Article Text

Abstract
Aim To monitor joint inflammation and destruction in rheumatoid arthritis (RA) patients receiving adalimumab/methotrexate combination therapy using MRI and ultrasonography. To assess the predictive value of MRI and ultrasonography for erosive progression on CT and compare MRI/ultrasonography/radiography for erosion detection/monitoring.
Methods Fifty-two erosive biological-naive RA patients were followed with repeated MRI/ultrasonography/radiography (0/6/12 months) and clinical/biochemical assessments during adalimumab/methotrexate combination therapy.
Results No overall erosion progression or repair was observed at 6 or 12 months (Wilcoxon; p>0.05), but erosion progressors and regressors were observed using the smallest detectable change cut-off. Scores of MRI synovitis, grey-scale synovitis (GSS) and power Doppler ultrasonography decreased after 6 and 12 months (p<0.05), as did DAS28, HAQ and tender and swollen joint counts (p<0.001). Patients with progression on CT had higher baseline MRI bone oedema scores. The RR for CT progression in bones with versus without baseline MRI bone oedema was 3.8 (95% CI 1.5 to 9.3) and time-integrated MRI bone oedema, power Doppler and GSS scores were higher in bones/joints with CT progression (Mann–Whitney; p<0.05). With CT as the reference method, sensitivities/specificities for erosion in metacarpophalangeal joints were 68%/92%, 44%/95% and 26%/98% for MRI, ultrasonography and radiography, respectively. Median intraobserver correlation coefficient was 0.95 (range 0.44–0.99).
Conclusion During adalimumab/methotrexate combination therapy, no overall erosive progression or repair occurred, whereas repair of individual erosions was documented on MRI, and MRI and ultrasonography synovitis decreased. Inflammation on MRI and ultrasonography, especially MRI bone oedema, was predictive for erosive progression on CT, at bone/joint level and MRI bone oedema also at patient level.
Statistics from Altmetric.com
Radiographic data from randomised placebo-controlled studies of rheumatoid arthritis (RA) patients show that erosive progression is arrested, and occasionally even reversed, when starting methotrexate and tumour necrosis factor alpha (TNFα) antagonist combination therapy.1,–,3
MRI is more sensitive than radiography for bone erosions, including erosive progression, and MRI enables visualisation of synovitis and bone oedema.4,–,7 Diminished size of MRI bone erosions during TNFα antagonist therapy was reported from a study of five RA patients,8 but no systematic MRI studies addressing the repair of erosions are available.
Ultrasonography is also more sensitive for bone erosions than radiography,5 9,–,12 but follow-up data are few.13,–,16 Ultrasonography allows the detection of synovial thickening by grey-scale ultrasonography (B-mode)5 17 and increased synovial blood flow using Doppler techniques.18,–,21
CT is considered a reference method for bone destructions, and is more sensitive for bone erosions than radiography, MRI and ultrasonography.12 22
No longitudinal RA studies comparing MRI, ultrasonography, CT and radiography exist. Combining these imaging modalities in one study of TNF antagonist-treated RA patients would allow an optimal assessment of joint inflammation (MRI and ultrasonography), bone erosion progression and repair (MRI, CT, ultrasonography and radiography) and, not least, the relation between inflammation and damage.
The primary purpose of the study was to monitor joint inflammation and destruction, using MRI and ultrasonography, in RA patients receiving adalimumab and methotrexate combination therapy, and to investigate whether MRI and ultrasonography findings have predictive value for erosive progression on CT. A secondary purpose was to compare the ability of MRI, ultrasonography, CT and radiography for erosion detection and monitoring.
Methods
Fifty-two RA patients, fulfilling the American College of Rheumatology criteria (ACR 1987),23 were included in this ethics committee-approved investigator-initiated study (clinicaltrials.gov NCT00696059). Inclusion criteria were: active RA with a disease activity score in 28 joints (DAS28) C-reactive protein (CRP) greater than 3.2 (DAS28(3)-CRP); indication for TNF antagonist therapy according to the treating rheumatologist; methotrexate treatment for 4 weeks or more before inclusion; no previous biological treatment and two or more low-grade erosions (Larsen grade 2–3) in the wrist of one hand or the metacarpophalangeal joints (index hand). Exclusion criteria were: treatment with other disease-modifying antirheumatic drugs (DMARD) than methotrexate; more than 10 mg/day of prednisolone, parenteral glucocorticoids or a change in dose of prednisolone 4 weeks or less before inclusion; or any medical conditions contraindicating TNF antagonist treatment. Adalimumab 40 mg subcutaneously every other week was added to previous methotrexate treatment. Tapering, but not increasing, methotrexate and prednisolone during the study was allowed.
Abbott Denmark provided financial support, but had no influence on, or involvement in, the planning or design of the study, data collection, data analysis or manuscript preparation.
Imaging and scoring methods
All imaging procedures were obtained before the first adalimumab injection and were repeated after 6 and 12 months of treatment. Radiography, CT and MRI were performed on the same day, whereas ultrasonography examinations were performed not more than 1 week apart. Images were read blinded to chronology, with assessors of radiographs (AB), CT (MØ), MRI (BE) and ultrasonography (UMD) unaware of other imaging and clinical data. Ten complete representative sets of images were re-evaluated to calculate intrareader intraclass correlation coefficients (ICC) on status scores and the smallest detectable change (SDC). Baseline imaging was used for comparing erosion detection on all modalities. As previously described,12 metacarpophalangeal joints 2–5 of the index hand were divided into quadrants, and the localisation of erosions were marked on score sheets.
MRI of the index wrist and metacarpophalangeal joints 2–5 was performed on a Philips Panorama 0.6T unit (Philips Medical Systems; Helsinki, Finland). High-resolution T1-weighted three-dimensional fast-field echo sequences were obtained separately of the wrist and metacarpophalangeal joints 2–5 for erosion assessment (repetition time 20 ms, echo time 8 ms, acquired slice thickness 0.8 mm (reconstructed at 0.4 mm), field of view 100 mm, matrix 216×216, averages 1). Synovitis was assessed on contrast-enhanced axial T1-weighted three-dimensional fast-field echo fat-saturated images (slice thickness 2 mm) and bone oedema on short tau inversion recovery images (slice thickness 3 mm).
High-resolution multidetector CT images (in-plane resolution 0.4 mm×0.4 mm, slice thickness 0.4 mm) of the index wrist and metacarpophalangeal joints 2–5 were obtained on a Philips Mx8000IDT unit (Philips Medical Systems, Cleveland, Ohio, USA).
For optimal comparison of erosions on MRI and CT at the three time points, standardised reconstruction of images was done. Images were scored according to definitions and principles of the outcome measures in rheumatology (OMERACT) RA MRI scoring method.24 25 CT was selected as the reference method for erosion detection and erosive progression both at the bone and patient level. For all metacarpophalangeal joint erosions on MRI and CT, estimates of erosion volume were obtained by measuring erosions using OsiriX medical imaging software (http://www.osirix-viewer.com). Measurements of erosions were performed twice on the same image set by the same person (UMD) with at least a 1-week interval, and the mean of the two measurements was used.
Ultrasonography examinations were performed using a General Electric LOGIQ9 unit (General Electric Medical Systems; Little Chalfont, Bucks, UK), equipped with a 14–9 MHz linear array transducer. Bilateral metacarpophalangeal joints 1–5 and wrists were examined with longitudinal and transversal scans. Images of all joints were stored and scored for erosions (metacarpophalangeal joints only), grey-scale synovitis (GSS) and power Doppler signal (PDS) as suggested by Szkudlarek et al.26
Radiographs (resolution 0.143 mm) of hands (posterior–anterior) and feet (anterior–posterior) were obtained on a Philips Digital Diagnost unit (Philips Medical Systems, Hamburg, Germany). Images were evaluated according to the Sharp/van der Heijde method.27 The Sharp/van der Heijde erosion scores were used for the analysis of the proportion of patients with a change in destruction at 12 months.
Clinical assessment
Clinical assessments, performed at baseline and weeks 2, 6, 12, 26, 39 and 52, included 28-joint count for swelling and tenderness, health assessment questionnaire (HAQ) and CRP. Clinical data were entered into case report forms and the Danish DANBIO registry.28 Disease activity was assessed by the DAS28 (DAS28(3)-CRP) and response rates by the ACR20/ACR50/ACR70 and the European League Against Rheumatism (EULAR) (none/moderate/good) response criteria.
Statistics
Baseline observations and change scores at follow-up are reported with descriptive statistics. Change from baseline to 12 months on the group level was tested using the Wilcoxon signed rank test, with p<0.05 considered significant. The SDC was calculated as suggested by Bruynesteyn et al,29 and expressed as a percentage of the highest obtained score (SDC%). On the patient level, a definite change was defined as a change score above the SDC cut-off. For predicting erosive progression on CT in individual joints/bones, Fisher's exact test and RR were calculated, whereas differences in time integrated values (area under the curve; AUC) were tested using the Mann–Whitney test. With CT as the reference method for erosion detection in the metacarpophalangeal joints, sensitivities, specificities, accuracies and κ values of MRI, ultrasonography and radiography were calculated. SPSS version 15.0 was used.
Results
Fifty-two RA patients were included (67% women, 79% IgM rheumatoid factor positive, median age 61 years (IQR 50–70), disease duration 7 years (3–13), number of previous DMARD two (one to three), methotrexate dose 19 mg/weekly (13–25); 29% received concomitant prednisolone). Sixteen patients were excluded before 12 months, due to lack of efficacy (n=5), adverse events (n=6), protocol violations (n=5).
Clinical efficacy
The DAS28 was significantly reduced at 6 and 12 months compared with baseline (median 2.9 and 2.5, respectively, vs 4.7 at baseline (Wilcoxon; p<0.001)), as were the number of tender and swollen joints, CRP and HAQ score (table 1).
Baseline values and change scores in clinical and imaging parameters
Clinical response rates at 12 months (with non-completers considered as non-responders) were ACR20 54%, ACR50 40%, ACR70 33%, EULAR good response 46% and DAS remission (DAS28 <2.6) 38%.
Imaging changes
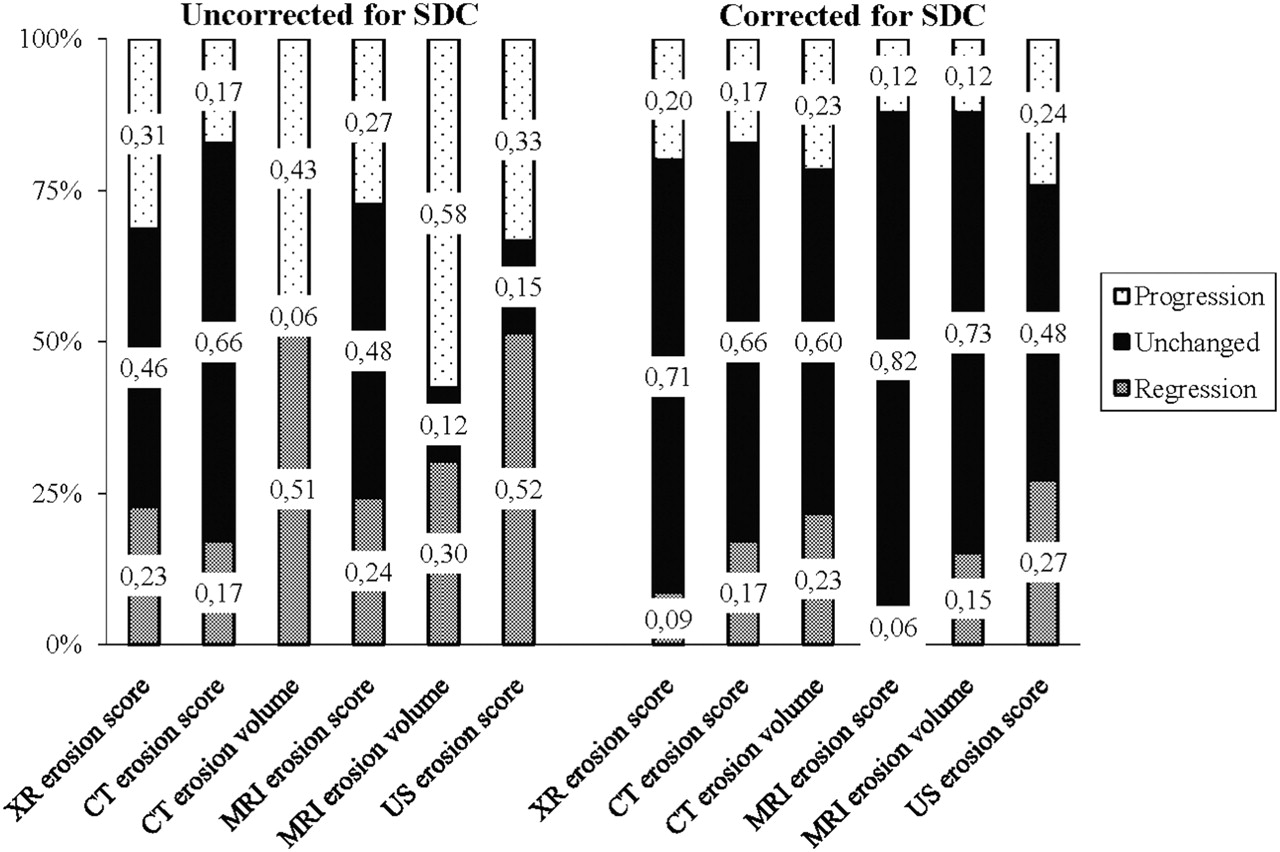
Not all patients completed all imaging modalities, making direct comparison between imaging modalities difficult. No statistically significant overall changes in bone destruction, compared with baseline, were observed on MRI or ultrasonography (table 1). However, at the patient level both progression and regression in erosion scores and volumes were seen, and in a minority of patients the observed changes exceeded the SDC (figure 1). Statistically significant decreases in scores of MRI synovitis, GSS and PDS and a numerical decrease in MRI bone oedema, were observed at 6 and 12 months (table 1). In all patients, at least one joint had synovitis on MRI and GSS at 12 months, whereas bone oedema and PDS were registered in 63% and 87% of patients, respectively. Also, at 12 months MRI synovitis was registered in 95% of joints, MRI bone oedema in 20% of bones, whereas on ultrasonography GSS and PDS were registered in 45% and 26% of joints, respectively.

Proportion of patients with regression, progression or unchanged erosion scores/volumes at 12 months on radiography (XR), CT, MRI and ultrasonography (US) before and after correction for the smallest detectable change (SDC).
Prediction of erosive progression
Patients with definite erosive progression at 12 months on CT (positive erosion change >SDC) had significantly higher baseline MRI bone oedema scores than non-progressors (Mann–Whitney p<0.05). When baseline MRI bone oedema was present, compared with not present, RR for erosive progression in the same bone on CT at 12 months was 3.8 (95% CI 1.5 to 9.3, p=0.004), whereas if bone oedema was ‘ever present’ versus ‘never present’ the RR was 14.8 (4.3 to 50.7; p<0.0001). Higher levels of time integrated (AUC) scores of MRI bone oedema, PDS and GSS were found in bones/joints with progression on CT compared with bones/joints without (Mann–Whitney p<0.05; table 2).
Relations between inflammation on MRI and ultrasonography and subsequent erosive progression on CT at the bone level (MRI bone oedema) and joint level (MRI synovitis, ultrasonography power Doppler, ultrasonography grey scale synovitis) at 12 months
MRI bone oedema was registered at some time (0, 6 and/or 12 months) in 25% of all bones, whereas in 15 out of 18 (83%) bones with CT progression and in two out of 12 (17%) bones with CT regression. PDS was seen in 43% of all joints, but in six out of six (100%) joints with CT progression and in four out of seven (57%) joints with CT regression.
Reliability and agreement
The median intraobserver ICC for erosion status scores at the three time points was 0.91 (0.44–0.98) for MRI, 0.93 (0.89–0.99) for ultrasonography and 0.96 (0.96–0.97) for CT (table 3).
Intrareader ICC and SDC for MRI, ultrasonography and CT
From baseline imaging, 800 (patients n=50) metacarpophalangeal joint quadrants on MRI, 784 (n=49) on ultrasonography and 832 (n=52) on radiography were compared with corresponding CT for the presence of erosions. With CT as the reference method, the overall sensitivity, specificity and accuracy for erosion detection were 68%, 92% and 84%, respectively, on MRI, 44%, 95% and 84% on ultrasonography, and 26%, 98% and 73% on radiography. Highest sensitivities were obtained at the metacarpal heads (MRI 91%, ultrasonography 58% and radiography 34%). Overall κ values were 0.63, 0.44 and 0.29 for MRI, ultrasonography and radiography, respectively, with the highest agreements in the metacarpal heads.
Of 29 patients in whom all modalities were complete, agreement of three or four modalities for the direction of change was observed in 16 patients before and in 24 patients after correcting the change score for the SDC (calculated for metacarpophalangeal joints 2–5).
Discussion
This is the first longitudinal study systematically following RA patients with repeated MRI, ultrasonography, CT and radiographic examinations.
The primary focus of this report was the assessment of structural joint damage on MRI and ultrasonography in a longitudinal setting during TNF antagonist and methotrexate combination therapy. We observed no statistically significant change in MRI or ultrasonography erosion scores or MRI erosion volume at 6 or 12 months. The majority of patients had negative or unchanged erosion scores, strongly suggesting that the erosive progression was arrested. In a minority of patients (6% on MRI and 24% on ultrasonography) the negative change score exceeding the SDC and repair of erosions was observed (figures 1 and 2). These MRI and ultrasonography findings are in agreement with CT and radiographic data from this cohort, and support that the repair of erosions in RA during TNF antagonist therapy occurs, but is rare.30

{kind=link}
{kind=link}
MRI and ultrasonography of the second metacarpophalangeal joint of a patient with rheumatoid arthritis (RA) before (A and D), and after 6 months (B and E) and 12 months (C and F) of adalimumab and methotrexate combination therapy. T1-weighted magnetic resonance images in coronal (A–C) and transversal (A′-C′) plane, and corresponding grey-scale ultrasonography in longitudinal (D–F) and transversal (D′–F′) plane. The erosion at the radial side was detected on both MRI and ultrasonography, and the size of the erosion has decreased on MRI at 6 and 12 months follow-up compared with baseline. The outcome measures in rheumatology (OMERACT) MRI erosion score decreased from grade 3 at baseline to grade 2 at 6 and 12 months, whereas the ultrasonography erosion score was 3 at all examinations. The decreased OMERACT MRI erosion size was also documented on CT, and by erosion volume measurements (not shown). Post-contrast MRI (A″–C″) and power Doppler ultrasonography (D″–F″) show a decrease in MRI synovitis and power Doppler signal at follow-up examinations, however, some MRI synovitis persists.
Significantly decreased scores of MRI and ultrasonography synovitis at 6 and 12 months were found. However, all patients had remaining synovitis on MRI and/or ultrasonography even at 12 months, eg, MRI synovitis in 95% and PDS in 26% of the assessed joint areas. The decreased sign of inflammation on MRI and ultrasonography during TNF antagonist therapy is in agreement with previous smaller studies.31,–,37
The ability of ultrasonography and MRI to detect subclinical synovitis, and that these findings have predictive value for subsequent radiographic progression have been demonstrated in RA patients treated with DMARD.38 39 Whereas baseline scores of synovitis on ultrasonography have been related to radiographic progression in placebo/conventional DMARD-treated patients,36 39 this was neither the case in the present study nor in earlier cohorts of TNF antagonist-treated patients36 40 This, in combination with the fact that the majority of patients showed sustained imaging signs of joint inflammation, suggests that TNF antagonist therapy suppresses bone erosion development, not only by the suppression of inflammation but also through an additional pathway.
The RR for erosive progression at the bone level on CT was statistically significantly increased both if bone oedema was present at baseline and if present at any time (RR 3.8 and RR 14.8, respectively). Bone oedema on MRI has been documented to represent an inflammatory infiltrate in the bone marrow (osteitis),41 42 and whereas a strong relationship between MRI bone oedema and erosive progression on MRI and radiography has been established,43,–,49 this is the first time MRI bone oedema has been related to erosive progression on CT. The weaker relationship between baseline MRI bone oedema and erosive progression found in this study may be explained by the very limited erosive progression in these TNF antagonist-treated patients, compared with patients treated with non-biological agents.43,–,48
On ultrasonography, a greater proportion of patients had a change in erosion score exceeding the SDC compared with other imaging modalities (figure 1). However, in this study the SDC on ultrasonography only measured the variability in reading the acquired images, and not the variability caused by differences in image acquisition. Based on this study, one cannot conclude that ultrasonography is more sensitive to change for erosions than MRI, CT or radiography. However, overall the study supports the potential of ultrasonography for the assessment of erosive progression, and the available longitudinal studies also suggest a greater sensitivity to change of ultrasonography than radiography.13 16 Previous follow-up studies did not take the reproducibility, eg, the SDC of the erosion assessment, into account when reporting the numbers of patients with progression. More data, particularly on reproducibility and sensitivity to change, are needed to establish the relative value of ultrasonography, compared with other imaging modalities, for detecting erosive progression. Higher PDS and GSS scores and the more frequent occurrence of PDS and GSS at baseline was detected in joints with CT progression compared with joints without.
The sensitivity, specificity and accuracy of radiography, MRI and ultrasonography obtained in the present study were very similar to findings in a previous smaller study.12 Compared with CT, high specificities for bone erosions were found with all three modalities, whereas a poor sensitivity of radiography and moderate sensitivities of MRI and ultrasonography were found. This proves that CT is very sensitive for detecting bone erosions, and suggests that CT may be useful for joint damage assessment in RA. However, CT is disfavoured by the use of ionising radiation and its inability to visualise soft tissues. The sensitivity for erosion detection by an experienced ultrasonographer was lower than on MRI, but higher than on radiography. In agreement with other studies, the highest sensitivities were found at metacarpophalangeal joints 2 and 5, being the most accessible joints to ultrasonography examination.5 10 12
The direction of change in erosion score at 12 months on four different imaging modalities was investigated. As the scoring systems used include a different number of joints and joint regions, we chose to compare metacarpophalangeal joints 2–5 only. Agreement of at least three imaging modalities was observed in 16 and 24 out of 29 patients before and after correcting for the SDC, respectively. It should be noted that only minimal changes occurred, making agreement much more liable to reader variation, than if many patients had shown extensive progression.
It should be emphasised that we prioritised high-resolution pre-contrast T1-weighted images with low slice thickness for assessment of erosion, whereas a fast contrast-enhanced axial fat-saturated sequence was used for assessing synovitis. This sequence provided a suboptimal difference between pre and post-contrast images, and thereby potentially suboptimal assessment of synovitis;however, a significant decrease in MRI synovitis was still observed. Furthermore, the study would have benefited from more patients, and only two-thirds of patients completed the study. However, this is to our knowledge the largest follow-up study comparing multiple imaging modalities in a RA cohort treated with a biological agent.
In summary, during adalimumab and methotrexate combination therapy, signs of synovitis on MRI and ultrasonography significantly decreased. No statistically significant overall change in structural joint damage was observed, but repair of individual erosions was documented on MRI. Imaging signs of inflammation on MRI and ultrasonography, especially MRI bone oedema, was predictive of subsequent erosive progression on CT, both at the individual bone/joint level and also for MRI bone oedema at the patient level.
Therefore, our data strongly support that erosive progression is arrested in RA patients treated with adalimumab and methotrexate combination therapy. Moreover, the study supports the idea of a partial uncoupling of inflammation and destruction. Finally, these data emphasise the predictive value of modern imaging, and especially highlight the importance of MRI bone oedema for predicting erosive progression.
References
Footnotes
See Editorial pg. 241.
-
Funding Funding was provided by Abbott Denmark, the Danish Rheumatism Association and the Aase and Ejner Danielsen Foundation. Abbott Denmark had no influence on, or involvement in, the planning or design of the study, data collection, data analysis or manuscript preparation.
-
Competing interests MLH has received consulting fees, speaking fees or research grants from Abbott, Centocor, Roche, Schering-Plough, UCB-Nordic and Wyeth, and she has received grants from Abbott, Bristol-Myers Squibb, Roche, Schering-Plough, UCB-Nordic and Wyeth on behalf of DANBIO. MSH has received consulting fees, speaking fees and/or research grants from Bristol-Myers Squibb, Roche, Schering-Plough and Wyeth. AH has received consulting fees, speaking fees or research grants from Abbott and Schering-Plough. MØ has received consulting fees, speaking fees or research grants from Abbott, Amgen, Bristol-Myers Squibb, Centocor, Genmab, Glaxo-Smith-Kline, Novo, Pfizer, Roche, Schering-Plough, UCB and Wyeth.
-
Ethics approval This study was conducted with the approval of the local ethics committee, Copenhagen, Denmark.
-
Provenance and peer review Not commissioned; externally peer reviewed.