Article Text

Abstract
Background The availability of increasing numbers of biological agents for the treatment of rheumatoid arthritis (RA) offers several therapeutic options. While all biologicals have proven effective in trials, very limited direct comparisons are available. The objective of the present work was to compare the efficacy of biologicals (anti-tumour necrosis factor (TNF) agents, rituximab, abatacept, tocilizumab) in patients with RA with active disease and (i) an inadequate response (IR) to methotrexate (IR-MTX), (ii) an IR to anti-TNF agents (IR-anti-TNFs) using indirect comparisons.
Methods Randomised clinical trials were identified examining the efficacy of a biological agent in RA at 6 months in patients with an IR-MTX or with an IR-anti-TNF. To compare the relative efficacy of biologicals, adjusted indirect comparison meta-analytic methods to estimate the ORs of achieving a 50% improvement according to American College of Rheumatology criteria (ACR50) response at 6 months were used.
Results A total of 18 published trials and 1 abstract were included in the analyses. In IR-MTX, anti-TNFs had the same probability of reaching an ACR50 compared to ‘non-anti-TNF biologicals’ taken together (OR 1.30, 95 % CI 0.91 to 1.86). However, when compared to specific biological agents, anti-TNFs demonstrated a higher probability of reaching an ACR50 than abatacept (OR 1.52, 95 % CI 1.0 to 2.28), but not in comparison to rituximab and tocilizumab. In IR-anti-TNF, rituximab demonstrated a higher probability of achieving an ACR50 than tocilizumab (OR 2.61, 95% CI 1.10 to 6.37), but no significant differences existed between rituximab, tocilizumab, abatacept and golimumab.
Conclusions In a meta-analysis of randomised clinical trials of patients with IR-MTX, anti-TNFs demonstrated a higher probability of achieving an ACR50 response than abatacept. In IR-anti-TNF, no difference was found between rituximab, tocimizumab, abatacept and golimumab.
Statistics from Altmetric.com
Introduction
In rheumatoid arthritis (RA), patients with inadequate responses (IR) to conventional disease-modifying antirheumatic drugs (DMARDs), have benefited from biological agents that target various elements involved in the pathogenesis of RA: tumour necrosis factor (TNF) with anti-TNF agents (infliximab, adalimumab, certolizumab and golimumab and etanercept), T cells with anti-cytotoxic T lymphocyte antigen 4 antibodies (abatacept), B cells with anti-CD20 antibodies (rituximab) or interleukin (IL)-6 (tocilizumab). We did not include anti-IL-1 biologicals (anakinra) in this meta-analysis because these agents are not widely available for the treatment of RA. All of these biologicals have demonstrated efficacy in placebo-controlled randomised clinical trials (RCTs) in patients with RA with active disease despite conventional DMARDs. Newer biologicals, that is rituximab, abatacept, golimumab, certolizumab and tocilizumab, have further demonstrated efficacy in patients with RA with an IR to anti-TNF agent (anti-TNFs).
The availability of increasing numbers of biologicals in RA suggests the need to establish the relative benefit of these agents in different clinical situations. However, placebo-controlled RCTs do not allow direct comparisons between the various biological agents. To date there are no RCTs of two biologicals using optimal dosing. Meta-analysis allows indirect comparisons between two interventions and has been previously used to compare and demonstrate similar, but not identical efficacy of infliximab, etanercept and adalimumab in patients with active RA despite use of methotrexate (MTX).1
The aim of this meta-analysis was to compare the relative efficacy at 6 months of available biologicals in two common clinical situations in established RA: (i) IR-MTX, (ii) IR-anti-TNFs.
Methods
We performed a systematic review of the literature and meta-analyses of the efficacy of biologicals in RA with concomitant DMARDs (MTX or other) in two clinical situations: (i) active disease despite MTX, (ii) after an IR (defined as lack of efficacy or an adverse event) to an anti-TNF agent.
A systematic review of the literature was conducted according to the Cochrane Collaboration guidelines and performed independently by two rheumatologists (CS and AF).2
The search included published studies until October 2009 in the three following electronic databases: Medline, Cochrane Central and Embase. We used several combinations of keywords (listed in the supplementary material), without limitation of time, language or journal. The literature search was extended by hand search of references. We completed the search with abstracts from recent scientific meetings (ACR and EULAR abstracts of the past 2 years (2007–2009)), and when needed we contacted the pharmaceutical firms involved in biotherapies for RA.
The inclusion criteria used for selecting the studies were established a priori. We only included double-blinded RCTs of adult patients with established RA after an IR to MTX or to anti-TNF treatments, and who received a biological agent or a placebo in combination with MTX or another DMARD for at least 24 weeks.
Data collection was performed by two rheumatologists independently (CS and WK). Data collected included study design (rescue, primary and secondary endpoints, intention to treat (ITT) analysis, follow-up, number of completers), baseline characteristics (gender, age, disease duration, proportion of rheumatoid factor, previous DMARDs), study intervention and concomitant treatments. Regarding the doses of biological agents, we focused on dosages used in clinical practice: 50 mg weekly for etanercept, 40 mg every other week for adalimumab, 3–10 mg/kg/8 weeks for infliximab, 400 mg at weeks 0, 2, 4 followed by 200 mg every other week for certolizumab, 50 mg every 4 weeks for golimumab, 1000 mg at days 1 and 15 for rituximab, 10 mg/kg/month for abatacept and 8 mg/kg/month for tocilizumab.
As primary outcome, we chose the ACR50 response rate (at least 50% improvement according to the American College of Rheumatology criteria in the number of swollen and tender joints, and in three of the following five parameters: physician global assessment of disease, patient global assessment of disease, patient assessment of pain, C reactive protein or erythrocyte sedimentation rate and the Health Assessment Questionnaire (HAQ score) at 24–30 weeks).3 While the ACR20 has been used as the primary outcome in many RCTs, we felt that the level of improvement involved with an ACR20 response was clinically not relevant enough, given the investment associated with biologicals.
Statistical analysis
If more than one RCT was available for a given agent, the data were pooled across the trials using the random effect model (Mantel–Haenszel method). Heterogeneity for ACR50 response rate was measured by I2 statistic.
We then used indirect comparisons to evaluate the relative efficacy of the various biologicals compared to a common comparator (placebo group), as described by Bucher et al.4 and Song et al.5 The comparisons were thus adjusted by the level of response to the placebo group. Indirect comparisons assume that the relative efficacy of a given intervention is consistent across different trials of that intervention.
A recent Cochrane meta-analysis with indirect comparisons demonstrated similar efficacy of etanercept, adalimumab and infliximab (based on ACR50 response rates).6 We first performed indirect comparisons for ACR50 response rates between ‘older’ anti-TNFs (infliximab, adalimumab and etanercept) and (i) certolizumab, (ii) golimumab. If no significant difference existed we assumed that all anti-TNFs have similar levels of efficacy and considered them as a group. Thus we planned to compare all anti-TNFs to biological agents of a different mechanism of action as a group, before comparing biological agents by mechanism of action among themselves. The various indirect comparisons are listed in table 1. We also performed sensitivity analyses to examine the impact of trial design (ie, trials with a rescue design) and patient characteristics.
Indirect comparisons between biologicals in the two populations of patients with rheumatoid arthritis (RA)
The results are given as ORs of reaching an ACR50 response with their 95% CIs. We used Statistical Analysis Software for windows V.9.1.3 (SAS Institute Inc., Cary, North Carolina, USA) and Review Manager V.5.0 (http://review-manager.software.informer.com/). A p value of <0.05 was taken to indicate statistical significance.
Results
Systematic review of the literature
The selection process of relevant published trials is summarised in the supplementary material. In all, 17 published studies and 1 abstract were retrieved and included in the analysis.7,–,25 A total of 15 studies, compared the efficacy of a biological agent to a placebo in patients with active disease despite MTX and 5 trials that compared the efficacy of a biological to a placebo in patients with active disease with IR to an anti-TNF agent.7,–,25 The concomitant treatment in biological and placebo groups was MTX in all RCTs, except for one.23 The definition of active disease varied across the trials that is, at least four to nine swollen and tender joints, and the presence of an acute phase response or morning stiffness.
The main characteristics of included trials are summarised in the supplementary material. All trials performed an ITT analysis and patients who discontinued therapy for any reason or received rescue therapies were considered as non-responders. Table 2 shows the ACR50 response rates for all included studies and arms.
Number of patients achieving or not the American College of Rheumatology 50% improvement (ACR50) response rates at week 24 in biological and placebo groups for all included studies (for IR-MTX and IR-anti-TNF RA)
Efficacy of biologicals in active RA despite MTX
We included 9 trials with anti-TNFs (2476 patients), 3 with rituximab (604 patients), 3 with abatacept (1138 patients) and 1 with tocilizumab (409 patients).7,–,21 The main patient characteristics were similar across these trials: most patients were women (70% to 90%), with a mean age at baseline between 49 and 56 years, long-standing RA (mean disease duration between 6 and 13 years) and with a positive rheumatoid factor in 73% to 100% of patients.
First, we pooled the results of trials of biologicals aiming for the same targets using the Mantel–Haenszel method and random effect models. Indirect comparisons of ACR50 response rates at 6 months between ‘older’ anti-TNFs (infliximab, adalimumab and etanercept) and ‘newer’ ones didn't find any significant difference: for certolizumab (p=0.08) and golimumab (p=0.33). These first results allowed us to consider all anti-TNFs as a group.
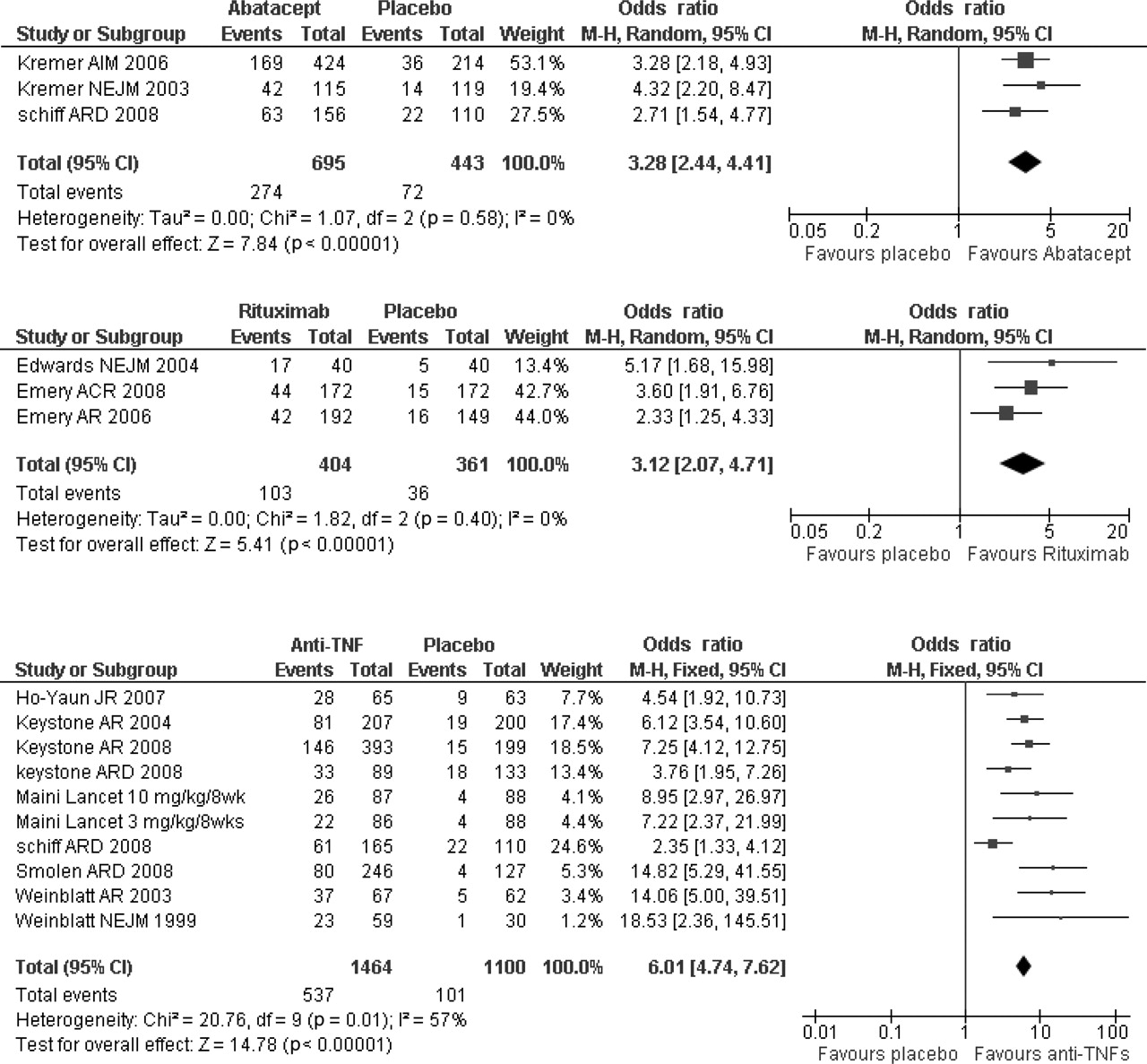
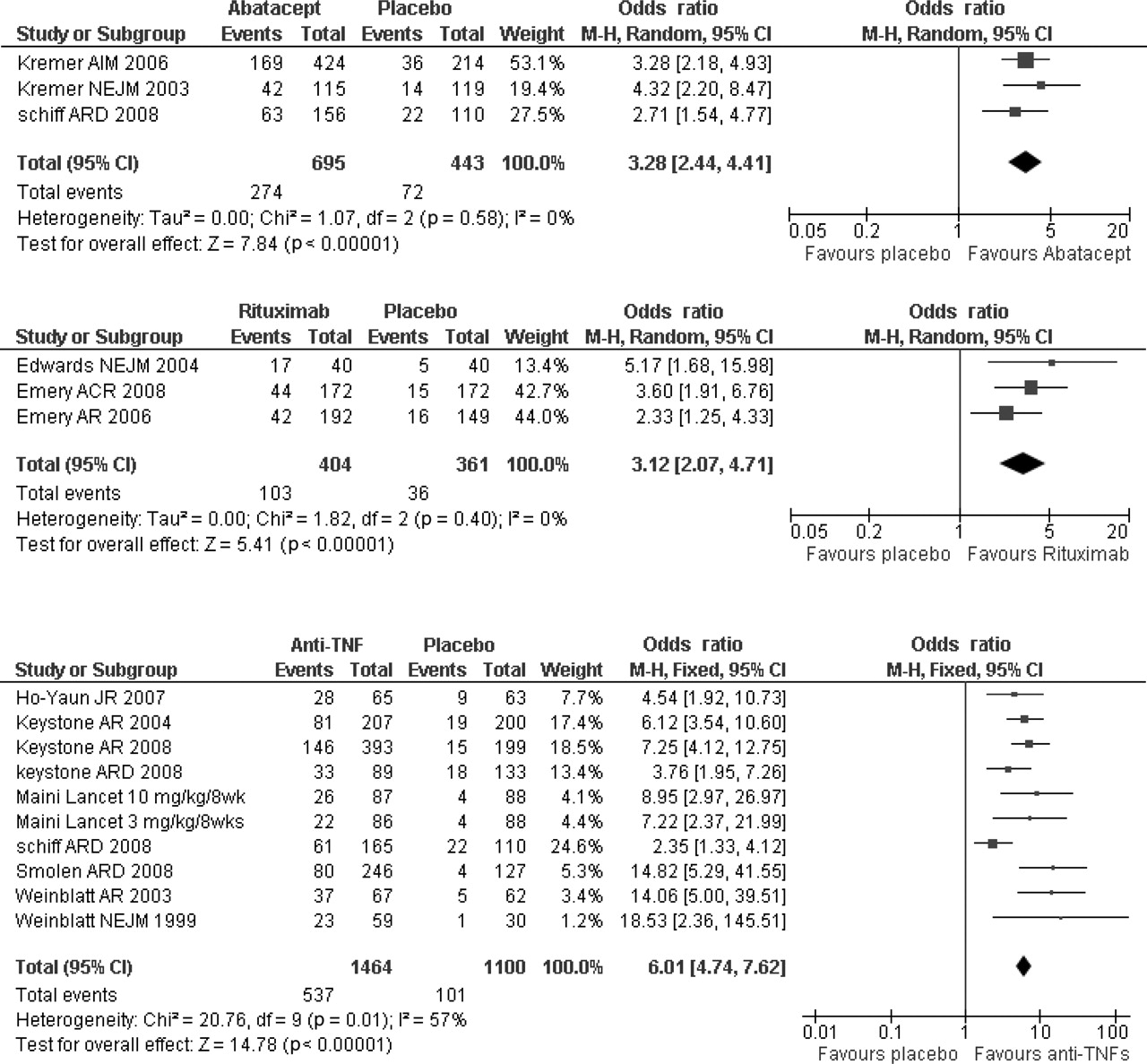
Heterogeneity for ACR50, as measured by the I2 statistic, was 0% for abatacept and rituximab (ie, low) and was 57% for anti-TNFs, considered as substantial. The results demonstrated that abatacept, rituximab and anti-TNFs (with MTX) provided a significantly higher probability of obtaining an ACR50 response at 6 months than MTX alone: OR 3.3 (95% CI 2.4 to 4.4), OR 3.1 (2.1 to 4.7) and OR 6.0 (4.7 to 7.6), respectively (figure 1).
{kind=link}
Forest plots showing the ORs for American College of Rheumatology 50% improvement (ACR50) response rates at week 24 in patients with active rheumatoid arthritis (RA) despite methotrexate receiving abatacept7 19 20 or rituximab 16,–,18 or anti-tumour necrosis factor agents (TNFs) (infliximab, etanercept, adalimumab, certolizumab and golimumab)7,–,15 versus placebo, using the Mantel–Haenszel method (random effect model).
The results of the adjusted indirect comparisons between biologicals are shown in table 3. Anti-TNF agents provided a significant higher probability of achieving an ACR50 response at 6 months than the non-anti-TNF biologicals taken together (OR 1.55, 95% CI 1.12 to 2.16). In a sensitivity analysis, we excluded trials with a rescue regimen from the ‘all anti-TNF’ group: (1) GO-FORWARD trial (golimumab), which did not change the results (OR 1.64, 95% CI 1.17 to 2.32, p=0.004) and (2) RAPID 1 and 2 (certolizumab), which qualitatively changed the results (OR 1.30, 95% CI 0.91 to 1.86, p=0.15).
Indirect comparisons between biologicals in active rheumatoid arthritis (RA) despite methotrexate (MTX) expressed in ORs for American College of Rheumatology 50% improvement (ACR50) response rate at 6 months (weeks 24 to 30), with sensitive analysis (exclusion of certolizumab trials)
Specifically, anti-TNFs had a higher probability of reaching an ACR50 compared to abatacept (OR 1.81, 95% CI 1.23 to 2.65) (even after excluding certolizumab trials, see table 3) but not in comparison to tocilizumab (OR 0.92, 95% CI 0.51 to 1.63). There was only a trend when we compared to rituximab (OR 1.62, 95% CI 1.0 to 2.66), but not after excluding certolizumab trials (OR 1.36, 95% CI 0.81 to 2.27).
When comparing non-anti-TNF biologicals among themselves, tocilizumab was significantly more effective than abatacept (OR 1.97, 95% CI 1.08 to 3.59) in terms of achieving an ACR50. No difference was found when we compared tocilizumab to rituximab and abatacept to rituximab.
Efficacy of biologicals in patients with RA with an IR to anti-TNFs
We analysed 5 trials; 2 with rituximab (DANCER and REFLEX trials; 581 patients), 1 with abatacept (ATTAIN trial; 391 patients), 1 with tocilizumab (RADIATE trial; 334 patients) and 1 with golimumab (GO-AFTER trial; 205 patients).17 22,–,25 In the GO-AFTER trial, 30% of patients did not receive DMARD as concomitant treatment; we included only the subgroup of patients who received golimumab (50 mg/4 weeks) or placebo with concomitant MTX.
The main patient characteristics were similar across these trials: most patients were women (77% to 84%), with a mean age at baseline between 52.2 and 54 years, a mean duration of the disease between 11.4 and 12.6 years and rheumatoid factor positivity in 73% to 79% of patients. Anti-TNFs were stopped for inadequate efficacy in 92% and 58% of patients in REFLEX and GO-AFTER studies, respectively.22 25 The proportion of patients who withdrew for lack of efficacy was not available for abatacept and tocilizumab trials. Only 1.5% to 2.3% of patients included in the abatacept trial previously received two anti-TNFs. This proportion was higher for rituximab (40%), golimumab (25%) and tocilizumab (32% to 44%). In the rituximab, golimumab and tocilizumab studies, all patients received MTX as concomitant treatment. In the abatacept trial, 76% to 82% of patients received MTX, 9% had hydroxychloroquine, 8.3% to 8.9% leflunomide and 9.8% sulfasalazine, according to the study arms. Leflunomide and sulfasalazine as biological cotherapies appear to have similar levels of effectiveness to MTX.26 On this basis, we felt we were able to compare the abatacept trial to the tocilizumab, golimumab and rituximab studies.
Table 4 lists the results of the indirect comparisons for ACR50 response rates at week 24. In patients with an inadequate response to anti-TNF, no significant difference was found when comparing rituximab to tocilizumab, rituximab to golimumab, abatacept to rituximab, abatacept to tocilizumab, golimumab to tocilizumab, rituximab or abatacept.
Indirect comparisons between biologicals in active rheumatoid arthritis (RA) with inadequate response to anti-tumour necrosis factor (TNF), in ORs for American College of Rheumatology 50% improvement (ACR50) response rate at 6 months (week 24)
Discussion
The multiplicity of biologicals currently available provides a strong rationale for comparing the benefit/risk of these agents in order to help rheumatologists to make rational therapeutic choices in the management of RA.
Our objectives were to compare the efficacy at 6 months (defined as the probability of achieving an ACR50 response) of several biologicals in two common situations in daily practice (i) when conventional DMARDs have failed (especially MTX) and (ii) when patients with RA experienced an IR to anti-TNF therapy. Using a systematic review of the literature and metaanalysis (Mantel–Haenszel and indirect comparison methods), we found that in MTX inadequate responders anti-TNFs appear to have a similar probability of achieving an ACR50 response in comparison to ‘non-anti-TNF biologicals’ all together (after excluding certolizumab trials). Separately, anti-TNFs would have a higher probability to achieve ACR50 than abatacept but not in comparison to rituximab or tocilizumab. A recent meta-analysis suggested that the ACR70 responses with tocilizumab may be better than that of other biologicals (anti-TNFs and abatacept) in IR-DMARD patients with RA, at 6 months. Nevertheless, for ACR50 responses no significant difference existed between tocilizumab and anti-TNFs or abatacept.27
After an inadequate response to anti-TNF, no differences were found between abatacept and tocilizumab, rituximab or golimumab.
Data for this analyses came exclusively from randomised, placebo controlled, double-blind trials in established RA, with similar baseline demographic and disease characteristics across studies. We chose the ACR50 response at as our outcome since this level of response appears more clinically relevant for agents of this price. But this choice also limits the conclusion to this outcome. Moreover we decided a priori to focus on outcome at 6 months, since most trials (11 of 18) did not report data at 1 year. Therefore, our results cannot be extrapolated to 1-year follow-up.
Although comparison of effectiveness between biologicals has been made possible by the common usage of composite indices such as the ACR and EULAR responses, comparisons of trials are becoming increasingly complex. Thus, the use of rescue arms with differences in (i) criteria to trigger the rescue phase, (ii) design of the rescue arm (ie, open label biological or standard of care) and (iii) timing of the rescue all may influence the results. Furthermore, response rates in IR-MTX patients and in IR-anti-TNF patients are quite different, with lower ACR50 and 70 responses in IR-anti-TNF patients even when adjusting the placebo. It is for this reason that IR-MTX and IR-anti-TNF patients have been analysed separately. Some trials (ie, DANCER) have mixed IR-MTX and IR-anti-TNF populations, which is why these two groups were analysed separately.
For IR-MTX, the indirect comparison of all anti-TNFs versus abatacept suggests that anti-TNFs are more effective than abatacept in IR-MTX patients (OR of an ACR50 response: 1.81 (95% CI 1.23 to 2.65)) at 6 months, which contradicts the results of the ATTEST trial that compared abatacept versus placebo and infliximab versus placebo.7 In this RCT, infliximab and abatacept had similar response rates at 6 months (ACR50 response rate with infliximab: 37% vs 40.4% with abatacept). However, in this RCT infliximab was given only at the lowest dose of 3 mg/kg every 8 weeks, which is suboptimal for a large proportion of patients and might have underestimated the potential response rates achievable with this agent.
Because the dose of 3 mg/kg appears suboptimal for a large proportion of patients in daily practice, we included patients who received from 3–10 mg/kg/8 weeks of infliximab in the ‘all anti-TNFs’ group. However, only 6% of patients (from the ATTRACT trial) received a maximum dose of 10 mg/kg/8 weeks of infliximab.8 Figure 1 shows similar ORs for the two groups, which makes it unlikely that this biases our results.
Substantial differences in study design (rescue arms) and patient characteristics resulted in heterogeneity between the anti-TNF trials (figure 1) and made such a comparison difficult on an individual basis. Thus, in the golimumab trial (GO-FORWARD), patients who displayed less then 20% of improvement from baseline on swollen and tender joints counts at week 16, had their study medications adjusted In the certolizumab trials (RAPID 1 and 2), patients who failed to achieved ACR20 response at week 12 or 14 were withdrawn from the study at week 16. The use of the ACR20 response as a rescue criterion in the certolizumab trials resulted in very large dropout in the placebo arm (63% to 79%) relative to the active agent (20% to 21%), which substantially enhances its apparent efficacy when adjusted for the placebo response. Furthermore, patients in these trials also have shorter disease duration and lower number of previous DMARDs, which could also explain some of the heterogeneity between anti-TNFs trials. We examined the impact of these study differences in sensitive analyses: The exclusion of the certolizumab trials from the ‘all anti-TNF’ group altered significantly the comparisons of the ‘all anti-TNF group’ with the other biological agents. We consider the result without the certolizumab trials a more rational comparison of the ‘all anti-TNF group’ and the other biological agents.
Analysis of IR-anti-TNF patients adds another level of complexity with differences in the number of anti-TNF failures and reason for failure. Several authors have demonstrated that the number of prior anti-TNF failures correlates inversely with the efficacy of an alternative anti-TNF and that patients failing for lack of efficacy generally respond less well than patients failing for adverse events. One limitation of our study was our inability to ascertain the reasons for anti-TNF failure and number of prior anti-TNF failures. Another caveat in comparing IR-TNF patients may be differences in dose or duration of the prior anti-TNF administration before considering an IR. The dose used is particularly important for infliximab. Another potential caution is the number of comparisons carried out for this analysis, which may favour spurious associations. However, all comparisons were planned a priori and the limited number of studies available did not allow us to correct for multiple comparisons.
The results of this meta-analysis suggest that in patients with RA with an IR-MTX, anti-TNFs may be more likely than certain non-anti-TNF biologicals to achieve an ACR50 response. However, in patients having experienced an IR to anti-TNF, no difference was found to achieve an ACR50 response between rituximab, abatacept, tocilizumab and golimumab. Head-tohead trials are clearly needed to confirm these results. The choice of a biological agent on a patient level also involves other factors, such as the patient's medical history, the medication's safety profile, personal preferences and the mode of administration. Doctors and patients need to consider these issues when choosing a new biological agent.
References
Supplementary materials
Web only data
Files in this Data Supplement:
Footnotes
-
Competing interests None declared.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Miscellaneous