Article Text

Abstract
Objectives To gain expert-judgement-free insight into the Gestalt of axial spondyloarthritis (axSpA), by investigating its ‘latent constructs’ and to test how well these latent constructs fit the Assessment of SpondyloArthritis international Society (ASAS) classification criteria.
Methods Two independent cohorts of patients with early onset chronic back pain (SPondyloArthritis Caught Early (SPACE)) or inflammatory back pain (IBP) (DEvenir des Spondylarthopathies Indifférenciées Récentes (DESIR)) were analysed. Latent class analysis (LCA) was used to estimate the (unobserved) potential classes underlying axSpA. The best LCA model groups patients into clinically meaningful classes with best fit. Each class was labelled based on most prominent features. Percentage fulfilment of ASAS axSpA, peripheral SpA (pSpA) (ignoring IBP) or both classification criteria was calculated. Five-year data from DESIR were used to perform latent transition analysis (LTA) to examine if patients change classes over time.
Results SPACE (n=465) yielded four discernible classes: ‘axial’ with highest likelihood of abnormal imaging and HLA-B27 positivity; ‘IBP+peripheral’ with 100% IBP and dominant peripheral symptoms; ‘at risk’ with positive family history and HLA-B27 and ‘no SpA’ with low likelihood for each SpA feature. LCA in DESIR (n=576) yielded similar classes, except for the ‘no-SpA’. The ASAS axSpA criteria captured almost all (SPACE: 98%; DESIR: 93%) ‘axial’ patients, but the ‘IBP+peripheral’ class was only captured well by combining the axSpA and pSpA criteria (SPACE: 78%; DESIR: 89%). Only 4% of ‘no SpA’ patients fulfilled the axSpA criteria in SPACE. LTA suggested that 5-year transitions across classes were unlikely (11%).
Conclusion The Gestalt of axSpA comprises three discernible entities, only appropriately captured by combining the ASAS axSpA and pSpA classification criteria. It is questionable whether some patients with ‘axSpA at risk’ will ever develop axSpA.
- axial spondyloarthritis
- diagnosis
- classification criteria
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Axial spondyloarthritis (axSpA) is a disease that is difficult to diagnose; its Gestalt is more than only a collection of SpA features included in the Assessment of SpondyloArthritis international Society (ASAS) axSpA classification criteria.
The ASAS axSpA criteria may suffer from inappropriate circular reasoning because they were developed against expert’s opinion.
What does this study add?
An analytical technique that circumvents expert opinion (latent class analysis) was used to determine, in a circularity-free manner, the Gestalt of axSpA and yielded three recognisable clinical entities labelled as: ‘pure axial SpA’, ‘axial SpA with peripheral signs’ and ‘axial SpA at risk’.
‘Pure axial SpA’ represents the conventional clinical picture of axSpA and is well captured by the ASAS axSpA criteria, but patients with ‘axial SpA with peripheral signs’ mostly fulfil the peripheral SpA (pSpA) criteria, suggesting a larger overlap between axSpA and pSpA than anticipated when the ASAS criteria were developed.
The ‘axial SpA at risk’ entity (often captured by the ASAS axSpA criteria) is a ‘grey zone’ entity based on the presence of risk factors for axSpA and may encompass individuals that do neither have SpA nor will ever develop it.
How might this impact on clinical practice or future developments?
Patients with ‘axial SpA with peripheral signs’ are not necessarily recognised as axSpA and therefore not included in axSpA trials; ‘at risk’ patients, on the contrary, may be overdiagnosed and overtreated, especially if classification criteria are misused for diagnostic purposes.
Introduction
Spondyloarthritis (SpA) encompasses heterogeneous entities with common clinical, laboratory and imaging features. The full spectrum of SpA includes patients with dominant axial symptoms (axial SpA (axSpA)) and patients with dominant peripheral symptoms (peripheral SpA (pSpA)).1 The term axSpA aggregates patients with radiographic axSpA (r-axSpA; also known as ankylosing spondylitis) and non-radiographic axSpA (nr-axSpA), differing only by the presence of radiographic sacroiliitis in the former, as defined by the modified New York (mNY) criteria.2
axSpA is a syndrome described by classification criteria that supposedly best reflect its inherently unmeasurable ‘latent’ construct (Gestalt). The Assessment of SpondyloArthritis international Society (ASAS) criteria for axSpA have been developed to classify both r-axSpA and nr-axSpA. In the absence of a ‘gold standard’, expert opinion has been used as an external ‘anchor’ to develop and validate classification criteria.3–5 The ASAS criteria outperform other criteria,6 meaning that they contain several elements that experts consider relevant for their ‘latent’ picture of axSpA.
While such an approach for developing classification criteria has been pursued by default in rheumatology, it has a fundamental limitation that may jeopardise their construct and content validity: circularity. If criteria are developed against expert opinion, and the expert finds certain characteristics (eg, inflammation on MRI of the sacroiliac joints (SIJ)) more important than others, such characteristics may be awarded a too prominent place in the criteria. Subsequent cross-validation against an expert diagnosis may produce results driven by experts’ beliefs rather than on an objective presence of axSpA. The axiom that ‘early (diagnosis and treatment) is always better’, a dominant view in modern rheumatology, may have contributed to rheumatologists’ beliefs and as such trickled down into the ASAS criteria, designed to better capture patients with early disease. When classification criteria are (mis)used in a diagnostic context, overdiagnosis, followed by overtreatment, is a logical consequence.7
A more circularity-free determination of the Gestalt of axSpA is lacking in the literature, which hampers the study of the side effects of overdiagnosis and overtreatment. Here, we propose to evaluate the Gestalt of axSpA using an analytical approach that excludes the rheumatologist’s diagnostic opinion. Our aims were twofold: (i) to gain an expert-judgement-free insight, into the concept of axSpA, by investigating its ‘latent constructs’ and (ii) to evaluate how well the ASAS SpA classification criteria capture these ‘latent constructs’.
Methods
Patients and study design
Baseline data from the SPondyloArthritis Caught Early (SPACE) cohort and baseline and 5-year data from the DEvenir des Spondylarthopathies Indifférenciées Récentes (DESIR) were used. Both cohorts have been previously described in detail.6 8 Briefly, in SPACE (ongoing multinational cohort), consecutive patients aged ≥16 years with chronic back pain (≥3 months, ≤2 years and onset <45 years) are included. In DESIR, consecutive patients aged 18–50 years with inflammatory back pain (IBP) (>3 months but <3 years), and for whom the treating rheumatologist considers the symptoms suggestive of axSpA (level of confidence (LoC) ≥5, scale 0–10), were included. Databases were locked in October 2017 (SPACE) and June 2016 (DESIR).
SpA features
The following features were collected in each cohort: HLA-B27, elevated C reactive protein (CRP) (≥6 mg/L), family history of SpA (ASAS definition),5 good response to non-steroidal anti-inflammatory drugs (NSAIDs), peripheral arthritis, heel enthesitis, dactylitis, psoriasis, inflammatory bowel disease, acute anterior uveitis and IBP.
At baseline, SpA features were considered positive if ‘ever present’ (ie, any time in the past and/or baseline) in both cohorts, except dactylitis (available only as ‘current’ in SPACE). In DESIR, data on SpA features were also collected every 6 months up to 2 years and yearly thereafter up to 5 years. Change in time-varying features was defined as ‘once-a-feature-always-a-feature (OFAF)’: patients positive at baseline remained positive at 5 years, even if becoming negative or missing in between; patients negative at baseline, remained negative at follow-up if no switch to positive or if missing in between. A feature changed to positive if appearing anytime during follow-up.
Radiographs and MRIs of the SIJ (X-SIJ; MRI-SIJ) and spine (X-Spine; MRI-Spine) were obtained at baseline in both cohorts, and at 2 and 5 years in DESIR. Each image was independently scored, by three trained central readers in each cohort, blinded to chronology, clinical data and to the results of other modalities. Four binary imaging features, defined by agreement between ≥2 out of 3 readers, were assessed: inflammation on MRI-SIJ (ASAS definition)9 10; bone marrow oedema (BME) on MRI-Spine (≥5 lesions)11; definite structural damage in X-SIJ according to the mNY criteria2 and ≥1 syndesmophyte in X-Spine.12
Statistical analysis
Latent class analysis (LCA) was performed with baseline data of each cohort separately, including patients with complete data on all features. LCA unmasks a ‘latent’ (ie, unobserved) construct (here: Gestalt of axSpA) by splitting patients into mutually exclusive classes based on the covariance of observed SpA features. Extensive evidence supports the superiority of LCA in identifying latent data structures, compared with other clustering methods.13–15 SpA features (15 variables in SPACE; 14 in DESIR (excluding IBP)) were selected ‘a priori’ based on content knowledge without predefined weights.
A detailed description LCA and how it can be used to identify the latent classes of the Gestalt of axSpA is provided in online supplementary text S1. Briefly, the number of classes was increased, one-by-one, until the best model was found, defined by: best goodness of fit assessed by Akaike’s information criterion, Bayesian information criterion (BIC), sample-sized adjusted BIC, entropy, likelihood ratio test (comparing the model with the one with n-1 classes) and by clinically recognisable patterns within each class (ie, a statistical criterion alone does not suffice). The classes of the final model were interpreted according to the probability of each feature and labelled as a clinically recognisable entity. Features were defined as: across-class dominant (highest probability across classes); within-class dominant (probability >50% within each class) and not dominant across or within classes.
Supplemental material
Maximum likelihood estimates were used to classify individual patients based on their posterior probability of class membership. This allowed us to describe the classes including also variables not used in the models and to evaluate the percentage of patients within each class fulfilling the ASAS axSpA, pSpA (ignoring IBP) and the SpA criteria (ie, combination of either axSpA or pSpA criteria) at baseline.
To address between-cohort differences in study design, a sensitivity analysis was performed in SPACE: only in patients with a rheumatologist’s diagnosis with LoC ≥5 (similar to DESIR).
Latent transition analysis (LTA) was used to estimate the likelihood of change across classes after 5 years in DESIR.16 LTA includes the same patients and variables as in LCA. The number of classes best fitting the baseline and 5-year LCA formed the basis of the LTA model. Classes at baseline and follow-up can be assumed as: having the same meaning (full invariance); different meaning (full non-invariance) or the same meaning for some and different for others (partial invariance). The final LTA model has the number of classes at baseline and 5 year and class-(in)variance that best fits the data provided it is clinically meaningful.
LCA was performed in Stata V.15.1. LTA was performed in MPlus V.7.
Results
Baseline characteristics
In total, 465 patients from SPACE and 576 from DESIR were included. In SPACE, included patients were more likely to be HLA-B27 positive (57% vs 37%) and less likely to have BME on MRI-SIJ (14% vs 30%) than those excluded (n=283). No differences were seen in DESIR (excluded: n=132) (online supplementary tables S1 and S2). Baseline characteristics of the included patients from both cohorts are shown in table 1. Patients from DESIR had, on average, more SpA features compared with those from SPACE, including peripheral features (eg, heel enthesitis 45% vs 20%) and axial imaging abnormalities (eg, sacroiliitis on MRI-SIJ 27% vs 14%).
Baseline patient characteristics in the SPACE and DESIR cohorts
Latent class analysis in SPACE and DESIR
A 4-class (SPACE) and a 3-class (DESIR) LCA model fitted the data best (table 2). The additional class in the 5-class (SPACE) and 4-class (DESIR) models, with worse model fit, did not yield a clinically recognisable pattern (online supplementary tables S3, S4 and S5).
Final latent class analysis (LCA) models in SPACE (n=465) and DESIR (n=576) in probability scale (range: 0–1)
The final LCA models are shown in table 2. In SPACE, class 1 was characterised by highest likelihood (ie, across-class dominance) of lesions present on axial imaging, elevation of CRP and HLA-B27 positivity, and was labelled as ‘axial’. Class 2 was labelled ‘IBP+peripheral’, given the 100% likelihood of IBP and across-class dominance of peripheral features. Class 3 had across-class dominance of positive family history (71%) and within-class dominance of HLA-B27 positivity (69%) and IBP (66%) but low likelihood of other features and was labelled as ‘at risk’. Class 4 was labelled ‘no SpA’ given the very low likelihood for each SpA feature.
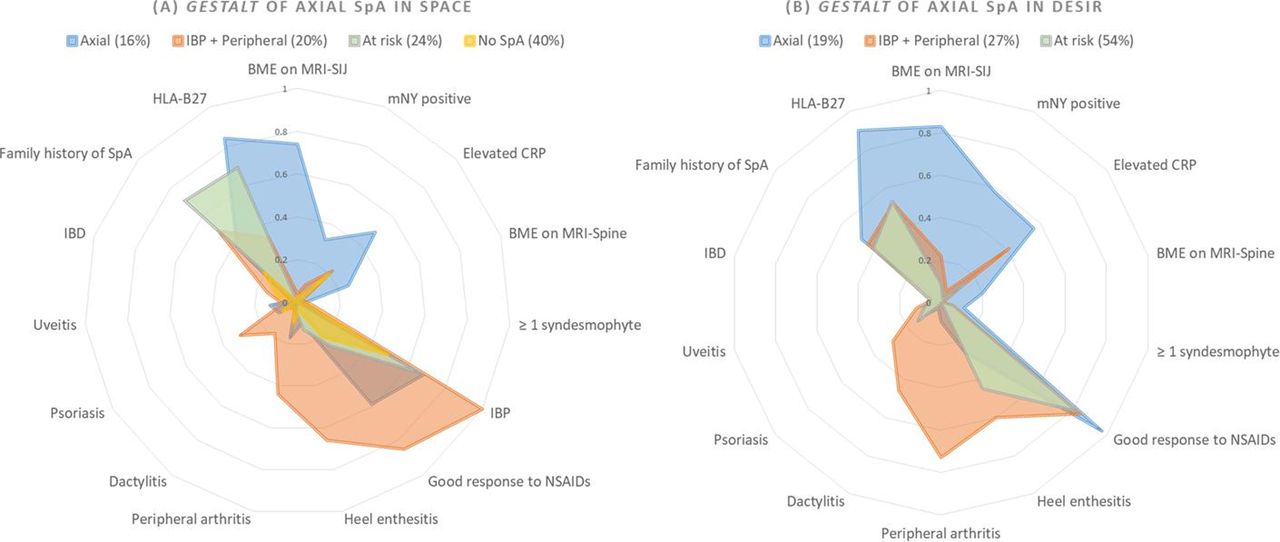
The LCA analysis in DESIR yielded the same latent classes, except ‘no SpA’, and an overlapping pattern of dominance: among 42 possible comparisons (14 features (excluding IBP) multiplied by 3 classes (excluding ‘no SpA’)), in 37 (88%) the dominance pattern was similar to SPACE (table 2). Figure 1 graphically displays the between-cohort similarities, and also the phenotypical differences between the ‘axial’ and ‘IBP+peripheral’ classes which overlap with the ‘at risk class’ only partially, and even less with the ‘no SpA’ class.

Radar charts showing the distribution of the probabilities of each feature according to the final LCA model in (A) SPACE and (B) DESIR. BME, bone marrow edema; CRP, C reactive protein; DESIR, DEvenirdes Spondylarthopathies Indifférenciées Récentes; IBD, inflammatory bowel disease; IBP, inflammatory back pain; mNY, modified New York criteria; NSAIDs, non-steroidal anti-inflammatory drugs; SIJ, sacroiliac joints; SPACE, SPondyloArthritisCaught Early; MRI-SIJ, magnetic ressonance imaging of the sacroiliac joints; MRI-Spine, MRI of the spine.
The LCA model in SPACE, in patients with a rheumatologist’s diagnosis of axSpA (LoC ≥5) (n=202) yielded the same classes as the main model, except ‘no SpA’ that is similar to DESIR (‘axial’: 29%; ‘IBP+peripheral’: 33%; ‘at risk’:38%; online supplementary table S6).
Latent transition analysis in DESIR
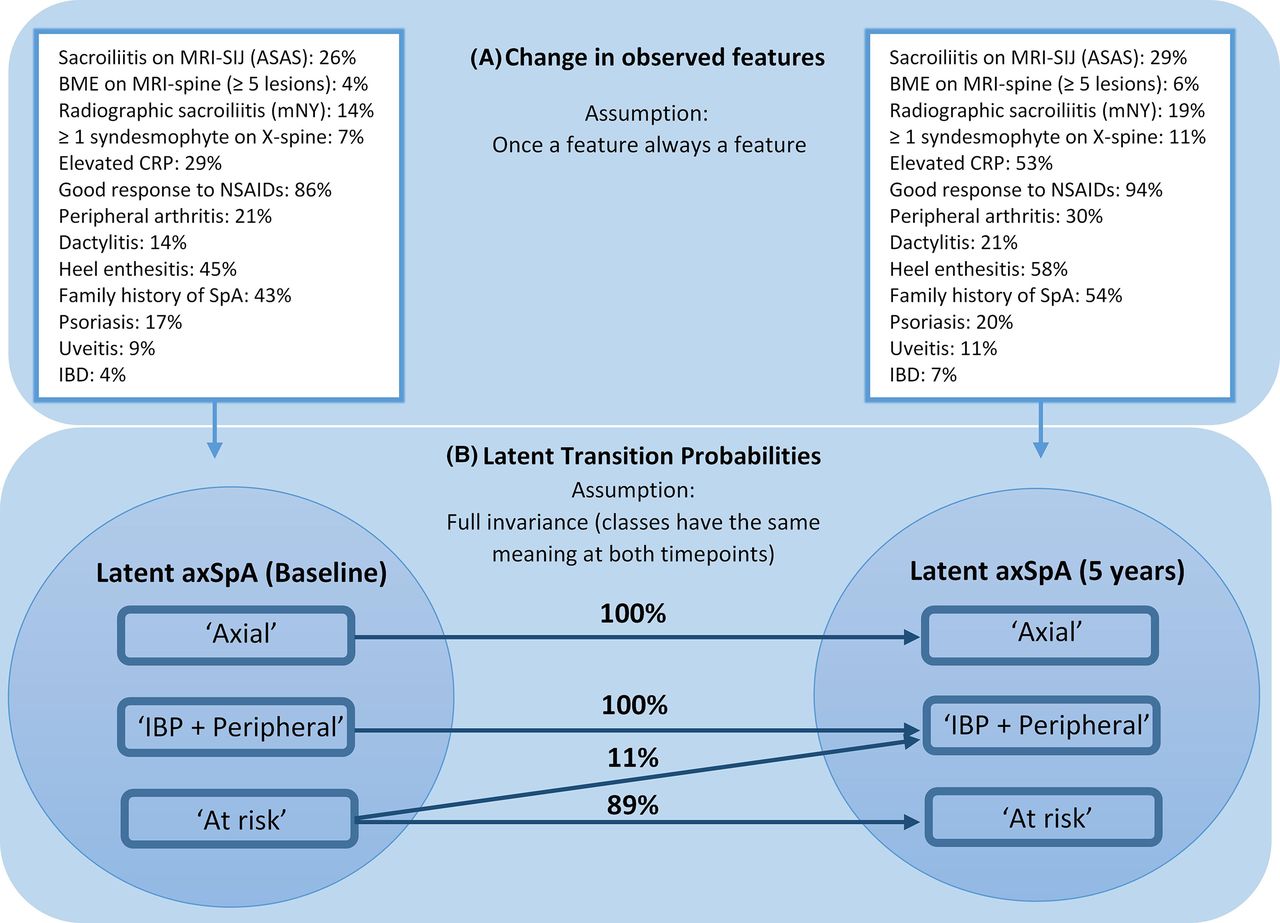
Of the 576 patients in DESIR, 500 (87%) completed the 5-year follow-up. The change in SpA and imaging features between baseline and 5 years is shown in figure 2A. Because of how SpA features were defined (OFAF), all increased in prevalence over time, but changes were more pronounced with peripheral (eg, peripheral arthritis: 21%–30%) than with imaging features (eg, BME on MRI-SIJ: 26%–29%).

{kind=link}
{kind=link}
Final latent transition analysis (LTA) model (with full invariance*) in DEvenirdes Spondylarthopathies Indifférenciées Récentes (n=576). (A) Squares refer to observed (ie, measurable) variables and (B) Circles refer to latent (ie, unobserved) variables. Arrows: latent transition analysis models the change in observed features (A) to estimate the latent (B) transition probabilities between classes from baseline to 5 years. ASAS, Assessment of SpondyloArthritis international Society; axSpA, axial spondyloarthritis; BME, bone marrow edemao; CRP, C reactive protein; IBD, inflammatory bowel disease; IBP, inflammatory back pain; LTA, latent transition analysis; mNY, modified New York criteria; NSAIDs, non-steroidal anti-inflammatory drug; SIJ, sacroiliac joints; X-Spine, radiograph of the spine MRI, magnetic ressonance imaging. *Selection of final LTA model according to goodness of fit detailed in online supplementary table S9 and full final model in online supplementary table S10.
Similar to baseline LCA, a 3-class model at 5 years best fitted the data (online supplementary table S7 and S8). Accordingly, an LTA model with three classes at both timepoints was fit. Although the model fit (online supplementary table S9) was better with partial invariance, the resulting model did not yield a clinically recognisable pattern (data not shown), so the simplest assumption (full invariance) was taken to define the final LTA model (figure 2b, online supplementary table S10). LTA revealed a 0% probability of switch from the ‘axial’ and ‘IBP+peripheral’ to another class. ‘At risk’ patients at baseline had 11% likelihood to change to ‘IBP+peripheral’ over 5 years.
Observed characteristics and fulfilment of the ASAS classification criteria
The patterns of observed characteristics per latent class in SPACE and DESIR were, expectedly, similar to the model-based estimates (table 3). In addition, across-class dominance of males in the ‘axial’ class (SPACE: 66%; DESIR: 73%), and current arthritis/enthesitis/dactylitis (ie, entry criterion for pSpA criteria) in the ‘IBP+peripheral class (SPACE: 87%; DESIR: 88%) were observed.
Baseline observed patient and disease characteristics per latent class in SPACE and DESIR
The ASAS axSpA criteria captured almost all patients from the ‘axial’ class in SPACE (63/64; 98%). This percentage was much lower with ‘IBP+peripheral’ (41/92; 49%), and missed patients were most often female (78%), positive for current arthritis/enthesitis/dactylitis (92%) and HLA-B27 and MRI-SIJ/mNY negative. The pSpA criteria captured 67% of the ‘IBP+peripheral’ patients and this figure was 78% when the axSpA and pSpA criteria were combined. Fifty-nine (60%) patients from the ‘at risk’ class fulfilled the axSpA criteria (58/59=98% fulfilling the ‘clinical arm only’). Among the 58 fulfilling the ‘clinical arm only’, family history of SpA (75%) and IBP (85%) were the most common features. Only nine patients (4%) from the ‘no SpA’ class fulfilled the axSpA criteria, all of which captured by the imaging arm only (78% positive for IBP or good response to NSAIDs). Results were similar in DESIR, except that the percentage of ‘at Risk’ patients fulfilling the ‘clinical arm only’ was somewhat lower (148/177=84%).
Discussion
Using a data-driven approach, we identified three separate clinical entities, remarkably stable over time, together forming the Gestalt of axSpA, in two independent cohorts, that we labelled ‘pure axial SpA’ (‘axial’), ‘axial SpA with peripheral signs’ (‘IBP+peripheral’) and ‘axial SpA at risk’ (‘at risk’). In SPACE, a cohort that includes patients with back pain without axSpA, these three axSpA classes decently discerned themselves from a fourth labelled as ‘no SpA’. This adds to the credibility of our data, since the absence of ‘no SpA’ in DESIR was expected based on enrolment criteria. The ASAS axSpA classification criteria captured almost entirely the ‘axial’ class but missed several patients from the ‘IBP+peripheral’ class: the latter is better captured when combining the axSpA and pSpA criteria, suggesting a larger overlap between axSpA and pSpA than previously thought, when the ASAS criteria were developed. Taken together, at the group level these results confirm the robustness of the classification criteria. The ‘at risk’ class is an entity characterised by the presence of presumed risk factors for axSpA but the absence of objective clinical signs. While these patients often fulfil the ASAS axSpA classification criteria, it is likely that some do not actually have or will ever develop axSpA. Overdiagnosis of axSpA in the 50% of patients in this class is likely if classification criteria are ticked for diagnosis.
A diagnosis of axSpA is challenging and should rely on thorough knowledge and recognition of ‘the appropriate pattern’.17 18 The rheumatologists’ perception of the ‘SpA pattern’ evolved over the last 40 years as a result of efforts by the international rheumatology community. Initially, only r-axSpA (ankylosing spondylitis) was recognised and classified by the mNY criteria.2 In the 70s–80s, Moll and Wright defined SpA as a group of entities with common features,19 and the Amor and the European Spondyloarthropathy Study Group (ESSG) classification criteria were proposed.20 21 Both criteria sets capture the broader ‘SpA pattern’ by combining axial and peripheral features and do not distinguish between patients with dominant axial and dominant peripheral patterns. Since then, evidence has emerged supporting that patients with the axial and peripheral pattern may respond differently to treatment,22 23 and that not all patients with axSpA will develop sacroiliitis on pelvic radiographs (mNY-positive). When they do, this is frequently a late and unreliable finding and often preceded by sacroiliitis on MRI-SIJ for many years.24–31 Such evidence prompted ASAS experts to develop classification criteria for patients with predominant axial involvement,5 also capturing those that are mNY-negative (nr-axSpA) as axSpA, and for patients with predominant peripheral involvement that—if combined—enclose the entire Gestalt of SpA according to experts.4
The ASAS axSpA and pSpA classification criteria were validated against an external ‘gold standard’: expert opinion.3–5 Extensive evidence supports that the ASAS criteria perform well against this anchor,32 but misclassification remains a matter of intense debate.33 It has been argued that expert opinion may have contributed to designing criteria that encompass circular reasoning,34 35 that is, features deemed important by experts, especially those that allow early detection (eg, sacroiliitis on MRI), were awarded a too prominent place in criteria that were subsequently again validated by experts. However, whether or not circularity has played a decisive role remains unclear, since an expert-judgement-free assessment of the Gestalt of axSpA has not been pursued so far. This is exactly what we have done in this study.
Using LCA we could describe the Gestalt of axSpA without any pre-assumptions on the contribution (‘weight’) of each SpA feature. This was only possible because LCA, following selection of parameters for analysis, does not need interpretational input from experts, whose beliefs therefore do not influence the analysis. The only inevitable influence experts potentially had was deciding if the patient should be included in the cohort. One of the phenotypes that arose from this analytical framework was a syndrome characterised by a high likelihood of axial imaging abnormalities, HLA-B27 positivity and male dominance, which we have subsequently labelled as ‘axial’. This phenotype closely resembles the rheumatologist’s conventional clinical picture of axSpA. Of note, LCA did not distinguish nr-axSpA from r-axSpA, even after forcing one additional class to the model. This is in line with extensive evidence suggesting that the split of axSpA in nr-axSpA and r-axSpA is artificial and supports the view that both are part of the same disease spectrum.1 26 36 37
However, the ‘axial’ class is only one part of the Gestalt of axSpA: we identified a separate phenotype, defined by the presence of IBP (100%) in close conjunction with peripheral signs and symptoms (‘IBP+peripheral’). These patients with axSpA (mostly female) had back pain but were unlikely to be positive for sacroiliitis on imaging and HLA-B27. Thus, these patients rather fulfilled the pSpA than the axSpA classification criteria since the latter require either positive imaging (‘imaging arm’) or HLA-B27 (‘clinical arm’). Formally, the ASAS pSpA criteria could not have been applied, since all patients had IBP.4 We ignored this rule to better understand the possible overlap between SpA with predominantly peripheral features (original ‘target’ of the pSpA criteria) and axSpA with peripheral signs (the entity described here). The high percentage of ‘IBP+peripheral’ patients fulfilling the pSpA criteria argues in favour of a significant overlap. This is in line with another study in DESIR, in which a different analytical approach (cluster analysis) was pursued that, unlike LCA, assumes an a priori presence of subgroups.38 Taken all together, our findings undermine the current stand that either sacroiliitis on imaging or presence of HLA-B27 is mandatory to classify patients as axSpA. Several (female) patients presenting with IBP and concomitant peripheral manifestations but without manifest sacroiliitis or HLA-B27 are not recognised as axSpA and therefore not included in axSpA trials. These patients have consistently shown to have significant burden of disease.38–41 Whether or not these patients truly have inflammatory SpA or rather a chronic pain syndrome is a question that cannot be resolved by this analysis.
A third phenotype we identified is based on the presence of risk factors for axSpA (ie, positive family history and HLA-B27) in association with IBP and only sporadically other SpA features. We have labelled this phenotype axSpA ‘at risk’. Here, ‘at risk’ means that patients present with features suggestive of axSpA, but such a diagnosis is not beyond any doubt. In other words, the ‘at risk’ class implies a higher level of uncertainty (grey zone) than the other classes, such as the ‘axial’ and the ‘IBP+peripheral’ classes. Too often, when dealing with uncertain or difficult cases clinicians apply classification criteria to inform binary diagnostic judgements (eg, axSpA vs no axSpA) that do not allow grey zones. In addition, the anchoring features of this class (ie, family history and HLA-B27) have shown redundancy,42 but yet count separately for classification, which may contribute to overcalling axSpA when the ASAS axSpA criteria are wrongly used for diagnostic purposes. The high likelihood of IBP in these patients does not further help in discriminating SpA and no-SpA, since it also occurs in half of the patients of the ‘no SpA’ class. This is in line with recent data suggesting that specificity of IBP is lower than previously thought.43 44 Although a longer follow-up may reveal more across-class switches over time, the low likelihood of ‘at risk’ patients to switch to a more profound phenotype within 5 years adds to the notion that ‘at risk’ patients may not have ‘real’ axSpA and will most often also not develop it later. A logical consequence would be to refrain from treating them as if they really have axSpA and from including these ‘at risk’ patients in axSpA trials which is indeed done as in addition to fulfilment of the ASAS criteria objective signs of inflammation are required.
In summary, we identified three latent phenotypes of the Gestalt of axSpA with a method that largely circumvents the circularity by expert opinion. ‘Pure axial SpA’ is the ‘classical’ phenotype of axSpA. ‘axSpA with peripheral signs’ is a recognisable phenotype in the spectrum of patients presenting with chronic back pain, best captured by the pSpA criteria suggesting that the overlap between axSpA and pSpA is larger than anticipated. The ‘at risk’ class is the least well-defined of all entities and may encompass individuals at risk of axSpA, but without fully established disease, and also individuals who do not have SpA or will ever develop it. Studies addressing the prognosis of these subphenotypes, especially that of the ‘at risk’ class, should inform us better on the real outcome of axSpA.
Acknowledgments
The authors would like to thank all patients who participate(d) in the SPACE cohort, and the physicians who contributed to the data collection. The authors would like to thank the different participating centres: Pr Désirée van der Heijde and Dr Floris van Gaalen (Leiden University Medical Center, Leiden, The Netherlands); Pr Robert Landewé and Dr Marleen van der Sande (Amsterdam University Medical Center, Amsterdam, The Netherlands); Dr Maikel van Oosterhout (Groene Hart Ziekenhuis Hospital, Gouda, The Netherlands); Dr Inger Jorid Berg (Diakonhjemmet Hospital, Oslo, Norway); Pr Roberta Ramonda (University of Padova, Padova, Italy); Pr Lennart Jacobsson (University of Gothenburg, Gothenburg, Sweden). The authors would also like to thank the different regional participating centres in DESIR: Pr Maxime Dougados (Paris-Cochin B), Pr Andre Kahan (Paris-Cochin A), Pr Philippe Dieudé (Paris-Bichat), Pr Bruno Fautrel (Paris-La Pitie-Salpetriere), Pr Francis Berenbaum (Paris-Saint-Antoine), Pr Pascal Claudepierre (Creteil), Pr Maxime Breban (Boulogne-Billancourt), Dr Bernadette Saint-Marcoux (Aulnay-sous-Bois), Pr Philippe Goupille (Tours), Pr Jean Francis Maillefert (Dijon), Dr Emmanuelle Dernis (Le Mans), Pr Daniel Wendling (Besancon), Pr Bernard Combe (Montpellier), Pr Liana Euller-Ziegler (Nice), Pr Pascal Richette (Paris Lariboisiere), Pr Pierre Lafforgue (Marseille), Dr Patrick Boumier (Amiens), Pr Martin Soubrier (Clermont-Ferrand), Dr Nadia Mehsen (Bordeaux), Pr Damien Loeuille (Nancy), Pr Rene-Marc Flipo (Lille), Pr Alain Saraux (Brest), Pr Xavier Mariette (LeKremlin-Bicetre), Pr Alain Cantagrel (Toulouse), Pr Olivier Vittecoq (Rouen). The authors would also like to thank the research nurses, the staff members of the Clinical Research Unit of Paris Centre, the staff members of the Biological Resource Center of Bichat Hospital, the staff members of the Department of Statistics of Nımes and all the investigators and in particular Jerome Allain, Emmanuelle Dernis, Salah Ferkal, Clement Prati, Marie-Agnes Timsit, Eric Toussirot for active patient recruitment and monitoring.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Twitter @AlexSepriano, @sofiaramiro82, @annamolto
Contributors AS, SR, DvdH and RBML designed the study. AS performed the statistical analyses. AS wrote the first draft of the manuscript. All authors critically interpreted the results, reviewed the draft version and approved the final manuscript.
Funding The DESIR study is conducted as a Programme Hospitalier de Recherche Clinique with Assistance Publique Hopitaux de Paris as the sponsor. The DESIR study is also under the umbrella of the French Society of Rheumatology, which financially supports the cohort. An unrestricted grant from Pfizer has been allocated for the first 10 years. The DESIR cohort is conducted under the control of Assistance publique Hopitaux de Paris via the Clinical Research Unit Paris Centre and under the umbrella of the French Society of Rheumatology and Institut national de la sante et de la recherche medicale (Inserm). Database management is performed within the Department of Epidemiology and Biostatistics (Professeur Jean-Pierre Daures, D.I.M., Nımes, France). AS is supported by a doctoral grant from 'Fundação para a Ciência e Tecnologia' (SFRH/BD/108246/2015).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was conducted according to Good Clinical Practice guidelines and approved by the appropriate local ethical committees. Written informed consent was obtained from participating patients before inclusion.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.