Article Text

Abstract
From birth, humans coexist and coevolve with trillions of micro-organisms inhabiting most body surfaces and cavities, referred to as the human microbiome. Advances in sequencing technologies and computational methods have propelled the exploration of the microbiome’s contribution to human health and disease, spearheaded by massive efforts such as the Human Microbiome Project and the Europe-based MetaHit Consortium. Yet, despite the accumulated body of literature and a growing awareness among patients, microbiome research in rheumatology has not had a key impact on clinical practice. Herein, we describe some of the landmark microbiome studies in autoimmunity and rheumatology, the challenges and opportunities of microbiome research and how to navigate them, advances in related fields that have overcome these pitfalls, and future directions of harnessing the microbiome for diagnostic and therapeutic purposes.
- autoimmune diseases
- microbiome
- methods
- study design
- best practices
Statistics from Altmetric.com
Introduction
Humans have coevolved with and harbour trillions of microbes from the time they are born. This collection of symbiotic, commensal and pathogenic micro-organisms (and their genomes) found on the skin, mucosal surfaces and other organs is referred to as the human microbiome, a term coined by the Nobel laureate, Joshua Lederberg (figure 1).1 Although mostly resilient during the adult life, the composition of the microbiome can be influenced by numerous factors, including genes, age, sex, mode of delivery, nursing, diet, drugs (prescription and non-prescription), and pets, to name a few.2 3 Previously, the ability to define these microbial communities was limited to classic culturing techniques, which were able to isolate up to 20% of the microbes known today.4 This situation dramatically changed with the democratisation of next-generation sequencing technologies, which allowed for a higher proportion of organisms to be identified, including bacteria, fungi and viruses.

{kind=link}
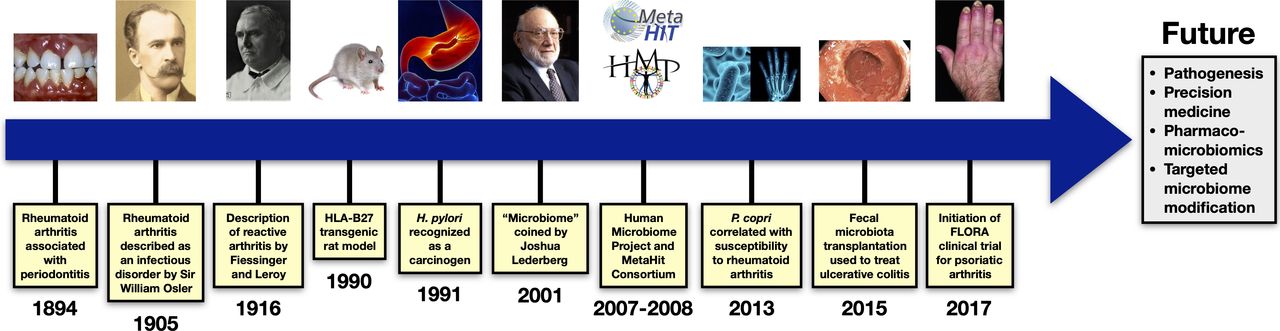
Historical time line of key events in microbiome research in rheumatology. Photo acknowledgements: 1894: https://www.efp.org/patients/what-is-periodontitis.html; 1905: https://www.acponline.org/about-acp/about-internal-medicine/sir-william-osler-and-internal-medicine; 1916: https://fr.wikipedia.org/wiki/No%C3%ABl_Fiessinger; 1990: https://www.dreamstime.com/stock-photos-grey-rat-isolated-white-image30500173; 1991: https://www.medicinenet.com/helicobacter_pylori/article.htm; 2001: https://www.nationalmedals.org/laureates/joshua-lederberg; 2007–2008: http://gutcyc.org/aboutGutCyc; 2013: https://www.theatlantic.com/health/archive/2015/01/joint-pain-from-the-gut/383772/; 2015: https://www.gponline.com/clinical-review-ulcerative-colitis-epidemiology-diagnosis-management/gi-inflammatory-bowel-disease/ulcerative-colitis/article/1293409; 2017: https://www.merckmanuals.com/home/bone,-joint,-and-muscle-disorders/joint-disorders/psoriatic-arthritis.
Through the use of these technologies and advanced computational analytics, we are now able to obtain an enormous amount of sequence data in each run, and have an efficient way of profiling microbial communities from different sources. The typical workflow involves obtaining samples of interest, isolating DNA from these samples and performing DNA sequencing of microbial taxa. This is done by either querying a marker gene, such as 16S rRNA for bacteria or internal transcribed spacer (ITS) for fungi, or looking at the DNA in its entirety via shotgun metagenomic sequencing, which allows for the characterisation of gene families and pathways.3 With the development of more sophisticated modalities, we now have the ability to profile gene expression (metatranscriptomics), proteins (metaproteomics) and metabolites (metabolomics) collectively produced by the microbiota.5 6
In 2007 the National Institutes of Health (NIH) launched the landmark Human Microbiome Project (HMP),7 which was followed by the Europe-based MetaHit Consortium,8 two massive multicentre efforts that have propelled research on how microbes contribute to human health and disease (figure 1). In fact, this work revealed that the microbiome also plays a prominent role in autoimmune disease, as evidenced by the exponential growth of studies in virtually all realms of rheumatology over the last few years.9 Still, despite the extent and wealth of information that such a body of literature has yielded, microbiome research is yet to have a significant influence on clinical practice (eg, enabling drug discovery or patient stratification).10 In fact, some of the results have been correlative in nature, hampering their translation into the clinical setting. However, due to its popularity, discussion of the microbiome has percolated into conversations with patients, and in some cases has resulted in dietary and behavioural modifications. Here, we describe the advances in rheumatology, enumerate the type of research that should be pursued and what should generally be avoided, review how other disciplines have overcome these challenges, and look into the microbiome-based diagnostic and therapeutic pipeline.
What is known about the microbiome in autoimmune diseases
Numerous studies of animal models and humans have demonstrated a link between the microbiome and autoimmunity. For instance, a wide range of animal models for inflammatory arthritis remain healthy when raised under germ-free conditions, only developing their respective phenotypes when exposed to particular microbes. Examples include the HLA-B27 transgenic rat,11 the interleukin (IL) 1 receptor antagonist knockout (IL1rn−/−) mouse,12 the K/BxN T cell receptor transgenic mouse (which expresses the KRN T cell receptor transgene and the MHC class II molecule Ag7)13 and the SKG mouse (which has a mutation in the Src homology 2 domain of zeta-chain-associated protein kinase 70 [ZAP-70]).14 These data have confirmed and validated the fact that intestinal microbiota are indeed required to trigger and drive systemic autoimmunity.
Similarly, studies of human autoimmune disease consistently characterise a state of microbial dysbiosis, a disruption in the homoeostasis of microbial communities and composition.15 Perhaps the most established connection is in rheumatoid arthritis (RA), where microbes were identified as potential contributors to disease as early as the 19th century. Sir William Osler attributed RA to tuberculosis,16 the toxaemic factor theory proposed that gut micro-organisms produced substances responsible for joint inflammation,17 and a connection between RA and periodontitis (PD) was established as early as 1894 (figure 1).18 More recently, Porphyromonas gingivalis, an oral anaerobe involved in the development of PD, was found to be highly prevalent in patients with RA,19demonstrating positive serological correlation with anticitrullinated peptide antibody titres,20 21 considered to be triggers for RA. Interestingly, peptidylarginine deaminase 4, an enzyme that catalyses citrullination, has also been identified as a contributor to RA pathogenesis.22–25 Distinct microbial perturbations exist in the gut as well, with expansion of Prevotella copri in untreated patients with new-onset RA,26a microbe that can induce an intestinal Th17 response leading to severe arthritis in SKG mice (figure 1).27 Evidence for P. copri involvement in pathogenesis derives from the identification of reactivity against a P. copri peptide in human RA and an associated Th1 response,28 providing a plausible mechanistic link.
The gut-joint axis is likewise involved in several conditions under the spondyloarthritis (SpA) umbrella classification. In the HLA-B27 transgenic rat model of SpA there is a marked intestinal dysbiosis,29 30 which is linked to enhanced expression of Th1 and Th17 cytokines, expansion of Th17 cells in the colonic mucosa, and increased production of bacteria-specific IgA.30 These perturbations are highly dependent on host genetic background.31 In humans, the most obvious examples of the gut-joint connection are reactive arthritis, described in 1916 by Noël Fiessinger and Emile Leroy,32 which results after infection by enteropathogenic (and uropathogenic) bacteria,33 and enteropathic arthritis, described in 1929 by J Arnold Bargen,34 which is a sequala of inflammatory bowel disease (IBD) and can parallel colitis exacerbations (figure 1).35 Another example is ankylosing spondylitis, where terminal ileal biopsies demonstrate distinct microbial signatures driven by several core families of bacteria.36 In paediatric enthesitis-related arthritis, a type of juvenile SpA, there is reduction of intestinal Faecalibacterium prausnitzii (similar to IBD),37 a gut commensal that produces the short-chain fatty acid (SCFA) butyrate,38 which is known to promote the expansion of T-regulatory cells.39 In psoriatic arthritis (PsA), our group has demonstrated a significant reduction of two gut commensals, Akkermansia and Ruminococcus, correlating with higher levels of intestinal secretory IgA and lower levels of receptor activator of nuclear factor κ-B ligand, as well as reduction of local anti-inflammatory medium-chain fatty acids (MCFAs), hexanoate and heptanoate.40
Systemic lupus erythematosus (SLE) is also characterised by microbial perturbations. One of the earliest investigations showed decreased gut bacterial diversity and a lower Firmicutes:Bacteroidetes ratio in patients with SLE.41 Other relatively small studies have also demonstrated gut bacterial dysbiosis in SLE,42–48 mostly corroborating previous findings. Intriguingly, similar to RA, translocation of intestinal pathobionts was likewise noted with the description of Enterococcus gallinarum in liver biopsies of patients with SLE.49 Furthermore, new evidence in mice and humans suggests that translocation of commensal orthologs of a human autoantigen, such as Ro60, can drive autoimmunity and may be a factor in SLE pathogenesis.50
There is far less evidence for microbiome involvement in systemic sclerosis. The majority of research to date has characterised gut microbial communities in those with and without disease,51–55 focusing on the dysbiosis in patients with gastrointestinal features of systemic sclerosis. Many of the studies found decreased gut bacterial diversity and lower levels of ‘anti-inflammatory’ microbiota such as Bacteroides, Faecalibacterium and Clostridium, as well as higher levels of pathobionts such as Fusobacterium.52–55
Navigating and addressing challenges in microbiome research
As discussed, although murine work has established a definite role for microbiome contribution to rheumatological conditions, the majority of human studies have been correlative in nature and therefore unable to distinguish whether dysbiosis precedes disease onset or is rather a consequence of the inflammatory process. Furthermore, very few studies propose a mechanism for pathogenesis. In general, microbiome experiments require thoughtful and thorough planning in order to generate data that are robust and reproducible, enabling their applicability in the clinic (table 1). Starting with experimental design, in lieu of performing exploratory correlative studies, the field should aim to answer particular questions that will preferably have a direct impact on patient care. In planning a microbiome experiment, it is also critical to select the appropriate control population and account for factors that may influence or confound the data, including host genes,56 57 age58 59 and sex,60 as well as environmental variables such as diet61 and drugs (even those without antibiotic or antimicrobial properties).62 In animal experiments, cage effects63 and facilities64 have a significant influence on the data and should be treated as separate variables of interest. Due to potential fluctuations in the microbiome, possibly related to disease flare/activity65 66 and/or treatment,67 characterising the microbiome in a longitudinal fashion is of utmost importance (instead of assessing a single cross-sectional time point). Most importantly, many microbiome experiments are performed on small cohorts, leading to conclusions that are based on statistically invalid methodology. It is therefore critical to estimate adequate sample sizes a priori in order to sufficiently power these studies for the identification of biologically relevant patterns. This may be challenging given the lack of consensus on appropriate power analyses for microbiome studies. Nevertheless, several approaches have been proposed based on the detection of differences in α/β diversity and taxa relative abundance.68 Furthermore, the need to incorporate confounding variables typically necessitates larger sample sizes, which may be difficult to achieve, particularly in the case of the rarest conditions in rheumatology. An effective way to overcome this hurdle is through multicentre study designs and data sharing.
Dos and don’ts in microbiome research
Once collected, samples should ideally be stored in a consistent fashion, processed at the same time with identical reagents and kits, and sequenced in single runs to avoid batch effect. The HMP Manual of Procedures provides detailed protocols for performing these steps.69 Positive and negative controls should always be used with every sequencing run. Low biomass samples, such as those derived from skin surface and lung fluid, present an extra challenge as they are prone to contamination from reagents and sensitive to sequencing conditions, thus requiring careful handling and the use of dedicated instruments.3 Postsequencing, certain software packages and computational methods may be employed to decrease background noise in low biomass data. In the analysis phase, comparisons are typically made across hundreds of identified taxa so multiple hypothesis testing must be accounted for by using statistical methods such as false discovery rate or Bonferroni corrections.70 71 Once results are obtained and published, the raw sequence data (including controls), a description of the detailed analyses, as well as any code written to generate results should be made publicly available through repositories such as the Sequence Read Archive,72 the European Nucleotide Archive73 and GitHub.74 This allows for cross-validation and incorporation of data in future studies. Unused samples should also be stored to answer future questions that originate from current research efforts.
To produce more meaningful generalisable outcomes, it is essential to collaborate with an interdisciplinary team that can address questions of biological/clinical relevance, computational complexity and appropriate statistical models. Moreover, simply using DNA sequencing to look at the presence of taxa in certain conditions is now considered outdated and rather rudimentary. Cost permitting, the field should instead aim to design studies that explore the entire milieu of microbes (including bacteria, fungi and viruses, acknowledging recognised limitations such as the underdevelopment of comprehensive high-resolution reference databases for fungal and viral micro-organisms), microbe-microbe interactions, metabolites produced by microbes, and the effect that they have on the host immune and metabolic system. This requires a multipronged approach that applies shotgun and other multiomic sequencing platforms combined with more sophisticated computational analyses. Finally, generated results should be validated and reproduced in separate cohorts and backed preferentially by in vitro, ex vivo and in vivo data to look for recognisable patterns in order to enable a mechanistic understanding of the inflammatory process.
Advances in microbiome research
Despite these challenges, there have been pivotal advances in the oncology75 and IBD disciplines,76 where microbiome research has taken a more mechanistic approach beyond correlative descriptions. In fact, the gut microbiome is increasingly recognised for its influence on cancer and response to cancer therapy.77 78 For example, there are data supporting the notion that recurrent antibiotic use may be associated with the development of malignancies in various organs.79 However, the majority of studies that demonstrate a more causal role for the microbiome, aside from Helicobacter pylori-associated gastric cancer,80 are in colorectal cancer (CRC). First, microbial composition in tumor-affected tissue is distinct from that of adjacent healthy mucosa.81 82 Second, and even more striking is that transplanting stool from patients with CRC can cause the formation of polyps, increase levels of intestinal dysplasia and alter the local immune environment in animal models.83 Moreover, specific bacteria have been shown to directly stimulate inflammation and promote carcinogenesis, including enterotoxigenic Bacteroides fragilis 84 and Fusobacterium nucleatum.85 The intestinal microbiota are also key drivers for patient response to therapy, as exemplified by immune checkpoint inhibitors used in the treatment of melanoma,86–88 where distinct differences exist between responders and non-responders that can be recapitulated in germ-free or antibiotic-treated animal models using faecal microbiota transplantation (FMT) from patients.89
In IBD, which includes Crohn’s disease (CD) and ulcerative colitis (UC), gut microbial dysbiosis is apparent in both the reduction of important gut commensals and the expansion of pathogens. For example, a reduction of F. prausnitzii, an important producer of the SCFA butyrate (discussed earlier) is well documented in both CD90 and UC.91 Although specific bacterial pathobionts have not been consistently identified, there are indications of certain microbiota driving inflammation,92 as well as an increased prevalence of Enterobacteriaceae such as invasive Escherichia coli.93 Several studies highlight the role of fungi, including the expansion of Candida albicans,94 95 an immunogen for anti-Saccharomyces cerevisiae antibodies, which serve as serological markers in IBD.96 Even the virome has been implicated with the expansion of Caudovirales bacteriophages in patients with IBD.97 Furthermore, due to its dynamic nature, one study looked at the longitudinal composition of the gut microbiome, demonstrating that microbial communities in IBD exhibit more fluctuations compared with healthy individuals.98 Another study profiled and correlated the gut metagenomes and metatranscriptomes over a 1 year period, showing species-specific biases in transcriptional activity with a predominance of F. prausnitzii-associated pathways that were disproportionate to F. prausnitzii abudnance.99 A number of investigations have also looked at adaptive immune responses to microbial agents and have shown that patients with IBD produce large amounts of IgG antibodies100 and CD4+ T-lymphocytes with altered IL-17A production101 directed against symbiotic bacteria.
IBD investigators have led the way in FMT research, which gained widespread interest after its success in treating refractory Clostridioides difficile (previously named Clostridium difficile) infections.102 103 FMT involves the transfer of minimally manipulated prescreened stool from a donor to the gastrointestinal tract of a recipient via a nasogastric tube, colonoscopy, retention enema or capsule, with the aim of reversing a dysbiotic state and restoring beneficial microbiota.104 Four randomised controlled trials have been published looking at the efficacy of FMT in UC,105–108 showing an overall remission rate of 37%, which was twofold higher than patients receiving placebo,109 and equivalent to outcomes with biological therapies (figure 1).110 To date, there have not been any randomised controlled trials of FMT use in CD, although a recent meta-analysis reports an overall rate of clinical remission,111 a finding that may be less interpretable given the heterogeneity of patient disease activity and FMT protocols.104
What the future holds: pharmacomicrobiomics and microbiome-modulating strategies in rheumatology
The field of rheumatology has also made advances with the potential to significantly impact the care of our patients. One example is the growing field of pharmacomicrobiomics, which describes the effects that microbial variations have on the action and toxicity of drugs (and vice versa).112 For instance, we know that the activation of sulfasalazine, a disease-modifying antirheumatic drug used to treat inflammatory arthritis and UC, is dependent on the enzymatic cleavage by gut microbes.113 This appears to also hold true for methotrexate, which is known to be metabolised by the gut microbiome in mice114 115 and humans,116 and may have off-target, antibiotic effects.117 In axial SpA, patients who respond to anti-TNF inhibitors exhibit a more resilient pretreatment gut microbiome,118 while IL-17A inhibitors are associated with expansion of intestinal C. albicans in a subgroup of paients with SpA/PsA,67 as well as an increased risk for the development of candidiasis.119 120 Further progress in pharmacomicrobiomics will lead towards personalised therapeutic approaches that are based on patient microbiome features, allowing for improved selection of medications with the highest efficacy and lowest risk for toxicity.121
Another promising area of active research is the study of targeted modulation of the microbiome to improve disease outcomes, with the caveat that for most conditions, it is not yet clear whether microbial changes contribute to disease pathogenesis or stem from the disease process itself. One indirect way to modulate the microbiome is through diet, which can globally shape the microbial community composition. Few conclusive studies exist on the topic but some trials looking at the Mediterranean diet have demonstrated beneficial effects in RA.122 123 In PsA, which is strongly associated with obesity and metabolic syndrome, weight loss has also led to significant improvements in disease outcomes.124 125 Another strategy relies on the use of prebiotics, compounds that promote the growth of advantageous microbes (ie, SCFAs and MCFAs), and probiotics, compounds that contain presumed beneficial living organisms. Prebiotics have demonstrated value in an animal model of SpA,126 while probiotics containing Lactobacillus have been associated with improvements in RA disease activity scores.127–129 As discussed, a more invasive approach that has yielded encouraging results is FMT, which directly modifies microbial communities and their metabolites, and may directly or indirectly stimulate the host immune response. No conclusive evidence exists in rheumatic disease as of yet, but this is currently being studied in PsA by the Danish-sponsored Efficacy and Safety of Fecal Microbiota Transplantation in Peripheral Psoriatic Arthritis clinical trial (figure 1).130 However, it is important to recognise that FMT has several important limitations. For instance, we do not know the best route of delivery (oral vs rectal) or the frequency of FMT needed to achieve durable responses. Likewise, we have not identified specific beneficial taxa that can reliably attenuate various autoimmune conditions, and it appears that previous successes in IBD may have been driven by ‘super-donors’ (ie, donors whose stool samples achieved successful outcomes).131 Extensive donor testing is also required to guarantee safety as recent reports have indicated transmission of drug-resistant organisms from donors to recipients.132 133 Aside from FMT, other potential strategies, which are being extensively tested by the pharmaceutical industry but are yet to be Food and Drug Administration approved, are microbial consortia or microbially derived bioactive compounds for the treatment of infectious and autoimmune diseases.134
Conclusions
Microbiome research in rheumatology is expanding significantly, offering unique opportunities to better understand aspects of autoimmune disease pathogenesis, the potential for patient stratification and its application towards personalised therapeutic strategies. However, in order to achieve its full potential, there is a need to further adapt state-of-the-art microbiome-related methods and technologies in our discipline. It is imperative to continue the quest for biologically relevant inquiries, addressing causality and designing studies that are important to patient care. The expansion of collaborations and data sharing is also critical to increase the sample size of our cohorts and apply the appropriate expertise. It is equally important to broaden the scope of these studies to look at the global network of organisms, their interactions and what they produce, so we can move beyond simplistic taxonomic classification work. Finally, the validation of microbiome-derived data should ensure meaningful results that could potentially serve in diagnostics and therapeutics, aiding in the development of precision medicine approaches to optimise health outcomes in rheumatic and autoimmune diseases.
References
Footnotes
Handling editor Josef S Smolen
Contributors All authors have contributed to the conception of the work, drafting and revising the work, and final approval of the version to be published.
Funding JUS is funded by NIH/NIAMS R01AR074500, the National Psoriasis Foundation, the Colton Center for Autoimmunity, the Riley Family Foundation and the Snyder Family Foundation.
Competing interests JUS has been granted USPTO patent no. 10011883 ('Causative agents and diagnostic methods relating to rheumatoid arthritis'). JUS has consulted for UCB, Janssen, Novartis and Pfizer.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.