Article Text

Abstract
Objectives To evaluate the cost-effectiveness of treat-to-target strategies among recently diagnosed patients with rheumatoid arthritis (RA) using methotrexate (MTX) and a step-down glucocorticoid (GC) scheme (COBRA Slim) compared with (1) this combination with either sulphasalazine (COBRA Classic) or leflunomide (COBRA Avant-Garde) in high-risk patients and (2) MTX without GCs (Tight-Step-Up, TSU) in low-risk patients.
Methods The incremental cost-utility was calculated from a healthcare perspective in the intention-to-treat population (n=379) of the 2-year open-label pragmatic randomised controlled Care in early RA trial. Healthcare costs were collected prospectively through electronic trial records. Quality-adjusted life years (QALYs) were estimated using mapping algorithms for EuroQoL-5 Dimension. Multiple imputation was used to handle missing data and bootstrapping to calculate CIs. Robustness was tested with biological disease-modifying antirheumatic drugs at biosimilar prices.
Results In the high-risk group, Classic (∆k€1.464, 95% CI −0.198 to 3.127) and Avant-Garde (∆k€0.636, 95% CI −0.987 to 2.258) were more expensive compared with Slim and QALYs were slightly worse for Classic (∆−0.002, 95% CI −0.086 to 0.082) and Avant-Garde (∆−0.009, 95% CI −0.102 to 0.084). This resulted in the domination of Classic and Avant-Garde by Slim. In the low-risk group, Slim was cheaper (∆k€−0.617, 95% CI −2.799 to 1.566) and QALYs were higher (∆0.141, 95% CI 0.008 to 0.274) compared with TSU, indicating Slim dominated. Results were robust against the price of biosimilars.
Conclusions The combination of MTX with a GC bridging scheme is less expensive with comparable health utility than more intensive step-down combination strategies or a conventional step-up approach 2 years after initial treatment.
Trial registration number NCT01172639.
- early rheumatoid arthritis
- DMARDs
- glucocorticoids
- cost-effectiveness
- QALY
Statistics from Altmetric.com
Key messages
What is already known about this subject?
While treat-to-target strategies are cost-effective in rheumatoid arthritis (RA), initial biological disease-modifying antirheumatic drug (bDMARD) therapy is not cost-effective and conventional synthetic DMARDs (csDMARDs) are to be preferred over bDMARDs or targeted synthetic DMARDs as first-line treatment.
What does this study add?
In patients with classical factors of poor prognosis, csDMARD combination therapy with step-down glucocorticoids (GCs) was not cost-effective compared with methotrexate (MTX) monotherapy also with step-down GCs within a remission induction strategy.
For patients without classical factors of poor prognosis, MTX plus a short-term course of GCs was clearly more cost-effective than the traditional MTX only.
How might this impact on clinical practice or future developments?
Initiating a step-down GC bridging combined with MTX in newly diagnosed patients with RA could be key to delay or even avoid use of second line expensive medication such as bDMARDs in both high-risk and low-risk patients.
Introduction
Insufficient control of disease activity in rheumatoid arthritis (RA) can lead to persistent pain, joint destruction, functional impairment and thus reduced health-related quality of life (QoL). Evidence suggests that controlling disease activity depends on early, intensive and to-target medical therapy.1 Therapy with conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) should be started as soon as possible after diagnosis, preferably methotrexate (MTX) and a short course of glucocorticoids (GCs).2 The ideal dosing scheme and the value of classical risk factors as therapeutic prognostics (theragnostic) are still a matter of debate. Over the years, several trials have demonstrated increased efficacy of initial csDMARD combinations over monotherapy, but evidence remains scarce for the superiority of combining csDMARDs within strategies including a step-down-bridge GC scheme. It has not been elucidated whether effectiveness of such strategies differs depending on prognostic risk profile.3–5 Care in early RA (CareRA), a randomised treat-to-target strategy trial showed no superiority of combinations of csDMARDs and bridging GCs (COBRA Classic or COBRA Avant-Garde) over MTX-only with a moderate-dose step-down GC bridging scheme (COBRA Slim), but COBRA Slim had a more favourable safety profile.6–8 In addition, COBRA Slim showed a better initial response and overall disease control than the traditional Tight-Step-Up (TSU) approach, starting MTX without oral GCs, in so-called low-risk patients.9
From a health economical point of view, it is important to investigate to what extent different initial treatment choices and consecutive treatment steps within a treat-to-target strategy lead to differences in longer-term costs. Therefore, we conducted a full economic evaluation of the CareRA trial to study the cost per quality-adjusted life years (QALYs).
Patients and methods
Using the 2-years data from the open label CareRA pragmatic treat-to-target randomised controlled trial (RCT) (EudraCT-number: 2008-007225-39), the incremental cost–utility and incremental net monetary benefit (iNMB) from a payer’s perspective were estimated. In the high-risk group, both COBRA Classic and COBRA Avant-Garde were compared with COBRA Slim. In the low-risk group, COBRA Slim was compared with TSU.
CareRA clinical trial
In total, 400 DMARD naïve patients with recently diagnosed RA (≤1 year) were assessed for eligibility between January 2009 and May 2013 and 379 were included.
Patients were stratified into a high-risk or low-risk group based on an algorithm with prognostic factors7 8 (erosions, rheumatoid factor (RF) or anticitrullinated cyclic peptide (anti-CCP) positivity and baseline Disease Activity Score in 28 joints with C-reactive protein (DAS28CRP)>3.2) and randomised into four different treat-to target schemes.
High-risk patients were randomised to one of the following initial treatment schemes:
COBRA Classic: 15 mg MTX weekly, 2 g sulfasalazine daily and a weekly step-down scheme of oral prednisone starting at 60 mg daily and tapering through 40-25-20-15-10-mg daily to a maintenance dose of 7.5 mg, with further tapering from week 28, before completely stopping at week 34.
COBRA Avant-Garde: 15 mg MTX weekly, 10 mg leflunomide (LEF) daily and a weekly step-down scheme of oral prednisone starting at 30 mg daily and tapering through 20–12.5-10-7.5 mg daily to a maintenance dose of 5 mg, with further tapering from week 28, before completely stopping at week 34.
COBRA Slim: 15 mg MTX weekly and a weekly step-down scheme of oral prednisone starting at 30 mg daily and tapering through 20–12.5-10-7.5 mg daily to a maintenance dose of 5 mg, with further tapering from week 28, before completely stopping at week 34.
Low-risk patients were randomised to either:
COBRA Slim.
TSU: 15 mg MTX weekly, no oral GCs allowed.
In all treatment arms, low disease activity (DAS28CRP ≤3.2) was used for steering treatment adaptations. The first trial year had prespecified (per-protocol) treatment adaptations. During the second year, adaptations were left at the discretion of the treating rheumatologist. An increase in the weekly MTX dose to 20 mg was the first adjustment in all treatment schemes. Next, the dose of the other csDMARD was increased in the combination arms (COBRA Classic and COBRA Avant-Garde) or 10 mg LEF was added in the non-combination arms (COBRA Slim and TSU). Further treatment changes could include bDMARD initiation according to Belgian reimbursement rules.10 Details on patient eligibility criteria, randomisation process, study design and treatment intensifications have been published.6–9 Patients were assessed at screening, baseline and then followed up at week 4, 8, 16, 28, 40, 52, 65, 78, 91 and 104. Optional visits, if clinically required, could be performed. Physicians filled out at every patient visit the electronic case record form (eCRF), comprising American College of Rheumatology core measures,11 medications and adverse events (AEs).
Outcomes
Health utility and QALYs
A health utility represents the preference of value attributed to a health state. It is expressed on a continuous scale from zero (equalling death) to one (full health). Scores can also be below 0 (states worse than death). By multiplying the utility value with years of survival, QALYs are calculated. For this study, QALYs were determined as the time-weighted average of reconstructed EuroQoL-5 Dimension (EQ-5D) values for each visit in the total follow-up (area under the curve). EQ-5D health utilities were reconstructed based on Health Assessment Questionnaire, age, pain on a Visual Analogue Scale and gender, using the validated UK algorithm of Hernández Alava et al.12–14 For patients experiencing AEs that were either severe or lasted for more than 3 months, the QALY was adjusted by a disutility, accounting for the duration of the AE. Based on an extensive literature search, disutilities per AE were constructed (online supplementary table 2).15–24 If no specific disutility was found, a general moderate-intensity treatment associated disutility (0.002) was applied.25
Supplemental material
Resource utilisation and direct healthcare costs
Healthcare costs in the economic analysis were rheumatology visits, RA-related medication (cs- and bDMARDs, GCs and all recorded analgesics including paracetamol, non-steroidals, tramadol and opioids), hospital admissions, laboratory and radiographs occurring during the 2-year trial.
Costs for rheumatology visits included scheduled and additional visits. Cost per visit was retrieved from the National Institute of Health and Disability Insurance (RIZIV) tariffs.26 RA-related medication costs were calculated from the eCRF reported medication name, dose, intake duration and frequency, then valued according to the Belgian Centre for Pharmacotherapeutic Information.27 Hospitalisation costs were calculated from AEs requiring hospitalisation and were price weighted depending on coded diagnosis (International Classification of Diseases, Ninth Revision, Clinical Modification), physician registered severity (mild, moderate, severe) and number of inpatient days with INAMI-RIZIV tariffs (tct.fgov.be).28 Supplemental costs for laboratory and radiographs were also incorporated.29 All prices were converted to 2018 euros using the general Belgian health index rate (statbel.fgov.be). Total costs per resource were calculated by multiplying the number of resources by the cost unit price extracted from Belgian national websites.26–29 Total costs per patient were obtained by summing costs of all resources. No discounting was considered due to the study’s short follow-up period (2 years).30
Cost-effectiveness analyses
This piggyback study, an economic evaluation alongside a clinical trial, follows the superiority design of CareRA and was performed on the intention-to-treat (ITT) population.
Differences in costs and QALYs between COBRA Classic and COBRA Avant-Garde compared with COBRA Slim for the high-risk group and between COBRA Slim and TSU for the low-risk group were analysed over 2 years. An incremental cost-effectiveness ratio (ICER) was calculated by dividing the cost difference by the QALY difference per pair of treatment schemes. The uncertainty analysis in the estimation of the ICER was plotted on cost-effectiveness planes (via non-parametric bootstrapping with 25 000 iterations of random sampling with replacement). Cost differences were depicted on the y-axis and QALY differences on the x-axis.
The incremental net monetary benefit (iNMB) of each comparison was calculated as iNMB=[incremental benefit * willingness to pay (WTP)]-incremental cost. The impact on the iNMB for varying thresholds of WTP (€0–€150 000) for one QALY gain was calculated. This reflects absolute economic gain (positive) or loss (negative), given how much society is willing to pay per QALY gained (ƛ). The World Health Organization proposes that it is reasonable to pay for an intervention that provides one additional year of healthy life per capita.31 An intervention is considered cost-effective when the cost for one QALY gained falls below three times the gross domestic product per capita (GDP) and highly cost-effective when below the GDP.32 In Belgium, no prespecified WTP exists, but the 2018 GDP was k€40.320.33 For this study, we used a WTP threshold (ƛ) of k€40 per QALY gained.
Considering the increased use of biosimilars, the base case analysis was repeated pricing bDMARDs at the lowest price of a biosimilar (Benepali) in Belgium (€153.15 for 50 mg weekly as of December 2018).
Sustained remission was used as an alternative health outcome to calculate the ICER. Sustained remission was defined as DAS28CRP <2.6 from week 16 to 104 at every visit.
Statistical analyses
Missing data were assumed to be missing at random and were imputed with multiple imputation (classification and regression trees) by chained equations.34 Missingness in clinical variables used to estimate utility, disease activity per time point, and total costs were imputed. Besides the incomplete variables, treatment strategy, centre of recruitment, age, gender, presence of comorbidities, AEs, RF, anti-CCP, erosions at baseline and trial completion were included as predictors in the matrix. Fifteen imputed datasets were created and analysed separately. Results of the 15 analyses were pooled using Rubin’s rules.35 36
For comparisons in complete cases, non-parametric Mann-Whitney U or Kruskal-Wallis and X2 bootstrapped-corrected were used when appropriate.
All analyses were performed with R V.3.6.1.
Results
Patients
Of the 379 patients included in the CareRA trial, 289 patients were stratified to the high-risk (COBRA Classic n=98, COBRA Avant-Garde n=93, COBRA Slim n=98) and 90 to the low-risk group (COBRA Slim n=43, TSU n=47). Patient characteristics in each treatment arm are presented in table 1. Good retention rates of up to 89% were observed (online supplementary figure 1). Missingness in the clinical variables over 2 years ranged from 12% to 39% per different time point and was 15% for total costs (n=328 for total cost).
Demographic and clinical characteristics at baseline per treatment scheme
Health outcomes
QALYs over 2 years were comparable in the high-risk group (1.551, 1.544, 1.553) between COBRA Classic, COBRA Avant-Garde and COBRA Slim, respectively (table 2). In the low-risk group, 2-year-QALYs were higher in COBRA Slim (1.629) compared with TSU (1.488), resulting in an incremental gain of 0.141.
Results of base-case and additional cost-effectiveness analyses comparing COBRA Classic and COBRA Avant-Garde to COBRA Slim in high-risk patients and COBRA Slim to TSU on low-risk patients (the last strategy being the comparator/reference scheme in every case)
Sustained remission rates (table 2) were also comparable in the high-risk group, whereas in the low-risk group COBRA Slim (42%) had better sustained remission rates than TSU (26%).
Healthcare use and costs
Healthcare costs in complete cases, including costs of medication, were presented in figure 1. The healthcare cost of rheumatology consultations and use of laboratory and X-rays was comparable across all schemes. In both high-risk and low-risk groups, differences in average cost per patient between treatment strategies could be attributed mainly to bDMARD use and hospitalisations (online supplementary table 1).

Costs across treatment schemes: mean € per patient and percentage (%) of the total cost in complete cost cases (n=328).
Combination arms (COBRA Classic and COBRA Avant-Garde) had a higher number of patients that were started on bDMARDs in the entire 2 years (online supplementary table 1), although not significant in all comparisons.
Total healthcare costs in the ITT population were for COBRA Classic (k€6.086), COBRA Avant-Garde (k€5.257) and COBRA Slim (k€4.622) in the high-risk group. In the low-risk group, costs were for COBRA Slim (k€4.007) and TSU (k€4.624).
Incremental cost per QALY
Given the higher costs and lower QALYs gained, COBRA Classic and COBRA Avant-Garde were dominated by COBRA Slim in the base-case analysis of the high-risk group (table 2). In the low-risk group, COBRA Slim also dominated TSU in view of the lower costs and higher number of QALYs gained (table 2). The sensitivity analyses considering biosimilar-prices for all bDMARDs yielded similar results (table 2).
Results from the 25 000 bootstrapped replications of the incremental cost–utility ratios for each comparison are presented in figure 2. In the high-risk group, COBRA Classic was more costly than COBRA Slim in 96% of the bootstrapped replications and was dominated by Slim in 68% of these replications (figure 2A). The bootstrapped uncertainty of COBRA Avant-Garde indicated this strategy to be more costly in 78% of replications compared with COBRA Slim (figure 2B) and in 56% of replications, this strategy was dominated. In the low-risk group, COBRA Slim dominated TSU (figure 2C) in 71% of the bootstrapped replications.

Cost-effectiveness planes of the base-case analysis (€/QALY). ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life-year; TSU, Tight-Step-Up; WTP, willingness to pay.
Incremental net monetary benefit per QALY
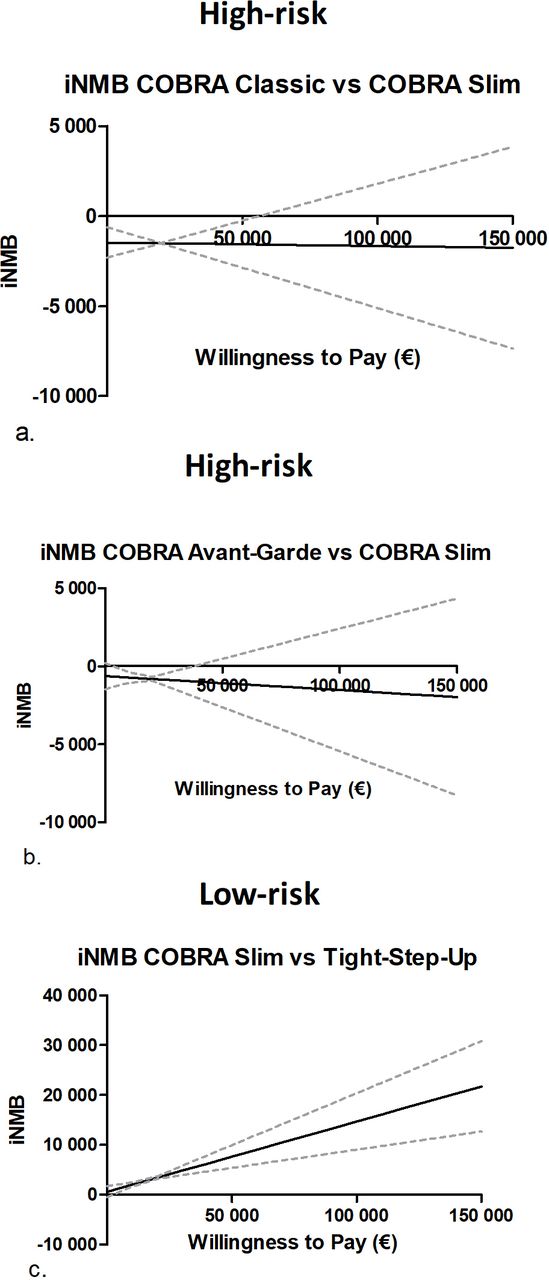
Figure 3 represents the iNMB per comparison of schemes at different thresholds for WTP from €0 to k€150 per QALY. In the high-risk group, when comparing COBRA Classic and COBRA Avant-Garde versus COBRA Slim, the iNMB estimate (black full line) was negative and remained below zero on the y-axis (figure 3A,B) regardless of the WTP. In other words, there was no economic benefit of choosing COBRA Classic or COBRA Avant-Garde over COBRA Slim. In the low-risk group, COBRA Slim versus TSU had a positive iNMB. COBRA Slim’s estimate never crossed the zero, indicating COBRA Slim was cost-effective even at a very low WTP range (figure 3C).
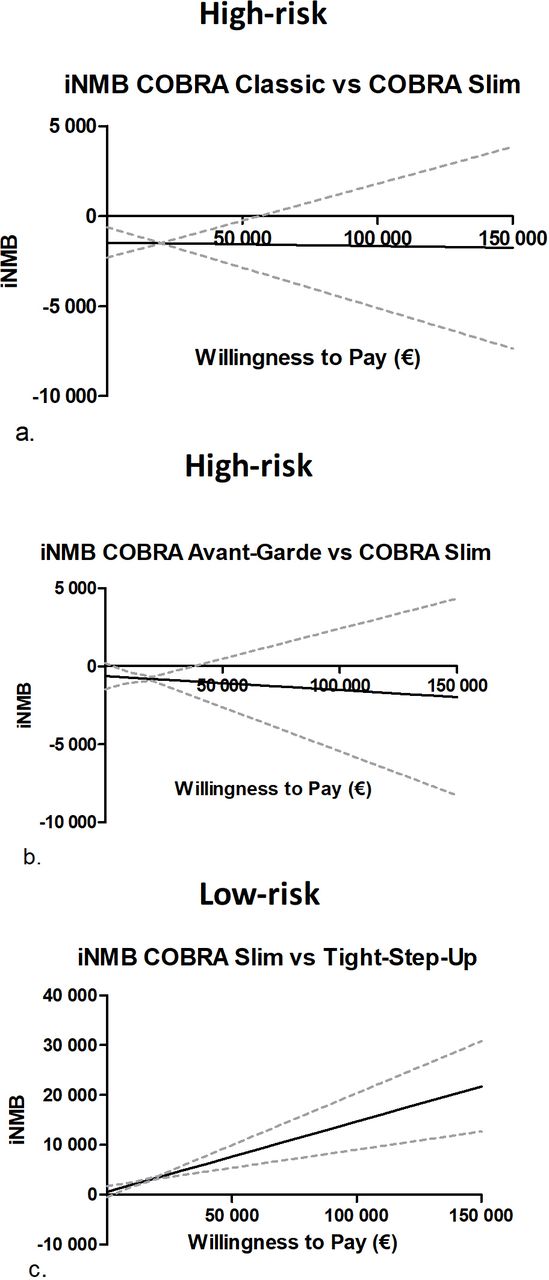
Mean incremental net monetary benefit (iNMB) with 95% CIs across different thresholds of willingness to pay (WTP) of the base-case cost–utility analyses with quality-adjusted life-years (QALYs) as health outcome. The black line is the estimate and the dotted lines its 95%CIs.
Incremental net monetary benefit per sustained remission
Figure 4 represents the iNMB per comparison of schemes at different thresholds for WTP from €0 to k€150 per sustained remission (DAS28CRP <2.6 from week 16 to 104). The iNMB approach represents the monetary benefit (in €) for each extra percentage (%) of patients that reached sustained remission at different WTP values. In the high-risk group, when comparing COBRA Classic versus COBRA Slim, the iNMB estimate (black full line) was negative and remained below zero on the y-axis (figure 4A). Regardless of the WTP, there was no economic benefit. When comparing COBRA Avant-Garde versus COBRA Slim, there was an added economic benefit from k€20 onwards. However, the lower CI remained negative at any WTP range (figure 4B). In the low-risk group, COBRA Slim was dominant to TSU with higher proportions of sustained remission at a lower cost, making it consistently beneficial across the WTP range (figure 4C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean incremental net monetary benefit (iNMB) with 95% CIs across different thresholds of willingness to pay (WTP) of the secondary analyses with sustained remission (DAS28CRP <2.6 from week 16 to 104) as health outcome. The black line is the estimate and the dotted lines its 95%CIs.
Discussion
This study showed that for high-risk early RA patients, csDMARD combination schemes with GCs (COBRA Classic and COBRA Avant-Garde) were not cost-effective or even dominated in the first 2 years when compared with COBRA Slim, MTX monotherapy together with a moderate-dose step-down GC bridging scheme, for initial remission induction within a treat-to-target strategy. In the low-risk group, COBRA Slim dominated the traditional MTX monotherapy without GC in patients with early RA treated-to-target. However, selecting the most appropriate first-line DMARD regimen remains a complex clinical decision.1
We published previously that COBRA Slim treatment resulted in similar remission rates but less therapy-related AEs compared with COBRA Classic or COBRA Avant-Garde.8 Such adverse drug events have been associated with higher costs of illness37 and also reduced patient’s QoL. This piggyback, trial-based economic evaluation, provides evidence that MTX with step-down GCs is an effective initial treatment choice for all patients with RA by balancing the necessary treatment intensity to control the disease with a favourable safety profile, resulting in an adequate QoL. This strategy could moreover minimise chances of an interruption or modification of the treatment scheme leading to more frequent discomfort and higher costs.
This study’s results were comparable to other cost-effectiveness analyses of early RA strategy trials. In the BeSt trial, the COBRA Classic-like strategy had a total cost of k€9.2 of which k€5.0 were direct medical costs (calculated from US dollars; exchange rate of 1:0.90),38 comparable to our cost of k€6.086 in COBRA Classic. In the COBRA-light trial, using strategies comparable to COBRA Classic and Slim, the total costs were k€9.7 and k€5.6, respectively, and differences in QALYs comparable to CareRA.39 The robust comparability with previous trials reinforces our message that COBRA Slim seems a cost-saving strategy.
In patients perceived as high-risk, the main driver for the lower cost of COBRA Slim was the lower number of bDMARDs initiated in the 2 years of the CareRA trial (online supplementary table 1). Because COBRA Classic and COBRA Avant-Garde combined two csDMARDs, patients insufficiently responding to these schemes were after failing to dose escalation of both csDMARDs eligible for bDMARDs according to Belgian reimbursement criteria.10 In contrast, patients on COBRA Slim therapy had to first initiate and fail a second csDMARD before being eligible for bDMARDs. In line with good clinical practice, this approach, including if necessary different adaptation steps depending on the initial treatment effect, delays the need for initiating bDMARDs, resulting in cost benefits but also potentially patient benefits, in terms of risk:benefit ratio.40 The long-term CareRA outcomes from the observational follow-up (3 years) will provide additional insights into cost-effectiveness and further bDMARD use.
Despite the fact that several trials and meta-analyses have demonstrated that efficacy outcomes improve when using tumour necrosis factor inhibitor (TNFi) bDMARDs as first-line treatment41 42 they have poor cost-effectiveness profiles.43 44 One of the challenges with these earlier analyses is that prices from before the approval of biosimilar TNFis were used for cost-effectiveness calculations. To estimate the hypothetical impact of using biosimilars in CareRA, an uncertainty analysis was performed changing every bDMARD to the lowest priced biosimilar in Belgium at the time of this study. This analysis demonstrated robustness of the initial results. To further explore the use of earlier bDMARD use, we initiated the CareRA 2020 trial (EudraCT # 2017-004054-41) examining the cost-effectiveness of accelerated but temporary bDMARD access after failing to MTX monotherapy with a GC bridging scheme.
Since pragmatic effectiveness trials seem best for economic studies, the use of data from the pragmatic CareRA study is a major strength for this economic analysis.45 As CareRA is a pragmatic, treat-to-target, multicentre investigator-initiated RCT with less stringent inclusion and exclusion criteria, the study population may represent a typical day-to-day healthcare population with no artificially enhanced compliance, using strategies already in place in clinical practice.46–48 The protocol-driven treatment adaptations were limited to two logical escalations of csDMARDs, meaning that when a bDMARD was needed, it was left at the discretion of the treating rheumatologist, just as in daily practice. However, this post hoc study of an RCT, provided no data on indirect costs nor direct non-medical costs. There might also be direct medical costs missing when it comes to general practitioner appointments and use of paramedical or alternative therapies. Intangible costs are complicated to account for, yet our study provides a glimpse into them by recreating the EQ-5D values considering pain and physical function among others. Moreover, the estimation of health utility was corrected for disutility produced by AEs.
Conclusion
Based on this economic analysis, compared with more intensive step-down combination strategies or to a conventional step-up approach, COBRA Slim, the combination of MTX and a moderate-dose GC bridging scheme, was less expensive and lead to comparable or better gain in QALYs. Therefore, we consider COBRA Slim a good starting strategy for all patients with early RA, irrespective of prognostic markers, in a treat-to-target setting.
Acknowledgments
We would like to show our gratitude to all participating patients, as well as to the investigators and medical staff at all sites. We appreciate the time invested. Furthermore, we are thankful for providing statistical advice to Robert Obenchain and Anikó Lovik, economical advice to Gonzalo Villa, data handling/processing advice to Ramiro Pazmino and proofreading to Geovanna Lucio.
References
Footnotes
Handling editor Josef S Smolen
Twitter @sophie_33pl
Contributors PV, RW, AB, SP and DDC made substantial contributions to the conception or design of the study. SP performed the statistical analysis. The manuscript was written by SP, PV, RW AB and DDC and subsequently revised critically by all the remaining coauthors. All authors were involved in data interpretation and approved the final version to be submitted for publication.
Funding The CareRA trial (EudraCT number: 2008-007225-39) was funded by a Flemish governmental grant (Agency for Innovation by Science and Technology (IWT)). Patrick Verschueren holds the Pfizer chair for early rheumatoid arthritis management at the KU Leuven.
Competing interests None declared.
Patient and public involvement statement The pragmatic CareRA protocol was strongly inspired by daily interactions of the investigators with RA patients in daily clinical practice. Patients were not formally involved in setting the research question or the outcome measures, nor were they invited to comment on study design or the interpretation of results of this manuscript. However, results of this research will be disseminated to study participants, all stakeholders and the general public in collaboration with patient organisations and the Belgian patient partners programme (trained patients who educate physicians, medicine students and other healthcare professionals in collaboration with a rheumatologist).
Patient consent for publication Not required.
Ethics approval The study was approved by the leading Ethics Committee of the University Hospitals Leuven after consulting the medical ethics committee of each participating centre (ref s51411).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. The authors commit to making the relevant anonymised patient data available for a specified purpose approved by the institution and the principal investigator of the CareRA study and with a signed data access agreement.