Article Text

Abstract
Objective To update the European League Against Rheumatism (EULAR) recommendations for the pharmacological treatment of psoriatic arthritis (PsA).
Methods According to the EULAR standardised operating procedures, a systematic literature review was followed by a consensus meeting to develop this update involving 28 international taskforce members in May 2019. Levels of evidence and strengths of recommendations were determined.
Results The updated recommendations comprise 6 overarching principles and 12 recommendations. The overarching principles address the nature of PsA and diversity of both musculoskeletal and non-musculoskeletal manifestations; the need for collaborative management and shared decision-making is highlighted. The recommendations provide a treatment strategy for pharmacological therapies. Non-steroidal anti-inflammatory drugs and local glucocorticoid injections are proposed as initial therapy; for patients with arthritis and poor prognostic factors, such as polyarthritis or monoarthritis/oligoarthritis accompanied by factors such as dactylitis or joint damage, rapid initiation of conventional synthetic disease-modifying antirheumatic drugs is recommended. If the treatment target is not achieved with this strategy, a biological disease-modifying antirheumatic drugs (bDMARDs) targeting tumour necrosis factor (TNF), interleukin (IL)-17A or IL-12/23 should be initiated, taking into account skin involvement if relevant. If axial disease predominates, a TNF inhibitor or IL-17A inhibitor should be started as first-line disease-modifying antirheumatic drug. Use of Janus kinase inhibitors is addressed primarily after bDMARD failure. Phosphodiesterase-4 inhibition is proposed for patients in whom these other drugs are inappropriate, generally in the context of mild disease. Drug switches and tapering in sustained remission are addressed.
Conclusion These recommendations provide stakeholders with an updated consensus on the pharmacological management of PsA, based on a combination of evidence and expert opinion.
- psoriatic arthritis
- treatment
- DMARDs (biologic)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Psoriatic arthritis (PsA) is a disease with heterogeneous manifestations in patients who have manifest or latent psoriasis. It comprises both musculoskeletal as well as non-musculoskeletal manifestations; the latter particularly include the skin and the nails, but also potentially the gut (inflammatory bowel disease) or the eyes (uveitis). Active chronic PsA also associates with cardiovascular, psychological and metabolic comorbidities,1–7 which, together with the musculoskeletal manifestations, impose a significant patient burden with impact on quality of life and also accelerated mortality.8–10
The day-to-day management of patients with PsA includes non-pharmacological as well as pharmacological interventions. The number of disease-modifying antirheumatic drugs (DMARDs) indicated for PsA has increased during the last decade. The armamentarium now includes not only conventional synthetic DMARDs (csDMARDs) such as methotrexate (MTX), sulfasalazine and leflunomide and tumour necrosis factor inhibitors (TNFi), but also other targeted biological agents (bDMARDs) aimed at different cytokines, such as TNF, interleukin (IL)-12/23 and IL-17A, as well as targeted synthetic DMARDs (tsDMARDs) that inhibit phosphodiesterase-4 (PDE4) or Janus kinases (JAKs).11–16 These multiple newer drugs have been investigated well in short-term, randomised controlled trials using placebo as comparator for reasons of drug approval. However, comparative research of different drugs, important for clinical practice, is rather sparse and clinicians need some guidance in decision-making.17–20
The European League Against Rheumatism (EULAR) developed recommendations for the pharmacological management of PsA in 2011 and updated them in 2015. These recommendations had their main focus on the musculoskeletal aspects of the disease and addressed the entire spectrum of PsA severity since they pertained to patients with very mild to very severe PsA.12 15 18 In this rapidly evolving field, a further update of the 2015 recommendations became necessary to accommodate newly obtained evidence and insights. The objective of this taskforce, therefore, was to update the EULAR recommendations for the management of PsA with non-topical, pharmacological therapies.
Methods
The updated EULAR standardised operating procedures were applied.21 In October 2018, a steering group consisting of five rheumatologists, a fellow, a patient research partner and a health professional defined the questions that were to be addressed through a systematic literature review (SLR). The SLR was performed between October 2018 and May 2019, for the years 2015–2018, and analysed the efficacy in both musculoskeletal manifestations as well as the skin and nails in patients with PsA.1 Of note, the SLR was not centred on skin psoriasis trials, and these trials are not reviewed systematically or alluded to systematically here. Where relevant and based on expert opinion, data made available after the end of the SLR were also integrated. In May 2019, the steering group as well as the taskforce met to integrate available information on disease management in PsA into practical recommendations. The taskforce consisted of 28 persons from 15 European countries with 15 different healthcare systems: 21 rheumatologists, 2 people affected with PsA, 1 health professional, 1 dermatologist and 3 rheumatology fellows/trainees. The taskforce comprised more than 30% new members compared with 2015.
The SLR informed the recommendations. However, the process was not only evidence-based but also experience-based and consensus-based, in line with the three-tier principles of evidence-based medicine that include clinical science (trials), patients’ perceptions and expectations, and physicians’ experiences. Benefit to cost ratios were taken into consideration when discussing prioritisation of drugs, since new effective treatments impose a significant burden on the healthcare budgets of EULAR and non-EULAR countries. Treatment guidance should therefore not only include considerations about safety and efficacy but should also focus on cost of treatment, in particular when different therapies have similar efficacy and safety data.
The results of the SLR were presented to the taskforce during a face-to-face meeting in May 2019, alongside the 2015 recommendations and proposals for changes to these recommendations prepared by the steering committee. Each recommendation was discussed in detail both in smaller (breakout) groups and in plenary sessions until consensus was reached. For changes to existing recommendations against which no new evidence has accrued since the last update, a ≥75% vote by the taskforce was mandated in order to prevent new taskforces from reformulating without major reasoning what had previously been developed based on the evidence presented at that point in time. If this majority was not reached, the recommendation was not changed. New recommendations were formulated and then accepted if ≥75% of the members agreed; if this agreement was not reached, the recommendation was reworded and subjected to a renewed vote for which a ≥67% majority was required. If this was not achieved, the wording underwent a next round of discussion and the new phrasing was approved if >50% of the taskforce members voted for it.
After the face-to-face meeting, the taskforce members were provided with the category of evidence and grade of recommendation for each item, based on the Oxford Evidence Based Medicine categorisation, as per the EULAR procedures.21 22 Then an anonymised, email-based voting on the level of agreement among the taskforce members was performed on a 0–10 scale (with 10 meaning full agreement) allowing calculation of mean levels of agreement.
Results
The recommendations are shown in table 1, and the modifications compared with the previous recommendations are shown in table 2. These recommendations address non-topical pharmacological treatments with a main focus on musculoskeletal manifestations. As before, the updated recommendations are targeted at various stakeholders, such as (1) experts involved in the care of patients with PsA, particularly rheumatologists and other health professionals (such as rheumatology nurses), but also general practitioners, dermatologists and other specialists; (2) people with PsA who can use these recommendations for information on current therapies, treatment strategies and opportunities; and (3) other stakeholders which include government and hospital officials, patient organisations, regulatory agencies and reimbursement institutions.
2019 EULAR recommendations for the pharmacological management of psoriatic arthritis, with levels of evidence, grade of recommendations and level of agreement
Comparison of the 2015 and 2019 recommendations
Overarching principles
These refer to principles of a generic nature (table 1). Note that optimal management of patients with PsA also requires non-pharmacological strategies such as patient education and regular physical exercise and may also require topical medication (in particular for skin psoriasis). The non-systemic and non-pharmacological therapies are not addressed in the present document.23
The overarching principles remained mostly unchanged compared with 2015 (table 2). Principle A refers to the heterogeneous and potentially severe nature of PsA, and principle B addresses the importance of shared decision-making with the patient, but also costs. Indeed, while efficacy and safety are considered to be the key drivers of the decision-making process, the committee noted that cost of treatment should also be taken into account. Modern DMARDs are expensive and unaffordable to many patients in less-affluent countries, but also in affluent countries social security systems may preclude provision of certain drugs to a significant proportion of patients, or request clinically unacceptable conditions (such as high disease activity or limitation of important agents to a maximum number) for cost reasons. Nevertheless, EULAR proclaims that all patients with active and/or severe (not necessarily highly active) PsA should have the right to be prescribed the treatment they need to optimise their quality of life. Of note, recently, costs of some drugs have decreased considerably through access to biosimilars and bio-originator repricing, but these advantages are not conveyed in all countries alike.
The pivotal status of the rheumatologist as the main caregiver for people with PsA is dealt with in principle C. Rheumatologists possess the optimal depth and breadth of experience regarding the use of all types of DMARDs, including efficacy outcomes, risk assessment and knowledge of comorbidities. The role of nurses and other health professionals in the management of PsA, in relation to principles A and B, was addressed by the taskforce. While rheumatologists are the principal physicians in the care of PsA, in some countries rheumatology nurses may prescribe medication and are the main healthcare givers for patients. On the other hand, in certain areas of the world, rheumatology training is not sufficiently available and other experts may care for patients with PsA, hence the term ‘primarily’. Where there is a lack of rheumatologists, the taskforce recognised the contribution of other physicians with appropriate rheumatological expertise and added this point also into the research agenda (table 3).
Research agenda for PsA
The treatment target is elimination of inflammation and optimisation of quality of life (principle D) (see table 1 and the 2015 update for detailed information).18 The importance of fatigue was also highlighted.1 5 7 10 24
The last two overarching principles refer to treatment strategy and have been modified. Principle E is a new overarching principle which reiterates the importance of all musculoskeletal manifestations in patients with PsA: this not only relates to peripheral arthritis but also enthesitis, tenosynovitis, tendinitis, dactylitis and inflammatory axial disease.
Principle F (which in 2015 was principle E) now includes the term ‘non-musculoskeletal’, replacing the term ‘extra-articular’ manifestations, and refers to PsA-linked organ involvement, namely psoriasis, uveitis and inflammatory bowel disease. The term ‘extra-articular manifestations’ was considered unclear—for some it includes axial or entheseal symptoms, which was not intended in this context.25–27 Although all the non-musculoskeletal manifestations should be taken into account, psoriasis is of course the most frequent. Referring to comorbidities, aside from cardiovascular disease, depression is explicitly mentioned because of its frequency and impact on the patient.4 7 10 24 28 29 The list of comorbidities is not meant to be exhaustive and other comorbidities should also be considered.
Recommendations
Twelve recommendations were formulated or updated (tables 1 and 2) and formed the basis of the management algorithm (figure 1). Table 1 provides the category of evidence, grade of recommendation and level of agreement for each of the points.17 It must be borne in mind that the individual disease characteristics—in line with the multidimensional nature of PsA—may respond differently to specific therapies and thus require use of distinct assessment instruments for each manifestation. This variability as well as contraindications and risks must be taken into account, and thus the balance between efficacy and safety is always dependent on the characteristics of the individual patient. Both table 1 and figure 1 synthesise the recommendations in an abbreviated way, and the accompanying text provides more detailed information about the evidence and the discussion process and should be regarded as integral to the recommendations.
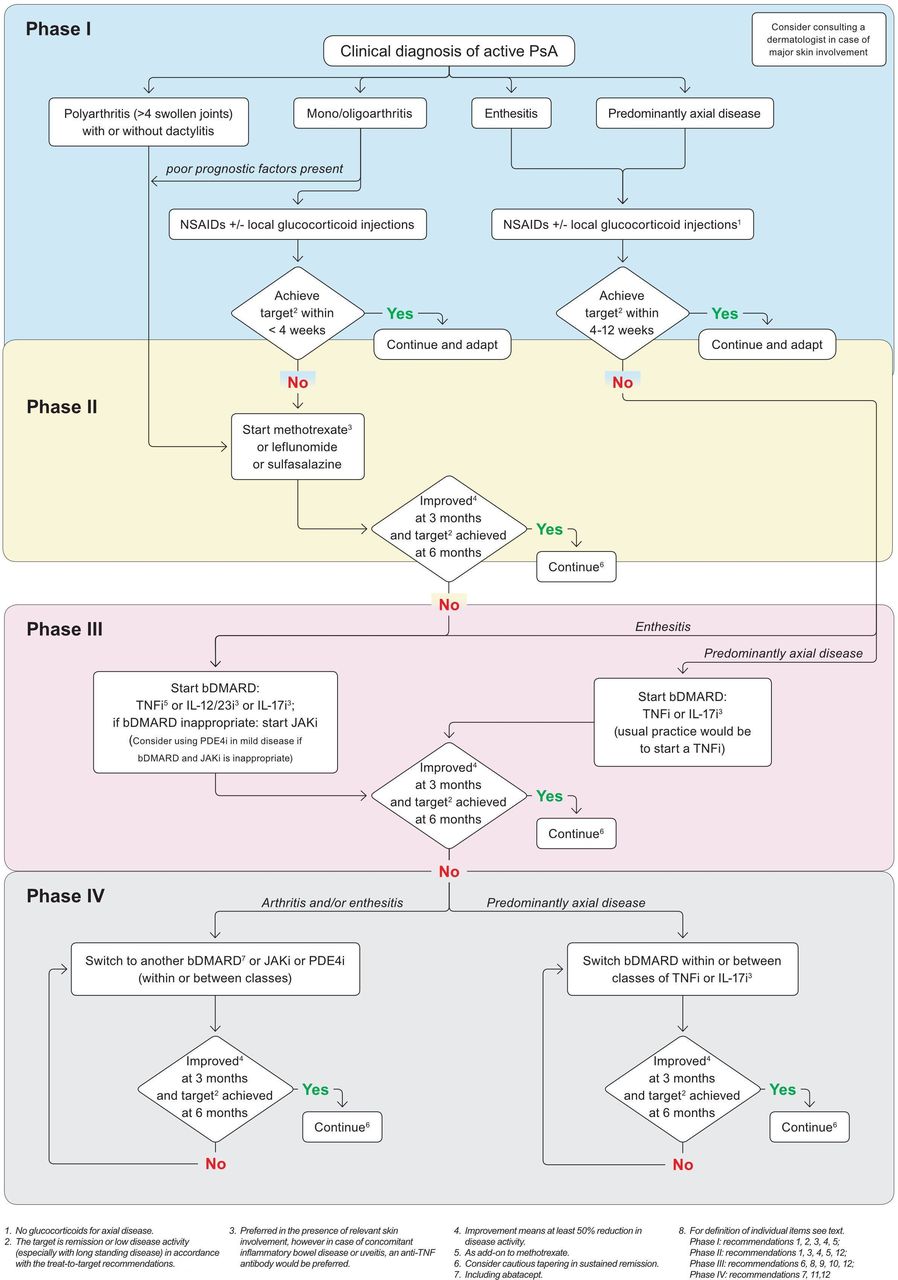
{kind=link}
The EULAR 2019 algorithm for treatment of PsA with pharmacological non-topical treatments. bDMARDs, biological disease-modifying antirheumatic drugs; EULAR, European League Against Rheumatism; IL-12/23i, interleukin-12/23 inhibitor; IL-17i, interleukin-17 inhibitor; JAKi, Janus kinase inhibitor; NSAIDs, non-steroidal anti-inflammatory drugs; PDE4i, phosphodiesterase-4 inhibitor; PsA, psoriatic arthritis; TNFi, tumour necrosis factor inhibitor.
Recommendation 1: Treatment should be aimed at reaching the target of remission or, alternatively, low disease activity, by regular disease activity assessment and appropriate adjustment of therapy.
This recommendation puts forward the importance of a treat-to-target (T2T) approach. The T2T strategy, which comprises definition of a distinct target as well as adherence to rules for monitoring and therapeutic adjustment, is well validated particularly in rheumatoid arthritis.30 The T2T recommendations for PsA have been updated recently.31 32 In line with these recommendations, this point has been slightly rephrased and now states clearly that remission or low disease activity should be targeted, with the deletion of the previously stated term of minimal disease activity (which refers to a score allowing the assessment of low disease activity rather than to a target).33 34 Remission in PsA is difficult to define.33 Remission should be seen as abrogation of inflammation.
Recommendation 2: Non-steroidal anti-inflammatory drugs may be used to relieve musculoskeletal signs and symptoms.
As in previous versions the taskforce continues to recommend the use of an non-steroidal anti-inflammatory drug (NSAID) to relieve symptoms.18 The benefit to risk ratio of NSAIDs must always be considered carefully, especially in this population with frequent cardiovascular comorbidities.
The taskforce noted that, in contrast to rheumatoid arthritis, in mild synovitis in PsA or for non-synovial features including axial symptoms, NSAIDs alone may be sufficient to control symptoms, especially with local glucocorticoid injections (see recommendation 3). There are little data regarding the efficacy of NSAIDs in enthesitis. In patients with peripheral arthritis, NSAIDs should be combined rapidly with DMARDs if needed (see also recommendations 4 and 5). NSAIDs have not shown any efficacy in skin psoriasis. When peripheral arthritis is present, NSAID monotherapy without DMARDs should not exceed 1 month if disease activity persists, and other treatment possibilities should be considered. When axial or entheseal involvement dominates the clinical picture, the duration of NSAID therapy might be prolonged up to 12 weeks, provided they have already induced relief by 4 weeks.35 If the treatment target is not achieved, other therapies should be prescribed as detailed in the subsequent recommendations.
Recommendation 3: Local injections of glucocorticoids should be considered as adjunctive therapy in psoriatic arthritis; systemic glucocorticoids may be used with caution at the lowest effective dose.
This recommendation is unchanged compared with 2015 but has been reordered to better align with the different phases of treatment (figure 1).18 It has to be also noted that glucocorticoid therapy should be used for only a short period of time. The taskforce does not recommend the use of systemic glucocorticoids for axial disease.35
Recommendation 4: In patients with polyarthritis, a csDMARD should be initiated rapidly, with methotrexate preferred in those with relevant skin involvement.
The main change in recommendations 4 and 5 (together recommendation 3 in 2015) is the separation of polyarticular versus oligoarticular joint involvement to ensure that the poorer prognostic nature of polyarthritis is more strongly emphasised than this was done before. The taskforce defined polyarticular disease as five or more active (swollen) joints.36 Patients with polyarticular disease should receive a csDMARD either as first-line drug or after only a short course of NSAIDs. ‘Rapid’ infers prompt commencement of a csDMARD, commensurate with the severity of clinical presentation or comorbidities; delays should not exceed 2 weeks. Thus, while recommendation 4 has been newly added, it was already comprised in former recommendation 3, where ‘many swollen joints’ was mentioned as a poor prognostic marker requiring rapid (‘early’) institution of DMARDs.
This recommendation, as well as recommendation 5, places the use of csDMARDs in the management of PsA as first-line DMARDs. The continuous prioritisation of csDMARDs reflects consensual expert opinion within the taskforce that favoured the benefit to risk balance of csDMARDs and in particular MTX over biologicals, as well as their lower cost. Data supporting the use of MTX in PsA are scarce and include only small or inconclusive clinical trials,37 as well as indirect evidence stemming from the TICOPA trial and evidence from observational studies.38–41 However, the SEAM-PsA study, which was part of the SLR and has meanwhile been published in full, revealed that MTX has similar efficacy in joint counts, skin involvement, enthesitis, dactylitis and physical function as etanercept or even etanercept plus MTX.42 Given this similarity of effectiveness, and the differences in costs, this study further supports the taskforce’s decision to place MTX and other csDMARDs at the top of the therapeutic algorithm (figure 1).
The taskforce acknowledged that patients may have a reluctance to take MTX and may experience adverse effects. To our knowledge, data proving that MTX is less well tolerated in PsA than in rheumatoid arthritis are lacking, but the effects of and the overall long-term experience with MTX should be part of the information given to the patient in the process of shared decision-making.43 Thus far, MTX remains widely used in daily practice as reported in registries, has high treatment maintenance over time and seems effective in the control arms of most clinical trials, in which disease control with MTX monotherapy appears satisfactory.42
MTX is highlighted among the csDMARDs, in particular for patients with ‘relevant’ skin involvement: ‘relevant’ is defined as either extensive (body surface area involvement >10%), or as important to the patient: more limited psoriasis leading to significant impact on quality of life (eg, face/hand/feet/genital involvement). This definition would correspond, in other dermatological terms, to moderate to severe psoriasis. MTX has proven efficacy in skin psoriasis, is recommended in treatment guidelines for psoriasis and has become the standard csDMARD for skin psoriasis in many countries.44–47
On the other hand, MTX leads to hepatotoxicity, and data on the beneficial effects of MTX on cardiovascular disease in PsA are conflicting.48 49 Taking all these elements into account, the taskforce felt a gradual approach to intensify PsA treatment most appropriate and proposed a csDMARD (usually MTX) as the first DMARD. MTX should be prescribed attempting to reach 25 mg per week as the optimal dose and with folate supplementation. Other csDMARDs have shown efficacy in PsA as well and may also be considered at this stage (although with less efficacy in the skin): these include leflunomide and sulfasalazine.50 Ciclosporin is not recommended for PsA.
If improvement does not exceed 50% of a composite measure for PsA within 3 months or the treatment target is not reached within 6 months, such csDMARD therapy should not be pursued longer (figure 1). In light of paucity of good clinical data, the search for better evidence for the efficacy of csDMARDs as monotherapy or as combination therapy was prioritised on the research agenda.
Recommendation 5: In patients with monoarthritis or oligoarthritis, particularly with poor prognostic factors such as structural damage, high erythrocyte sedimentation rate/C reactive protein, dactylitis or nail involvement, a csDMARD should be considered.
This recommendation emphasises that patients with oligoarticular disease should (similar to polyarticular patients) receive a csDMARD rapidly in the presence of poor prognostic factors (please see the text of the recommendation). Concerning factors associated with poor prognosis (here defined as radiographic severity), the SLR identified nail involvement in addition to those factors presented in 2011 and 2015, and this element was added accordingly to the phrasing of recommendation 5.51 52
Dactylitis was previously addressed together with enthesitis (see recommendation 9 in 2015). However, these manifestations have now been separated. The taskforce considered that dactylitis was distinct in terms of physiopathology, diagnosis and prognosis, since it is linked to radiographic changes in PsA, whereas enthesitis is not.53 Furthermore, although there is a lack of good-quality data, recent studies suggest at least some efficacy of MTX in dactylitis.41 42 Thus, dactylitis should now be treated similarly to arthritis, and if associated with polyarticular disease it should be treated like polyarthritis. Of note, NSAIDs have not demonstrated efficacy in dactylitis.
Given the lack of strong data on oligoarticular PsA, this recommendation was based more on expert opinion than on hard data (level of evidence, 4; grade of recommendation: C).
Recommendation 6: In patients with peripheral arthritis and an inadequate response to at least one csDMARD, therapy with a bDMARD should be commenced; when there is relevant skin involvement, an IL-17 inhibitor or IL-12/23 inhibitor may be preferred.
This recommendation addresses patients with peripheral arthritis, after failure or intolerance to at least one csDMARD. In these patients, the taskforce recommends a bDMARD. In some patients, especially those without bad prognostic factors or those with mild disease activity, it may be indicated to rotate to a second csDMARD before starting a bDMARD, as previously outlined in the 2015 recommendations.12
The taskforce extensively discussed the legitimacy of a bDMARD as first DMARD strategy; the discussion focused on efficacy and safety, as well as on costs. The taskforce was of the opinion that many patients respond satisfactorily to MTX, while tolerating the drug well. These patients would be subjected to overtreatment if starting a bDMARD immediately rather than waiting for 3 months to determine if a response to MTX has occurred (see recommendations 9 and 10). A good example is revealed in the SEAM-PsA trial. However, if entheseal or axial inflammatory involvement predominates, earlier use of bDMARDs is proposed, since csDMARDs are ineffective in these conditions (please see recommendations 9 and 10).
Whereas the 2015 recommendation stated that it was ‘usual practice’ to start a TNFi in comparison with other bDMARDs, the current update does not distinguish anymore between TNFi, IL-12/23 inhibitor (IL-12/23i) and IL-17 inhibitor (IL-17i). The SLR reconfirmed the efficacy of TNFi in PsA, and there are now reassuring long-term safety data with these drugs, including data indicating that the incidence of malignancies is not increased.54 55 Drugs targeting IL-12/23 and IL-17 are also consistently efficacious in comparison with placebo and long-term safety seems favourable.1 In addition to secukinumab, a second IL-17i, ixekizumab, has been approved since the 2015 recommendations, showing a similar efficacy and safety profile, which further reassured the taskforce.14 56 Importantly, a head-to-head trial of ixekizumab versus the TNFi adalimumab showed similar efficacy of ixekizumab and adalimumab for musculoskeletal manifestations.57
Of note, efficacy in joints appeared numerically less for the IL-12/23i ustekinumab; however, observational data indicate similar magnitudes of response versus TNFi, and a formal head-to-head trial is currently lacking.13 58 Furthermore, the taskforce noted that recent studies with biologicals targeting the IL-23-p19 subunit (guselkumab, risankizumab, tildrakizumab) appear encouraging, and that targeting this pathway has shown excellent efficacy in psoriasis.59–63 Thus, a suggested order between different targeted pathways is intentionally not given in this recommendation.
The total safety picture of these three categories of bDMARDs appeared acceptable in our SLR.1 The risks of TNFi are well known from large registries for long-term safety including these drugs. IL-17i may increase the incidence of (mild) localised candidiasis, and monitoring for a possible increased risk of inflammatory bowel disease is still ongoing.64 In any case, safety must always be considered carefully in every patient; more complete information regarding the safety aspects of bDMARDs is provided in the drugs’ package inserts.
Taking together data on efficacy and safety, with regard to the treatment of arthritis in PsA, the taskforce found no reason to currently prioritise one of these bDMARDs over another one (as shown also in figure 1); costs should also be taken into account, and these may vary at the country level.
In contrast, both IL-12/23i and IL-17i have shown greater efficacy in skin than TNFi, in head-to-head trials of psoriasis and PsA62 65 66; this evidence justifies the second half of the recommendation, which encourages the use of an IL-12/23i or IL-17i in patients with relevant skin involvement, where ‘relevant’ is defined (as above) as either extensive or as important to the patient.
When choosing a first bDMARD, the differential impact on certain musculoskeletal and non-musculoskeletal manifestations as well as comorbidities such as metabolic syndrome has to be considered. While important skin involvement was already mentioned, IL-12/23 inhibition may not be effective for axial involvement; IL-17 inhibition may not be appropriate for patients with concomitant inflammatory bowel disease for which monoclonal antibodies to TNF and IL-12/23 inhibitors are approved; and in the presence of uveitis, a monoclonal antibody to TNF may be the preferred first and second bDMARD because of respective approval.67 68 On the other hand, regarding comorbidities, the paucity of relevant data precludes firm recommendations at present; this has been added to the research agenda.
The issue of monotherapy with bDMARDs versus combination therapy with a csDMARD was discussed.69 70 The current recommendation is to continue MTX with a bDMARD (using the latter as an add-on strategy) in patients already taking this drug and tolerating it well, but the taskforce admitted that to date there is no clear evidence that combination therapy is more efficacious than monotherapy, aside from a slight reduction of immunogenicity that is of doubtful clinical significance.71 We suggest that MTX dose may be reduced in subjects showing a good biological drug response, especially when there are concerns about MTX toxicity. However, more data are needed and this point was put into the research agenda.
Recommendation 7: In patients with peripheral arthritis and an inadequate response to at least one csDMARD and at least one bDMARD, or when a bDMARD is not appropriate, a JAK inhibitor may be considered.
At this moment, the only JAK inhibitor (JAKi) approved for PsA is tofacitinib. Our SLR indicated tofacitinib may have similar efficacy as the TNFi adalimumab for joint involvement, but numerically lower efficacy in skin psoriasis.1 15 72 There also appears to be satisfactory efficacy of tofacitinib in TNFi insufficient-responder populations.1 According to European Medicines Agency approval, tofacitinib must be prescribed with MTX. Safety signals exist for some infections, especially herpes zoster, as well as a recent signal for deep vein thrombosis especially with a high dose of tofacitinib which is not approved for PsA, but also the usual 5 mg twice daily dose particularly in those with cardiovascular risk factors and older patients.15 72 73
To date, two other JAKis are in development phases for PsA. Filgotinib showed promising efficacy in a phase II trial and upadacitinib was approved for use in rheumatoid arthritis shortly after the development of these recommendations, and also showed encouraging results in PsA.16
Taking these elements into account, as well as the general principle of favouring drugs with robust long-term safety data, the taskforce proposed JAKi either after inadequate response or intolerance to at least one bDMARD, or when a bDMARD is considered not appropriate. ‘Not appropriate’ means, for example, non-adherence to injections or a strong patient preference for an oral drug (in accordance with the overarching principle A concerning ‘shared decision making’). However, the group agreed that normally the step-up approach would be a csDMARD followed by a bDMARD, and subsequently another bDMARD or a JAKi.
As new data become available, the current positioning of JAKis may evolve; this will justify an update of the recommendations if appropriate.
Recommendation 8: In patients with mild disease and an inadequate response to at least one csDMARD, in whom neither a bDMARD nor a JAK inhibitor is appropriate, a PDE4 inhibitor may be considered.
Similar to the 2015 update, this recommendation reserves a special place for apremilast: it should be used only when csDMARD therapy has failed and bDMARDs and JAKi are not appropriate; however, the taskforce considered that the value of apremilast may be found in treating patients with relatively mild disease or those in whom other agents are contraindicated, such as in patients with chronic infections. Mild disease is defined here as only few joints (four or less, thus oligoarticular disease), lower disease activity by composite scores and/or limited skin involvement. The reason for proposing the use of apremilast primarily for mild disease is that profound responses, such as Amercian College of Rheumatology 70% (ACR70), are rarely seen in clinical trials with apremilast and are sometimes not different from placebo.11 74–77 Moreover, radiographic data providing the disease-modifying potential of the drug are still lacking for apremilast, and therefore this drug may not be appropriate for patients with poor prognostic factors. A randomised controlled trial with apremilast in oligoarticular disease is currently under way.78
The level of agreement with this recommendation was lower than for the others, suggesting diverse expert views on the place of this drug.
Recommendation 9: In patients with unequivocal enthesitis and insufficient response to NSAIDs or local glucocorticoid injections, therapy with a bDMARD should be considered.
Compared with recommendation 8 of the 2015 version, ‘active enthesitis’ has been replaced by ‘unequivocal enthesitis’, and the last part stating that ‘current practice is to use a TNF-inhibitor’ has been omitted. In patients with enthesitis, NSAIDs and local glucocorticoids are the first-line treatment; in case of insufficient response, intolerance or contraindication to NSAIDs, and given that csDMARDs are not efficacious for enthesitis, a bDMARD (targeting TNF, IL-17 or IL-12/23) may be used. ‘Enthesitis’ here refers to inflammation rather than entheseal pain, and the term ‘unequivocal’ has now been added to avoid overtreating trigger-point pain that has other underlying causes (such as concomitant widespread pain syndromes).79 While sonography or MRI may underpin the presence of enthesitis, clinical examination should in principle suffice, and the number and pattern (asymmetrical) of painful entheses, as well as the presence of clinical swelling, should guide the clinician and allow a distinction from widespread pain syndromes.80–85 Entheseal disease is a complex issue in PsA and was also added to the research agenda.
Regarding bDMARDs, the taskforce now regards all bDMARDs as having efficacy of a similar magnitude for enthesitis and hence the preference for TNFi has been deleted.1
Recommendation 10: In patients with predominantly axial disease which is active and has insufficient response to NSAIDs, therapy with a bDMARD should be considered, which according to current practice is a TNF inhibitor; when there is relevant skin involvement, IL-17 inhibitor may be preferred.
In 2015, predominant (or highly significant) axial involvement was dealt with in recommendation 9. The phrasing of the current recommendation was partly aligned with the Assessment of Spondyloarthritis International Society (ASAS)/EULAR management recommendations for axial spondyloarthritis (axSpA),35 with the exception that these do not yet account for the use of IL-17is. It also reflects that in the situation of predominantly axial disease, TNFi would still represent the first bDMARD by usual practice. The taskforce discussed that secukinumab has demonstrated efficacy in axSpA, and recently has demonstrated efficacy in patients considered to have predominant axial PsA.86 However, the experience with IL-17 inhibition in terms of long-term efficacy and safety in axSpA and axial PsA is limited.
In predominantly axial PsA, in the presence of relevant skin involvement (as defined in the text below recommendation 4), an IL-17i would be preferred over a TNFi, given the greater efficacy of IL-17i in skin.57 Importantly, however, in case of concomitant inflammatory bowel disease or uveitis, a TNFi (monoclonal antibody) would be preferred.
Of note, the IL-12/23 pathway drugs did not demonstrate efficacy in axSpA.87 Thus, in light of lack of clear efficacy, drugs targeting IL-12/23 and abatacept (see also recommendation 11) are not indicated for patients with predominantly axial disease.87
Recommendation 11: In patients who fail to respond adequately to, or are intolerant of a bDMARD, switching to another bDMARD or tsDMARD should be considered, including one switch within a class.
This recommendation, a slight expansion of the recommendation previously numbered as 10, addresses first bDMARD failure or intolerance. Here we propose a switch either to another bDMARD or to a tsDMARD, especially a JAKi. Novel data on switches are limited, with only one such new study found through the SLR.88 Trials performed in TNFi insufficient responders have demonstrated efficacy of bDMARDs with another mode of action when TNFi has failed.56 However, another TNFi can also be used, since no head-to-head trial data are available that suggest switching between classes is different from switching within class. Finally, the taskforce agreed that while switching within class was a viable option, it would be logical to change class after a second failure within a given class (expert opinion). Studies addressing the best possible strategy after failure(s) of bDMARDs other than TNFi are lacking to date, and this topic was added to the research agenda.
The taskforce discussed the place of abatacept, which has been approved for use in PsA, and considered abatacept’s place in the current algorithm should be limited to potential use after other bDMARDs have failed, given its relatively low efficacy.89
Recommendation 12: In patients in sustained remission, cautious tapering of DMARDs may be considered.
This is a new recommendation, primarily based on broad consensus among experts in the absence of solid trial data. Sparse data suggest a certain risk of relapse (either for joints or skin) when tapering.90–95 Still, the taskforce decided to offer guidance on tapering, since it was felt an important aspect of modern management, especially when sustained remission has been achieved, to mitigate treatment-related risks, to meet patients’ desires and demands, and to reduce cost of treatment.
Tapering was considered appropriate only in the context of sustained remission, defined here as complete remission (rather than low disease activity) for at least six consecutive months.32
This point was deliberately phrased tentatively, with a recommendation to taper with great caution, as a consequence of shared decision-making based on comprehensive patient information. The recommendation does not have the intention to push clinicians towards stopping treatment but rather to try finding the smallest effective dose, either through dose reduction or interval lengthening. Best possible tapering strategies were also added as an item to the research agenda (table 3).
Discussion
Since the last update of these recommendations, new information has accumulated on the efficacy and safety of established drugs and treatment strategies, but also on newer agents such as IL-17is and IL-12/23is as well as JAKis. Thus, while these updated recommendations continue to integrate the established as well as the new information, they also continue to attempt covering the broad spectrum of disease severity that best reflects clinical practice, in order to guide clinicians and other stakeholders involved in treating patients with PsA with a simple algorithm and set of recommendations that can easily be translated into daily clinical practice. Importantly, all of this information is based on a thorough SLR and on conclusions by an expert committee that primarily used evidence to derive its recommendations, but also specialists’ opinions, where evidence was lacking or was insufficient.
These recommendations have been modified substantially compared with the 2015 update, since new drugs have entered the market and more evidence about existing drugs has accrued (table 2). In particular, longer term safety data have become available, which add importantly to the robustness of the evidence. In general this update adheres to the previous structure of these recommendations in all respects. (1) We continue to separate this guidance document into overarching (general) treatment approaches and individual therapeutic recommendations. (2) We continue to recommend targeting clinical remission (primarily for early disease) or, alternatively, low disease activity (for established disease); in this light, a moderate let alone high disease activity state is unacceptable, unless comorbidities or other patient factors preclude treatment advances. (3) We continue to recommend a T2T strategy; the T2T recommendations have been recently updated and propose at least 50% improvement of the composite measure within 3 months and achievement of the target within 6 months from treatment initiation, thus requiring the use of a continuous measure of disease activity to follow patients longitudinally and also reflect patient perceptions. (4) As before, we structure the pathway to a successful outcome into four phases, an initial phase which might suffice in very mild disease or necessitate advancement to one of the next two phases; a second phase focusing on the use of csDMARDs; a third phase for patients who failed to reach the target in phase II and/or phase I when exhibiting predominant axial or entheseal disease; and a fourth phase for those who failed phase III.
Further, we provide a quantitative rather than only a qualitative assessment of the evidence available for all agents dealt with—not every drug that is approved must be assigned the same level of applicability if the database suggests differences, even if head-to-head trials are largely missing.57 In our view it is the task of expert committees to judge and qualify available data to the best of their knowledge for the best outcomes of the patients by interpreting the relevance of the available data after a thorough debate and decision-making process. Thus, we weighed the evidence provided by the SLR in the course of the discussion and voting process. We aimed and aim at providing recommendations that are not only truthful, but also have face validity and thus usefulness.
In preparing the recommendations, the taskforce adhered to the EULAR operating procedures for the development of recommendations and assessed evidence levels according to the Oxford Evidence Based Medicine approach.21 22 Finally, the focus of this taskforce was on the musculoskeletal manifestations and, while mentioning the need to consult other specialists, these recommendations, in line with the composition of the taskforce, are primarily aimed at rheumatologists and their patients with PsA. Recommendations for other specialists should be sought in the respective specialty literature.
Unlike other organisations that have also released treatment recommendations for PsA, EULAR has decided to not pursue Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology for prioritising available treatments. While GRADE methodology is widely used and highly appreciated for properly judging quality of available evidence, experts within EULAR feel that GRADE puts too much emphasis on the methodology itself and tends to downplay prevalent but poorly investigated clinical scenarios for which clinicians still seek guidance. A good example of the latter is the place of MTX as first-line treatment: while we acknowledge the absence of good clinical evidence for MTX as first-line DMARD, we still recommend it as such, by virtue of long-term positive clinical experience, including data from registries, as well as recent encouraging results, such as in the TICOPA and SEAM-PsA trials,42 long-term positive clinical experience, widespread fame and low treatment cost. We think this set of practical recommendations, which has been developed according to general principles of evidence-based medicine, will help rheumatologists in choosing the most appropriate and cost-effective drug treatment for every patient with PsA and in every clinical scenario, even though the body of scientific evidence may fall short in many aspects of the disease. We recognise the fields in which evidence is sparse or lacking are crucially important, and they frame the research agenda. We hope that clinical researchers will be influenced by and appreciate the clinical questions summarised in the research agenda, and design experiments or trials aiming at providing resolution to these research questions.
All these aspects have allowed us to provide what the taskforce believes is the right place for the different drug classes in the treatment algorithm. Still, the EULAR PsA recommendations have preserved their original character which they share with other sets of EULAR recommendations for different inflammatory diseases. Important elements thereof are a graduated approach favouring well-known csDMARDs as first-line drugs and allowing escalation to bDMARDs when necessary; preferring drugs with an established long-term track record for safety over those that have recently been approved; and attention for tapering and stopping treatment if possible.
As before, the recommendations make it clear that one drug does not fit all and stipulate the role of the phenotypes and patient characteristics in the decision-making process of starting and stopping treatments. Shared decision-making has become an integral part of the management of patients with PsA. There is also more attention for ‘prognostic profiling’, paying more tribute to clinical reality; while the spectrum of patients with PsA included in trials is skewed towards patients with prognostically unfavourable polyarticular PsA, this type of PsA is a relatively rare condition in clinical practice, especially in the scenario of the initial early disease presentations in contemporary rheumatology practice. Thus, recommendations should also give guidance about how to address patients with milder oligoarticular or monoarticular disease.
Treatment decisions also have to take account of extramusculoskeletal disease manifestations such as inflammatory bowel disease or uveitis, aside from skin involvement, which require distinct therapies (anti-TNF monoclonal antibodies for uveitis, anti-TNF monoclonal antibodies or IL-12/23i for inflammatory bowel disease in the absence of axial involvement) just as they require distinct clinical evaluation. Importantly, these novel pieces of information only originated from the information that was obtained in the course of clinical trials of the various established and new compounds.
As before, the updated recommendations have been summarised in an algorithm. The EULAR algorithm (figure 1) continues to account for the musculoskeletal diversity of PsA and should be easy to follow; where new therapies are particularly efficacious regarding skin involvement, a special note is provided within the algorithm (see also respective footnotes), thus allowing to follow these management recommendations straightforwardly throughout the evolution of the disease.
In summary, the updated treatment recommendations for patients with PsA living in many different countries, under the influence of very different healthcare systems, support decision-making for the management of PsA and address the entire spectrum of the disease. An update will be needed within 2–4 years, as new data arise in PsA.
References
Supplementary materials
Lay summary
Disclaimer : This is a summary of a scientific article written by a medical professional (“the Original Article”). The Summary is written to assist non medically trained readers to understand general points of the Original Article. It is supplied “as is” without any warranty. You should note that the Original Article (and Summary) may not be fully relevant nor accurate as medical science is constantly changing and errors can occur. It is therefore very important that readers not rely on the content in the Summary and consult their medical professionals for all aspects of their health care and only rely on the Summary if directed to do so by their medical professional. Please view our full Website Terms and Conditions.
Copyright © 2020 BMJ Publishing Group Ltd & European League Against Rheumatism. Medical professionals may print copies for their and their patients and students non commercial use. Other individuals may print a single copy for their personal, non commercial use. For other uses please contact our Rights and Licensing Team.
Footnotes
Handling editor David S Pisetsky
Twitter @KragstrupTW, @R_M_Santiago
Contributors All authors have contributed to this work and approved the final version.
Funding This study was funded by the European League Against Rheumatism. DMG and HM-O are supported by the National Institute for Health Research (NIHR) Leeds Biomedical Research Centre (LBRC). The views expressed are those of the authors and not necessarily those of the (UK) National Health Service (NHS), the NIHR or the (UK) Department of Health.
Competing interests LG: AbbVie, Biogen, Celgene, Janssen, Lilly, Mylan, Novartis, Pfizer, Sandoz, Sanofi-Aventis, UCB. XB: AbbVie, Amgen, BMS, Celgene, Chugai, Hexal, Janssen, Lilly, MSD, Mylan, Novartis, Pfizer, Sandoz, UCB. AK: Bristol-Myers Squibb, Celgene, Eli Lilly, Gilead, Merck Sharp and Dohme, Novartis, Pfizer. MdW: Through Stichting Tools from AbbVie, BMS, Celgene, Eli Lilly, Janssen-Cilag, Novartis, Pfizer, Roche. IM: AbbVie, BMS, Lilly, Novartis, Celgene, Gilead, Janssen, Boehringer, UCB, Pfizer. MD: AbbVie, BMS, Janssen, Lilly, Novartis, Merck, Pfizer, UCB. JP: BMS, Pfizer. DGM: AbbVie, BMS, Celgene, Eli Lilly, Janssen, Merck, Novartis, Pfizer, UCB. DA: AbbVie, Amgen, Gilead, Lilly, Merck, Novartis, Pfizer, Roche, Sandoz, Sanofi/Genzyme, Sobi. AB: AbbVie, Amgen, AstraZeneca, Angelini, AlfaSigma, BMS, Berlin-Chemie, Egis, Ewopharma, GSK, Lilly, Mylan, MSD, Novartis, Pfizer, Roche, Sandoz, Sanofi, Teva, UCB, Zentiva. PVB: AbbVie, Celgene, Lilly, MSD, Novartis, Pfizer, Richter. HB: Pfizer. W-HB: AbbVie, Almirall, BMS, Celgene, Leo, Lilly, Novartis, Pfizer, UCB. GRB: AbbVie, Celgene, Lilly, MSD, Novartis, Pfizer. JDC: Celgene, Eli Lilly, Gilead, Janssen, Novartis, Pfizer, UCB. NSD: AbbVie, Boehringer Ingelheim, Gedeon Richter, Lilly, Novartis, Pfizer, Roche. TWK: Bristol-Myers Squibb, Eli Lilly, Novartis, Pfizer, UCB. TKK: AbbVie, Amgen, Biogen, BMS, Celltrion, Egis, Eli Lilly, Ewopharma, Hikma, Hospira/Pfizer, MSD, Mylan, Orion Pharma, Roche, Sandoz, Sanofi, UCB. RBML: AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli Lilly, Galapagos, Gilead, MSD, Novartis, Pfizer, UCB. RJUL is Director of Rheumatology Consultancy; AbbVie, Celgene, Eli Lilly, Janssen, Novartis, Pfizer, UCB. HM-O: AbbVie, Celgene, Eli Lilly, Janssen, Novartis, Pfizer, Takeda, UCB. DP: AbbVie, BMS, Celgene, Janssen, Lilly, MSD, Novartis, Pfizer, Roche, UCB. SARM: Janssen, MSD, Novartis. GS: AbbVie, BMS, Celgene, Gilead, Janssen, Lilly, Novartis, Pfizer, Roche, UCB. DJV: AbbVie, Biogen, Boehringer Ingelheim, HealthBeacon, Janssen, Lilly, MSD, Novartis, Pfizer, Roche, UCB. FEVdB: AbbVie, Celgene, Eli Lilly, Galapagos/Gilead, Janssen, Merck, Novartis, Pfizer, UCB. DvdH: AbbVie, Amgen, Astellas, AstraZeneca, BMS, Boehringer Ingelheim, Celgene, Cyxone, Daiichi, Eisai, Eli Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, Merck, Novartis, Pfizer, Regeneron, Roche, Sanofi, Takeda, UCB Pharma; Director of Imaging Rheumatology. JSS: grants to institution from AbbVie, AstraZeneca, Janssen, Lilly, Merck Sharp & Dohme, Pfizer and Roche; speaker for AbbVie, Amgen, AstraZeneca, Astro, Bristol-Myers Squibb, Celgene, Celltrion, Chugai, Gilead, ILTOO Pharma, Janssen, Lilly, Merck Sharp & Dohme, Novartis-Sandoz, Pfizer, Roche, Samsung, Sanofi and UCB.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.