SSc than puffy fingers because it specifically marks an evolution upon time to a fibrotic phenotype, was selected after the two first rounds and was considered by the experts to have high clinical relevance in round 3. The item puffy fingers, a non-specific clinical sign of SSc that can also be present in other diseases, such as undifferentiated connective tissue disease or mixed connective tissue disease, was considered by experts to have a low clinical relevance. However, puffy fingers were one of the preferred signs that should trigger referral to a specialist for the very early diagnosis of SSc. Finally, during the face-to-face meeting, the experts preferred to consider puffy fingers, although not specific to SSc, as a red flag rather than puffy swollen digits turning into sclerodactily, which is a sign of established SSc.
The further prospective validation of these criteria will require the consideration of this evolution from puffy fingers to sclerodactily, both as separate items and in terms of the time frame for the change from ‘puffiness’ to ‘sclerodactily’.
Commonly available specific autoantibodies (anticentromere and antitopoisomerase-I antibodies) and nailfold capillaroscopy were considered as the preferred confirmatory diagnostic tools to diagnose a patient with very early SSc with a high probability. The predictive value of these diagnostic tools has recently been assessed in 586 patients with Raynaud's phenomenon and no definite connective tissue disease.11 Patients were evaluated for microvascular damage by nailfold capillaroscopy and for SSc-specific autoantibodies by specific assays, in order to identify markers predicting the evolution to definite SSc. Of these patients, 12.6% developed definite SSc over the years. The results showed that, in patients with Raynaud's phenomenon and abnormal capillaroscopy with scleroderma pattern together with an SSc-specific autoantibody at baseline, there was a good probability of 79.5% developing definite SSc after up to 9 years of observation.11
When interpreting the outcomes of this Delphi exercise, certain methodological considerations should be taken into account. We applied the usual elements of the Delphi technique, including a structured flow of information, feedback to the participants and anonymity for the participants during the exercise itself (thus not inhibiting their input). Many Delphi exercises utilise a small number of experts and sometimes also include face-to-face meetings.12 13 In the present exercise, the internet was used to reach a consensus, thus allowing a larger number of participants to be included. It was also relatively cost-efficient, because only one face-to-face meeting was necessary for the final validation of the results. The response rate we achieved was high and approximates the rate obtained in the exercises previously published, probably as a result of the fact that all participants were EUSTAR members.14 15
The data obtained by our Delphi investigation have an additional value to the prospective data reported by Koenig et al,11 but show an important change of attitude towards the diagnosis of very early SSc, suggesting an awareness of the need for very early diagnosis.
It must be emphasised that the final core set of criteria of this Delphi survey is the subjective opinion of experts in the field. This should not be confused with the validation of particular criteria, which was not the aim of the present study. The final core set defined by this Delphi survey can thus be seen as a priority list for the domains and, possibly, items for the diagnosis of very early SSc, for which a full validation study must still be done. This validation, now ongoing in a prospective observational cohort, will determine the discriminatory (sensitivity and specificity) and predictive value (positive predictive value and negative predictive value) of chosen features.
The reason to diagnose very early SSc rests on the assumption that the use of these preliminary criteria will lead to earlier diagnosis and earlier treatment of SSc, which should improve long-term outcome in SSc.9 In this perspective, the results of this Delphi exercise and the further validation of the criteria identified in this study aim to improve the management of SSc by means of earlier, easier and more reliable screening of individuals at risk in order to establish a definite diagnosis of very early SSc (VEDOSS study). This will allow finding an optimal non-invasive screening tool or a combination of screening tools, to increase the chance of accurately detecting very early SSc patients, diagnosis as later confirmed by ACR, LeRoy6 16 or the new incoming EULAR/ACR criteria.
Acknowledgments
The authors would like to thank the European League Against Rheumatism for excellent support.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
EUSTAR Group F De Keyser, Department of Rheumatology, Ghent University Hospital, Belgium; A Sulli, C Pizzorni, Research Laboratory and Division of Rheumatology Department of Internal Medicine, University of Genova, Italy; B Maurer, Department of Rheumatology, University Hospital Zurich, Zurich, Switzerland; S Sierakowsky, Department of Rheumatology and Internal Diseases, Medical University of Bialystok, Bialystok, Poland; O Kowal-Bielecka, Department of Rheumatology and Internal Diseases, Medical University of Bialystok, Bialystok, Poland; P Coelho, Instituto portugues de Reumatologia, Lisboa, Portugal; G Riemekasten, Department of Rheumatology-Charité University Hospital, Berlin, Germany; S Rednic, I Nicoara, Clinica Reumatologie – University of Medicine and Pharmacy ‘iuliu Hatieganu’ Cluj, Cluj-Napoca, România; R Caporali, Unità Operativa e Cattedra di Reumatologia, IRCCS Policlinico S, Matteo, Pavia, Italy; J Štork, Department of Dermatology the 1st Faculty of Medicine, Charles University, Prague, Czech Republic; M Inanc, Istanbul Medical Faculty, Department of Internal Medicine, Division of Rheumatology, Istanbul, Turkey; P Carreira, Hospital Universitario 12 de Octubre, Servicio de Reumatología, Madrid, Spain; S Novak, Department of Rheumatology and Clinical Immunology, Internal Medicine, KBC Rijeka, Croatia; C Varju, Department of Immunology and Rheumatology, Faculty of Medicine, University of Pecs, Pecs, Hungary; C Chizzolini, C Ribi, Immunology and Allergy, University Hospital, Geneva, Switzerland; EJ Kucharz, A Kotulska, M Widuchowska, Department of Internal Medicine and Rheumatology, Medical University of Silesia, Katowice, Poland; J Richter, Rheumatology Department, Heinrich-Heine University, Düsseldorf, Germany; A Sipek-Dolnicar, B Rozman, University Medical Center Ljublijana, Division of Internal Medicine, Department of Rheumatology, Ljubljana, Slovenia; A Gabrielli, G Moroncini, Istituto di Clinica Medica Generale, Ematologia ed Immunologia Clinica Polo Didattico Università Politecnica delle Marche, Ancona, Italy; D Farge, C Durant, Department of Internal Medicine, Hopital Saint Louis, Paris, France; HP Kiener, E Rath, Department of Medicine III, Division of Rheumatology, Medical University of Vienna, Vienna, Austria; P Airo, Servizio di Reumatologia e Immunologia Clinica, Spedali Civili, Brescia, Italy; FA Wollheim, Department of Rheumatology, Lund University Hospital, Lund, Sweden; N Hunzelmann, Universitätshautklinik Köln, Köln, Germany; S Bombardieri, A Della Rossa, L Bazzichi, Department of Internal Medicine, Rheumatology Unit, University of Pisa-Santa Chiara, Pisa, Italy; R Pellerito, M Saracco, Ospedale Mauriziano, Centro di Reumatologia, Torino, Italy; C Denton, Centre for Rheumatology, Royal Free and University College London Medical School, London, UK; M Vonk, F Van den Hoogen, Sint Maartenskliniek, Nijmegen, The Netherlands; N Damjanov, Institute of Rheumatology, Belgrade, Serbia and Montenegro; I Kötter, Universitätsklinikum Tübingen, Medizinische Klinik und Poliklinik, Tübingen, Germany; S Heitmann, Department of Rheumatology, Marienhospital Stuttgart, Stuttgart, Germany; M Seidel, Medizinische Univesitäts-Poliklinik, Department of Rheumatology, Bonn, Germany; P Hasler, Kantonsspital Aarau, Rheumaklinik und Institut für Physikalische Medizin und Rehabilitation, Aarau, Switzerland; JM Van Laar, James Cook University Hospital, Middlesbrough, UK; MJ Salvador, JA Pereira Da Silva, Reumatologia, Hospitais da Universidade, Coimbra, Portugal; S Jacobsen, Department of Rheumatology Rigshospitalet, University of Copenhagen, Copenhagen, Denmark; M Worm, Charité – Universitätsmedizin Berlin, Department of Dermatology and Allergy, Berlin, Germany; A Kuhn, Department of Dermatology, University of Münster, Münster, Germany; T Nevskaya, EL Nasonov, Institute of Rheumatology, Russian Academy of Medical Science, Moscow, Russia; R Scorza, UO Immunologia Clinica Centro di Riferimento per le Malattie Autoimmuni Sistemiche, Milano, Italy; H Nielsen, Department of Rheumatology and Endocrinology, Herlev, Denmark; RM Silver, Division of Rheumatology and Immunology, Charleston, South Carolina, USA; E Hachulla, D Launay, Department of Internal Medicine, Hôpital Claude Huriez, Lille, France; G Valesini, Divisione Di Reumatologia – Universita Di Roma La Sapienza, Roma, Italy; R Ionescu, D Opris, ‘Carol Davila’ University of Medicine and Pharmacy, Department of Internal Medicine and Rheumatology, Bucharest, Romania; N Del Papa, W Maglione, D Comina, Rheumatology, Gaetano Pini, Milano, Italy; G Udrea, C Ciurtin, R Ionitescu, C Mihai, Clinic of Internal Medicine and Rheumatology, Dr I Cantacuzino Hospital and Early Arthritis Center, Bucharest, Romania; C Sunderkötter, Department of Dermatology, University of Münster, Münster, Germany; Jae-Bum Jun, Hanyang University Hospital for Rheumatic Diseases, Seoul, Republic of Korea; C Derk, Thomas Jefferson University, Philadelphia, USA; S Alhasani, L Alhajjar, Rheumatology and Rehabilitation Department, Ibnsina Teaching Hospital, Mosul, Iraq; E Ton, University Medical Centre Utrecht, Utrecht, The Netherlands; J Seibold, Division of Rheumatology University of Connecticut Health Center, Farmington, Connecticut, USA; P Nash, Rheumatology Research Unit, Queensland, Australia; L Mouthon, Department of Internal Medicine, Hôpital Cochin, Paris, France; CA von Mühlen, Rheuma Clinic, Porto Alegre, Brazil; B Krummel-Lorenz, P Eilbacher Endokrinologikum, Frankfurt, Germany; R Westhovens, E De Langhe Catholic University of Leuven, Leuven, Belgium; M Mayer, B Anic, M Baresic, University Hospital Centre Zagreb, Division of Clinical Immunology and Rheumatology, Zagreb, Croatia; F Stoeckl, Klinikum Darmstadt, Med Klinik III, Nephrology, Hypertension and Rheumatology, Darmstadt, Germany; M Üprus, East-Tallinn Central Hospital, Department of Rheumatology, Tallinn, Estonia; S Popa, Department of Rheumatology, Republican Clinical Hospital, Chisinau, Republic of Moldova; M Buslau, European Centre for the Rehabilitation of Scleroderma, Rheinfelden, Switzerland; B Granel, Service de Médecine Interne, Hôpital Nord, Marseille, France; T Zenone, Department of Medicine, Unit of Internal Medicine, Valence, France; A Mathieu, A Vacca, II Chair of Rheumatology, University of Cagliari, Monserrato, Italy; P Amerio, Clinica Dermatologica Università di Chieti, Chieti, Italy; T Tourinho, L Lonzetti, M Lemos Lopes, Complexo Hospitalar Santa Casa de Porto Alegre, Porto Alegre, Brazil; R de Souza, University of São Paulo – Rheumatology Division, Faculdade de Medicina da Universidade de São Paulo, São Paulo, Brazil; D Vealex, Department of Rheumatology, Bone and Joint Unit, St Vincent's University Hospital, Dublin, Ireland; P Caramaschi, Dipartimento di Medicina Clinica e Sperimentale, Università di Verona, Verona, Italy; A Balbir-Gurman, Y Braun, Shine Department of Rheumatology, Rambam Health Care Campus, Haifa, Israel; S Ullman, Department of Dermatology, University Hospital of Copenhagen, Copenhagen, Denmark; M Szmyrka-Kaczmarek, E Morgiel, Department of Rheumatology and Internal Diseases, Wroclaw University of Medicine, Wroclaw, Poland; M Vanthuyne, Université catholique de Louvain, Bruxelles, Belgium; M Meurer, P Rehberger, Department of Dermatology, University Medical Center Carl Gustav Carus, Dresden, Germany; C Müller, Universidade Federal do Paraná, Curitiba-Paraná, Brazil; P Sampaio-Barros, University of São Paulo – Rheumatology Division São Paulo, Brazil.