Article Text

Abstract
Objective To assess the safety and efficacy of rituximab in systemic sclerosis (SSc) in clinical practice.
Methods We performed a prospective study including patients with SSc from the European Scleroderma Trials and Research (EUSTAR) network treated with rituximab and matched with untreated patients with SSc. The main outcomes measures were adverse events, skin fibrosis improvement, lung fibrosis worsening and steroids use among propensity score-matched patients treated or not with rituximab.
Results 254 patients were treated with rituximab, in 58% for lung and in 32% for skin involvement. After a median follow-up of 2 years, about 70% of the patients had no side effect. Comparison of treated patients with 9575 propensity-score matched patients showed that patients treated with rituximab were more likely to have skin fibrosis improvement (22.7 vs 14.03 events per 100 person-years; OR: 2.79 [1.47–5.32]; p=0.002). Treated patients did not have significantly different rates of decrease in forced vital capacity (FVC)>10% (OR: 1.03 [0.55–1.94]; p=0.93) nor in carbon monoxide diffusing capacity (DLCO) decrease. Patients having received rituximab were more prone to stop or decrease steroids (OR: 2.34 [1.56–3.53], p<0.0001). Patients treated concomitantly with mycophenolate mofetil had a trend for better outcomes as compared with patients receiving rituximab alone (delta FVC: 5.22 [0.83–9.62]; p=0.019 as compared with controls vs 3 [0.66–5.35]; p=0.012).
Conclusion Rituximab use was associated with a good safety profile in this large SSc-cohort. Significant change was observed on skin fibrosis, but not on lung. However, the limitation is the observational design. The potential stabilisation of lung fibrosis by rituximab has to be addressed by a randomised trial.
- systemic sclerosis
- rituximab
- lung fibrosis
- skin fibrosis
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Some efficacy of rituximab in systemic sclerosis (SSc) has been suggested by few small-sized uncontrolled studies. Large controlled studies were lacking.
What does this study add?
Rituximab is safe in SSc.
Treatment with rituximab improves skin fibrosis, which is a marker of disease activity and severity as compared with untreated control-patients.
No significant change was observed on lung fibrosis in the whole cohort.
Secondary analyses suggest that combination therapy with mycophenolate mofetil might be more effective for treating lung fibrosis.
How might this impact on clinical practice or future developments?
A clue for the future to get a better impact on SSc outcomes might be combination therapy, which should be further studied.
Introduction
Systemic sclerosis (SSc) is an orphan disease that is characterised by fibrosis of the skin and internal organs, autoimmunity and vasculopathy.1 SSc has the highest cause-specific mortality among connective tissue diseases.2 Progressive interstitial lung disease (ILD) is the leading cause of death in SSc.3 Despite the fatal burden associated with this condition, treatment options for SSc remain limited.4 Preliminary case-reports and series have suggested that rituximab, a chimeric monoclonal antibody targeting B cells, could improve skin and lung fibrosis in SSc.5–19 However, these studies were mostly limited by small samples sizes, lack of control arms, single centre designs, discrepancies in study designs and short durations of follow-up. In a previous European Scleroderma Trials and Research (EUSTAR) report on 63 patients with SSc, rituximab treatment was associated with improvement in skin fibrosis, particularly in the diffuse cutaneous form, together with a stabilisation of pulmonary functional testing.20 Though rituximab demonstrated a good safety profile, but this was limited by 6 months follow-up; and only nine of these patients had restrictive SSc-ILD, thus preventing any firm conclusions. The aim of our study was to investigate larger population with longer follow-up and including more patients with lung involvement to better assess the effect of rituximab on SSc and establish a side effect profile specific for SSc.
Methods
Data source
The ongoing EUSTAR is an international, multicentre, prospective registry managed by physicians (list of authors and online supplementary appendix I) and organised centrally by its committee.20
Supplemental material
For controls, we interrogated the EUSTAR database at the end of July 2017, providing information on 14 239 patients, from 142 participating centres, fulfilling the 2013 criteria for SSc21 (Strobe Checklist in online supplementary appendix II). Patients without follow-up (n=4664) and patients with previous autologous stem cell transplantation were excluded. The structure of the database, the minimum essential data set and the inclusion criteria have been described in detail previously.22
Design and analytic sample
From March to September 2017, we queried the database and sent a call for observations in the EUSTAR network regarding rituximab use. Out of 14 239 patients recorded in the database, 254 were recruited because of rituximab use (37 centres). We sent a questionnaire to each centre with at least one rituximab-treated patient. For each patient, we collected in addition to the database content, the main indication for initiating the treatment, previous treatments received and dosage. The following baseline and follow-up information were also queried: modified Rodnan skin score (mRSS), presence and extent of lung fibrosis on CT, FVC (% predicted), DLCO (% predicted), presence of digital ulcers, overlap disease (defined by co-occurrence of another autoimmune disease),23 number of tender and swollen joints (/28), DAS-28 ESR/CRP scores, joint contracture and tendon friction rubs, morning stiffness, visual analogic scale for articular pain, HAQ-DI score, presence of lower and upper gastrointestinal symptoms and CRP (mg/L). The number of infusions and dosage were recorded. Concomitant treatments and dosage were also collected.
Outcomes
The occurrence of any adverse event (including hypogammaglobulinemia,24 infection (and need for hospitalisation), scleroderma renal crisis [SRC]), serious adverse event and discontinuation because of an adverse event was collected. In case of death, we asked the relationship between the death and rituximab: (1) not related, (2) unlikely related, (3) possibly related, (4) probably related and (5) definitely related.
Outcomes were assessed at last observation under treatment (median follow-up [IQR]: 24.3 [13.3–41.4] months) responders for skin fibrosis were defined as patients with ≥5 points and 25% of improvement in mRSS.25 mRSS is frequently used as a primary outcome in clinical trials, therefore we assessed rituximab effect also in patients without a ‘skin indication’ and limited the analysis to patients with a mRSS ≥10 (n=131) consistently with distribution of skin involvement in Eustar.3 For lung fibrosis worsening, we used the following cut-offs: ≥10% decrease in FVC and ≥15% decrease in DLCO.26 Evolution of articular involvement was assessed: tender and swollen joints counts (/28), DAS-28 ESR/CRP scores, joint contracture, tendon friction rubs, duration of morning stiffness, articular pain, HAQ-DI score and CRP (mg/L). Concomitant steroid use and dosage were collected.
Covariates
Covariates used in the model to calculate propensity score were baseline characteristics: sex, age, cutaneous form, antinuclear antibodies (ANA), anticentromere antibodies (ACA), anti-Scl70 antibodies, RNA polymerases III (RNA pol III) antibodies, disease duration, region (Western and Eastern Europe, North and South America, Africa and Asia), time between two visits (time between the baseline and final visit under rituximab), previous and concomitant use of immunosuppressant (IS) or biologics, mRSS, DLCO, FVC and lung fibrosis. IS drugs included methotrexate, mycophenolate mofetil, azathioprine and cyclophosphamide, whereas biologics included TNF alpha inhibitors, tocilizumab and abatacept.
Statistical analysis
Categorical results are presented as counts and percentages. Non-normally distributed variables are presented as median with IQR and normally distributed variables as means±SD. Comparison of characteristics of treated and non-treated patients was performed by χ² test and Student’s t-test or the Mann–Whitney test, according to the distribution of the variable. Side effects during treatment with rituximab were summarised by the frequency and percentage. To evaluate efficacy of rituximab for skin fibrosis in SSc, a propensity score approach was used. This score was estimated using a logistic regression with adjustment on regions. The analysis of responders was based on propensity score matching with a ratio 1:4 and a calliper of 0.05 SD of the logit propensity score. To account for missing data, analyses were conducted using multiple imputations by chained equations with 50 imputations obtained after 10 iterations.27 The variables considered in the imputation models were all characteristics used in propensity score. For each complete imputed data set, propensity score was estimated and association between decrease in the mRSS and treatment was evaluated using conditional logistic regression. Results were aggregated by pooling estimates obtained on each imputed dataset according to Rubin’s rules.28 Balance in potentials confounders was assessed by standardised mean differences.29 Sensitivity analyses were performed using other alternative methods of propensity score analysis: ratio 1:1 within a calliper of 0.05 SD of the logit propensity score, stratification on the quintiles of the propensity score and inverse probability of treatment weighting. The analyses of decrease in the FVC of 10%, decrease in the DLCO of 15% and tapering or stopping steroids were performed according the same methodology and same covariates as decrease in mRSS. The variation of FVC as a continuous variable was analysed by a linear mixed-effects model. Exploratory analyses of skin fibrosis improvement and lung fibrosis worsening were focused on diffuse cutaneous form and early disease (<5 years of disease duration).
Factors associated with lung improvement in patients treated with rituximab were determined using univariate and multivariable logistic regression analyses with multiple imputations. Age, disease duration and DLCO were dichotomised according to their median or first quartile for FVC. All variables with p<0.1 in univariate were included in multivariate analysis with adjustment on regions. The lack of significant interaction between covariates was checked.
All tests were two-sided at a 0.05 significance level. Analyses were carried out using R statistical software V.3.3.2.
Results
Baseline cohort characteristics
From March to September 2017, out of 14 239 patients recorded in the database, 254 were recruited because of rituximab use (37 centres): 71% of female, median age: 51 years, 64% of diffuse cutaneous form and 71% displayed lung fibrosis. Median extent of lung fibrosis on CT was 20%.10–29 Anti-Scl70 and ACA antibodies were detected in 53% and 11% of the patients, respectively. An overlap syndrome was diagnosed in 26% of the cohort, consistently with previous reports in SSc.23 Previous treatments included DMARDs in 66/252 (32.5%), biologics in 24/252 (9.5%), cyclophosphamide in 23/252 (9.1%). Further details are provided in table 1 and online supplementary table I and II.
Baseline characteristics of patients with SSc treated with rituximab and untreated SSc-controls from EUSTAR database
The leading indication for rituximab was lung involvement in 146/254 (58%) cases, skin in 81/254 (32%) cases and in 108/254 (42%) musculoskeletal involvement (flowchart in online supplementary figure 1). Concomitantly to rituximab, patients received steroids for 67.3% (median dose: 10 mg/day [IQR: 5–10]). Total 136 (53.7%) were treated in parallel with DMARDs (methotrexate for 75, mycophenolate mofetil for 45, azathioprine for 14 and cyclophosphamide for 6).
Supplemental material
Safety analysis
After a median follow-up of 2 years, nearly 70% of patients (175/254) had no reported side effect, 43 (17%) had minor side effects and 36 (14%) were considered as severe by investigating centre. This led to discontinuation of the treatment in 24 patients (9%). During follow-up, six deaths were recorded: four unrelated to the treatment (two sudden deaths, one sepsis attributed to decubitus ulcers, one heart failure) and two possibly related (two respiratory insufficiencies in the context of lung carcinoma). In all, five cancers were reported during the follow-up. There was no association between occurrence of infections and previous or concomitant treatment with IS or hypogammaglobulinemia. Further details are provided in online supplementary table III.
Efficacy
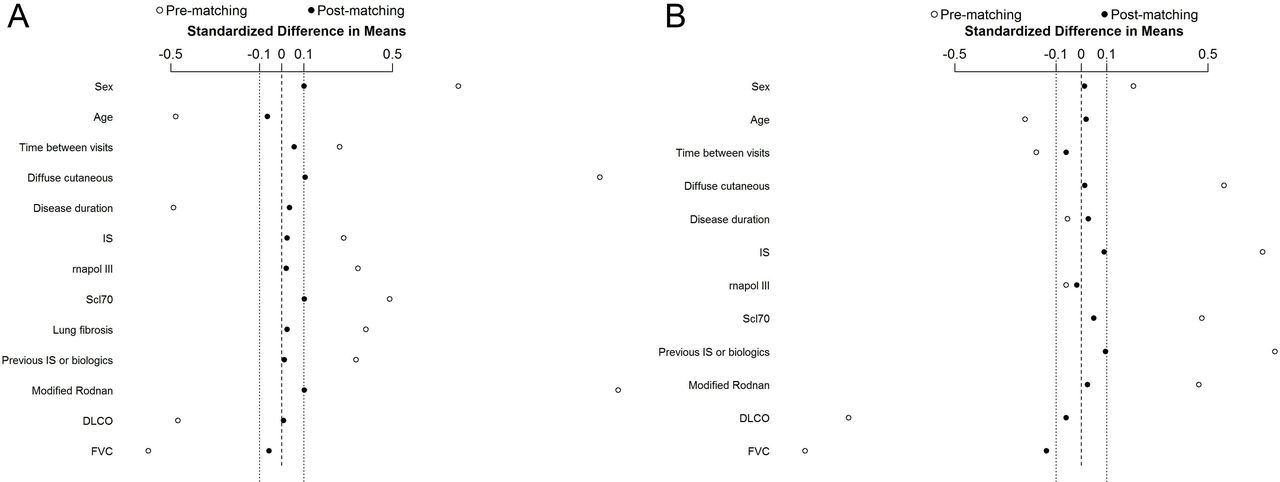
Among the 14 239 patients who underwent ≥1 visit, 9575 had ≥1 follow-up (table 1). Comparison of characteristics between patients with and without follow-up showed minor differences (online supplementary table IV). Matching for skin and lung allowed comparability of cases and controls (figure 1).

Quality of the matching: Matching 1:4 for skin (A) and for lung involvement (B). Matching allows comparability of cases and controls with less than 10% of difference between all variables studied. Data, presented as mean±SEM, are from the first imputed and matched (ratio 1:4) dataset. DLCO, diffusing capacity of lung for carbon monoxide; FVC, forced vital capacity.
Skin fibrosis
The mRSS of patients treated for skin fibrosis decreased from mean±SD 22.1 (±9.3) to 14.1 (±8.4) in treated patients (n=74) vs 21.1 (±10.5) to 16.2 (±10.3) (p<0.0001) in untreated patients matched according to propensity score (n=281) (figure 2A). In patients with a mRSS ≥10 (n=131), the mRSS decreased from 21.2 (±8.8) to 13.4 (±7.9) vs 20.4 (±8.2) to 16.0 (±8.2) in controls (p<0.0001) (figure 2B).

Evolution of skin and lung fibrosis among propensity score-matched patients treated and untreated with rituximab. (A,B) evolution of modified Rodnan skin score between baseline and last visit (under treatment) in patients and propensity score-matched patients from EUSTAR: (A): in patients with skin indication for the treatment; (B) in patients with modified Rodnan skin score at baseline ≥10; (C) evolution of forced vital capacity between baseline and last visit (under treatment) in patients with a lung indication for the treatment and propensity score-matched patients from EUSTAR; (D) evolution of DLCO between baseline and last visit (under treatment) in patients with a lung indication for the treatment and propensity score-matched patients from EUSTAR. Data, presented as mean±SEM, are from the first imputed and matched (ratio 1:4) dataset. DLCO, diffusing capacity of lung for carbon monoxide; EUSTAR, European Scleroderma Trials and Research; FVC, forced vital capacity.
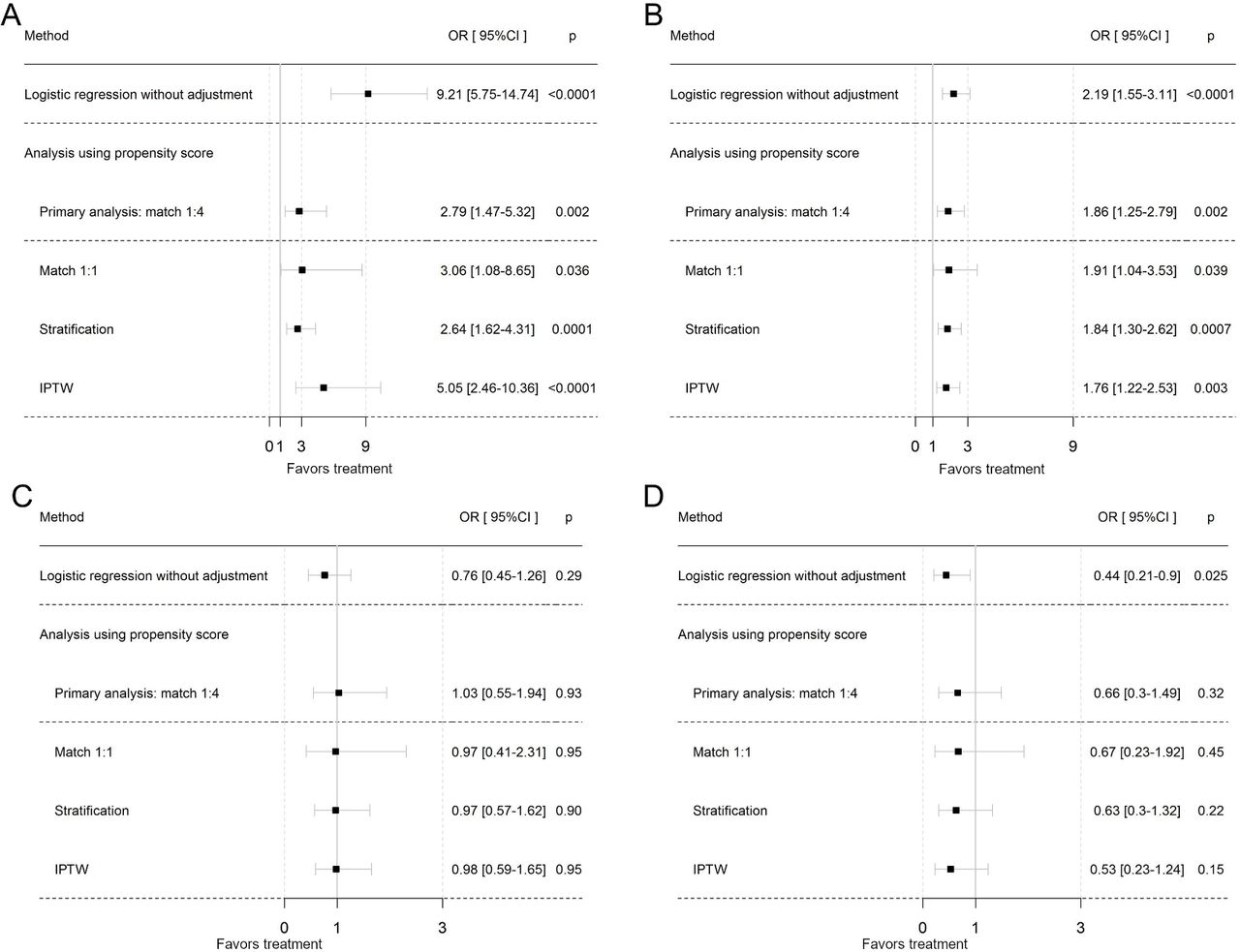
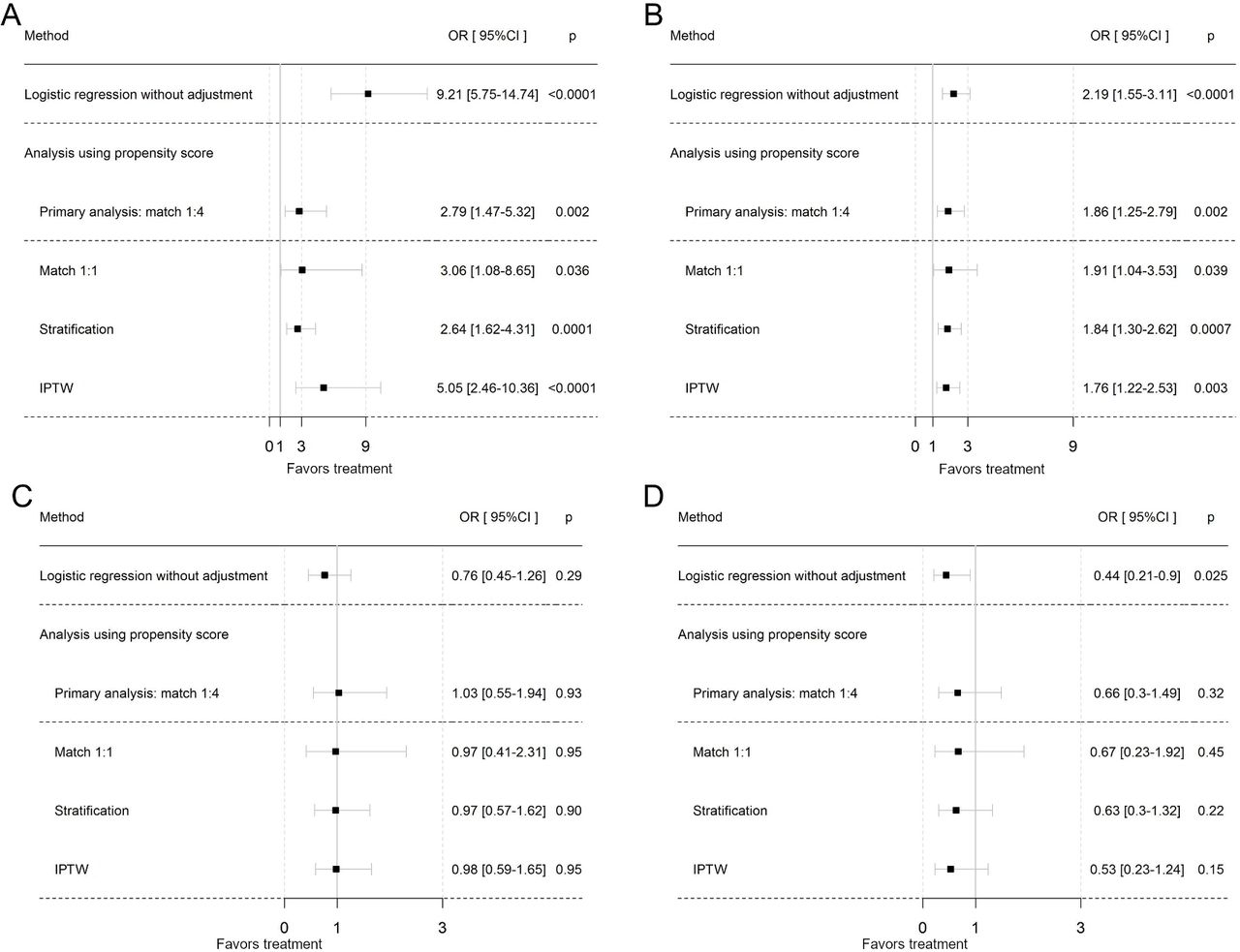
Rituximab-treated patients had a higher probability of improvement in dermal fibrosis as compared with propensity score matched-controls (22.7 vs 14.03 events per 100 person-years; OR: 2.79 [1.47–5.32]; p=0.002). This was confirmed in sensitivity analyses (figure 3A).
![[annrheumdis-2018-214816supp002.jpg]](https://ard.bmj.com/content/annrheumdis/78/7/979/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
{kind=link}
{kind=link}
{kind=link}
Adjusted OR for skin fibrosis improvement and lung fibrosis worsening among propensity score-matched patients treated or untreated with rituximab. The analyses of decrease in the modified Rodnan score of 5 points and 25% and decrease in the FVC of 10% and decrease in the DLCO of 15% were based on propensity score matching with a ratio 1:4. For each complete imputed data set, propensity score was estimated and association between decrease in the modified Rodnan score/ in FVC and in DLCO, respectively, and treatment was evaluated using conditional logistic regression. We used other matching method with ratio 1:1 within a calliper of 0.05 SD of the logistic propensity score, stratification on the quintiles of the propensity score and IPTW. Decrease in the modified Rodnan score of 5 points and 25% in patients with (A) skin indication; (B) modified Rodnan skin score >10 at baseline; (C) decrease in the FVC of 10% in patients with lung indication for the treatment; (D) decrease in the DLCO of 15% in patients with lung indication for the treatment. DLCO, diffusing capacity of lung for carbon monoxide; FVC, forced vital capacity; IPTW, inverse probability of treatment weighting.
Same results were observed for patients with a mRSS ≥10 (OR: 1.86 [1.25–2.79]; p=0.002) (figure 3B) as well as in subgroup analyses (diffuse and early forms; online supplementary figure 2A,B).
Supplemental material
![[annrheumdis-2018-214816supp003.JPG]](https://ard.bmj.com/content/annrheumdis/78/7/979/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
Lung fibrosis
In lung treated patients (n=146), FVC remained stable during the follow-up (76.3 (±19.3) to 77.7 (±20.2)), similarly to controls (79.1 (±20.6) to 80.7 (±21.1)) (n=497) (figure 2C). DLCO also remained stable both in treated patients (54.4 [±18.8] to 55.5 [±19.5]) and in controls (55.6 [±18.7] to 54.7 [±20.2]) (figure 2D). Extent of fibrosis remained stable (20.0 [±2.1] to 20.0 [±2.5]) (n available=60). Treated patients did not have significantly different rates of decrease in FVC >10% (6.5 vs 6.6 events per 100 person-years; OR: 1.03 [0.55–1.94]; p=0.93) nor in DLCO decrease (figure 3C,D), which was confirmed in all secondary analyses (online supplementary figure 2 C, D and 3). In univariate cox models, lung function had a trend to improve in early disease and in patients with FVC <80%, which was not confirmed in multivariate analysis (table 2).
Factors associated with lung improvement in patients treated with rituximab
In secondary analyses, the concomitant use of mycophenolate to rituximab (n=37 with lung indication) showed a trend for better outcomes (delta FVC with controls: 5.22 [0.83–9.62]; p=0.019 vs delta FVC: 3 [0.66–5.35]; p=0.012 in patients receiving rituximab alone). Furthermore, 9/31 (29%) had an increase >10% in FVC. The difference with patients treated by rituximab alone was not statistically significant (delta: 2.98 [–2.12 to 8.09]; p=0.25). No adjusted analysis could be performed due to the small sample size. DLCO did not change significantly in this subgroup.
There was no difference for skin and lung outcomes according to rheumatoid factor, anti-CCP antibodies or smoking status (online supplementary table V).
Musculoskeletal involvement
All articular parameters, but two (joint contractures and HAQ-DI) significantly decreased with rituximab (table 3). No controlled analysis could be performed because of a high proportion of missing data (eg, 81% for tender and swollen joint counts in control group).
Evolution of musculoskeletal involvement during treatment with rituximab
Inflammation and cotreatments
CRP levels decreased during the treatment from 11.5 (±1.0) to 6.7 (±0.7) mg/L (p<0.0001). About one quarter of the patients treated with steroids at baseline could stop steroids and steroids dosage decreased from 9.5 (±0.5) mg/day to 7.0 (±0.3) mg/day (p<0.0001) in the 130 remaining patients. Patients treated with rituximab were more likely to decrease or stop steroids in controlled analyses (25.3 vs 18.0 events per 100 person-years; OR: 2.34 [1.56–3.53], p<0.0001) (online supplementary figure 3B).
Supplemental material
![[annrheumdis-2018-214816supp004.JPG]](https://ard.bmj.com/content/annrheumdis/78/7/979/DC4/embed/inline-supplementary-material-4.jpg?download=true){kind=link}
Dose-effect
Rituximab regimens were variable according to centres: for each infusion: dose of 1000 mg for 203 patients, 500 mg for 27 375 mg/m2 for four patients. We observed a dose-effect with a better effect on skin involvement for a total dosage higher than 4000 mg (online supplementary table VI).
Discussion
In a large cohort of carefully matched patients treated with rituximab for skin, or lung involvement, rituximab was associated with a good safety profile. The outcomes showed a high efficacy on skin fibrosis, but not on lung. Patients treated with rituximab were 2-fold more likely to stop or decrease steroids.
Following previous promising studies suggesting an amelioration of lung involvement, the raw analyses after propensity score matching clearly show no difference between treated and not treated patients and overall a large proportion of non-progressive patients.7 10 12 14–16 19 Therefore, the results should be interpreted as the lack of effects of rituximab in this sample of patients with SSc. Nevertheless, one may advocate that the lung trajectory of rituximab-treated patients may differ from the one of untreated patients. Indeed, if the treating physician decided to offer rituximab therapy, then it is most of the time because of lung activity and severity, which are identified are poor predictive factors. These biases (selection biases, persistence of confounders despite the matching) are limitations to our study inherent to its observational design.30 Therefore, the potential stabilisation of ILD following rituximab therapy has to be addressed in the future but only a randomised trial will provide robust answer.
Some previous small uncontrolled or unadjusted series have suggested some efficacy of rituximab on cutaneous involvement in SSc.5–13 19 29 However, evaluation of drug efficacy in SSc might be difficult because of spontaneous improvement in skin fibrosis during the first years, highlighting the need of control group. In our study, patients treated with rituximab were twofold more likely to improve skin fibrosis in all matched analyses, sensitivity analyses and subgroup approaches. The mRSS is a validated surrogate marker31–34 frequently used as an outcome measure in clinical trials.36 Indeed, worsening in mRSS is associated with higher mortality, and worsening of internal organ involvement.32 37 38 Conversely, improvement of the skin score is predictive of favourable outcomes, including better survival.38 Therefore, improvement in mRSS observed in rituximab-treated patients might indicate a better prognosis for these patients. Consistently, CRP levels, a marker of disease activity and severity,39 decreased following rituximab treatment.
One may also highlight the different trajectory between skin and lung outcomes in our sample. It must be pointed out that this has already been observed and by example the recent tocilizumab trial showed some benefit on lung whereas skin was less influenced.40 This highlights the difficulties to design clinical trials in SSc regarding both the choice of the primary outcome measure and also the patients selection criteria.41 A clue for the future to get a better impact on SSc outcomes might be combination therapy which seems to be more effective on lung involvement in our study and has shown clear benefit for treatment with rituximab in other diseases.42
Surprisingly, few patients have been previously treated with cyclophosphamide.43 This choice of using first rituximab might be driven by the need of concomitant treatment for musculoskeletal involvement in almost half of the cohort (online supplementary figure 1). Furthermore, common use of rituximab in other diseases like RA but also connective tissue diseases and vasculitis has given rheumatologists confidence in the management and in the safety of rituximab. Finally, the use of cyclophosphamide and mycophenolate mofetil could be limited by safety data.44
Interestingly, rituximab use doubled the probability of discontinuing or decreasing steroids. This is of major importance, since steroids cumulative dose increases the risk of subclinical/clinical atherosclerosis45 and SRC46 in SSc.
In our study, safety profile of rituximab was acceptable with in particular no progressive multifocal leukoencephalopathy or related-death. Furthermore, despite the use of intravenous steroids, only two SRCs were reported.
The main strengths of our study are (1) large sample size, (2) availability of well-matched controls, (3) standardised collection of data according to a questionnaire and (4) broad spectrum of patients included corresponding to ‘real-life’ patients and allowing subgroup analyses (diffuse forms, early SSc). Using extensive matching methods, we accounted for many potential cofounders of the associations between rituximab use and outcomes. We also performed several sensitivity and subgroups analyses, which were highly consistent.
Our study has limitations: first, rituximab regimens were variable according to centres. We analysed effect of the dose received and observed a dose-effect for a dosage higher than 4000 mg for skin involvement, suggesting that a dosage of 1000 mg should be used for the first infusions. This is an open label study, which can bias study results towards beneficial effect for the test medication (if the examiner anticipates beneficial effect of the treatment) in an outcome measure that is less objective (ie, mRSS) than FVC, which is more objective and less dependent on the examiner’s bias. There are also limitations inherent to the observational design of this study. However, the importance of disease registries, like EUSTAR, in rare diseases was recently highlighted, as they allowed collecting detailed case studies with standardised information and improving understanding of SSc and its treatment.47 Furthermore, the study reflects clinical practice in this orphaned heterogeneous disease. The duration of exposure to rituximab was relatively short (2 years), which limited precision for safety analyses. We could also not assess safety in control group (no data available) or outcomes that occurred after withdrawal of rituximab. Finally, despite highly matched cohorts across a wide range of characteristics, we cannot rule out residual confounders.
References
Footnotes
Handling editor Josef S Smolen
Correction notice This article has been corrected since it published Online First. Affiliation number 11 has been amended.
Collaborators EUSTAR coworkers, Serena Guiducci; Ulrich A. Walker; Diego Kyburz; Giovanni Lapadula; Britta Maurer; Suzana Jordan; Rucsandra Dobrota; Radim Becvar; Stanislaw Sierakowsky; Otylia Kowal Bielecka; Alberto Sulli; Maurizio Cutolo; Giovanna Cuomo; Ileana Nicoara; André Kahan; Panayiotis G. Vlachoyiannopoulos; Carlo Maurizio Montecucco; Roberto Caporali; Jiri Stork; Murat Inanc; Patricia E. Carreira; Srdan Novak; László Czirják; Cecilia Varju; Eugene J. Kucharz; Anna Kotulska; Magdalena Kopec-Medrek; Malgorzata Widuchowska; Franco Cozzi; Blaz Rozman; Carmel Mallia; Bernard Coleiro; Armando Gabrielli; Dominique Farge; Chen Wu; Zora Marjanovic; Helene Faivre: Darin Hij; Roza Dhamadi; Frank Wollheim; Agneta Scheja; Dirk M Wuttge; Kristofer Andréasson; Duska Martinovic; Alexandra Balbir-Gurman; F. Trotta; Andrea Lo Monaco; Raffaele Pellerito; Ospedale Mauriziano; Paola Caramaschi; Jadranka Morovic-Vergles; Carol Black; Christopher Denton; Nemanja Damjanov; Jörg Henes; Vera Ortiz Santamaria; Stefan Heitmann; Dorota Krasowska; Matthias; Paul Hasler; Harald Burkhardt; Andrea Himsel; Gianluigi Bajocchi; José Antonio Pereira Da Silva; Maria João Salvador; Bojana Stamenkovic; Aleksandra Stankovic; Carlo Francesco Selmi; Maria De Santis; Mohammed Tikly; Lev N. Denisov; Ariane Herrick,Ulf Müller-Ladner; Marc Frerix; Ingo Tarner; Raffaella Scorza; Francesco Puppo; Merete Engelhart; Gitte Strauss; Henrik Nielsen; Kirsten Damgaard; Gabriela Szücs; Antonio Zea Mendoza; Carlos de la Puente; Sifuentes Giraldo WA; Øyvind Midtvedt; Silje Reiseter; Torhild Garen; David Launay; Guido Valesini; Ruxandra Maria Ionescu; Laura Groseanu; Daniela Opris; Roxana Sfrent Cornateanu; Razvan Ionitescu; Ana Maria Gherghe; Alina Soare; Marilena Gorga; Mihai Bojinca; Mihaela Milicescu; Cord Sunderkötter; Annegret Kuhn; Nora Sandorfi; Georg Schett; Christian Beyer; Pierluigi Meroni; Francesca Ingegnoli; Luc Mouthon; Filip De Keyser; Karin Melsens; Francesco P. Cantatore; Ada Corrado; Line Iversen; Carlos Alberto von Mühlen; Jussara Marilu Bohn; Lilian Scussel Lonzetti; Kilian Eyerich; Rüdiger Hein; Elisabeth Knott; Piotr Wiland; Magdalena Szmyrka-Kaczmarek; Renata Sokolik; Ewa Morgiel; Marta Madej; Frédéric A. Houssiau; Brigitte Krummel-Lorenz; Petra Saar; Martin Aringer; Claudia Günther; Rene Westhovens; Jan Lenaerts; Branimir Anic; Marko Baresic; Miroslav Mayer; Maria Üprus; Kati Otsa; Brigitte Granel; Carolina de Souza Müller; Sebastião C. Radominski; Valderílio F. Azevedo; Sergio Jimenez; Joanna Busquets; Svetlana Agachi; Liliana Groppa; Lealea Chiaburu; Eugen Russu; Sergei Popa; Thierry Zenone; Margarita Pileckyte; Alessandro Mathieu; Alessandra Vacca; Percival D. Sampaio-Barros; Natalino H. Yoshinari; Roberta G. Marangoni; Patrícia Martin; Luiza Fuocco; Simon Stebbings; John Highton; Peter Chapman; John O’Donnell; Lisa Stamp; Alan Doube; Kamal Solanki; Douglas Veale; Marie O’Rourke; Esthela Loyo; Mengtao Li; Walid Ahmed Abdel Atty Mohamed; Antonio Amoroso; Antonietta Gigante; Fahrettin Oksel; Figen Yargucu; Cristina-Mihaela Tanaseanu; Monica Popescu; Alina Dumitrascu; Isabela Tiglea; Rosario Foti; Rodica Chirieac; Daniel Furst; Peter Villiger; Sabine Adler; Jacob van Laar; Cristiane Kayser; Nihal Fathi; Manal Hassanien; Paloma García de la Peña Lefebvre; Silvia Rodriguez Rubio; Marta Valero Exposito; Emmanuel Chatelus; Jean Sibilia; Jacques Eric Gottenberg; Hélène Chifflot; Ira Litinsky; Paul Emery; Maya Buch; Francesco Del Galdo; Algirdas Venalis; Irena Butrimiene; Paulius Venalis; Rita Rugiene; Diana Karpec; Joseph A. Lasky; Vanesa Cosentino; Eduardo Kerzberg; Fabiana Montoya; Washington Bianchi; Sueli Carneiro; Giselle Baptista Maretti; Dante Valdetaro Bianchi; Massimiliano Limonta; Antonio Luca Brucato; Elide Lupi; Itzhak Rosner; Michael Rozenbaum; Gleb Slobodin; Nina Boulman; Doron Rimar; Maura Couto; Sarah Kahl; Fei Chen; Deborah McCloskey; Halina Malveaux; François Spertini; Camillo Ribi; Guillaume Buss; Thierry Martin; Aurélien Guffroy; Vincent Poindron; Fatima Chotchaeva; Nikolay A. Mukhin; Sergey Moiseev.
Contributors ME, MB and YA formulated the study hypotheses and contributed to its design, literature search, composition of the tables and figures and redaction of the first draft and subsequent iterations of the manuscript. ME, MB, CB-Q and YA: analysis and interpretation of data. ME and MB performed the statistical analyses. OD, VS, MM-C, JJAS, M-ET, YB-M, FI, PIN, AL, ES, IC, PA, SV, EDL, EH, AE, LA, MK, FJL-L, JHWD, NH, A-MH-V, VR, VMH, MRP, CA, ER, CM, MK, LAS, CC, RH, SU, SY, SR, CC and YA conceived and launched the EUSTAR database, collected data in their respective countries and offered critical comments regarding the manuscript. All authors have finally approved the submitted version to be published.
Funding EUSTAR database is supported by the World Scleroderma Foundation.
Competing interests OD has consultancy relationship with Actelion, Bayer, BiogenIdec, Boehringer Ingelheim, ChemomAb, espeRare foundation, Genentech/Roche, GSK, Inventiva, Italfarmaco, Lilly, medac, MedImmune, Mitsubishi Tanabe Pharma, Pharmacyclics, Novartis, Pfizer, Sanofi, Sinoxa and UCB in the area of potential treatments of scleroderma and its complications. OD has received research funding from Actelion, Bayer, Boehringer Ingelheim, Mitsubishi Tanabe Pharma and Roche in the area of potential treatments of scleroderma and its complications. In addition, OD has a patent mir-29 for the treatment of systemic sclerosis licensed. M-ET has received consulting fees, speaking fees or honoraria from Abbvie, BMS, Lilly, Medac, MSD, Pfizer, Roche and UCB. PA has received travel expenses from Roche (<2500€). SV received speaking fees by Pfizer, Abbvie, Bristol-Myers Squibb, consultant fee from Thermofischer and Boehringer-Ingelheim Italia and Educational support from Pfizer, Roche, BMS. EH has received speaker fees and/or honoraria for consultations from Roche, less than 10 000€. NH received lecture fees from Actelion Pharmaceuticals, Pfizer, Roche and grant support from Actelion and Bayer Pharmaceuticals. CM has/had consultancy relationship and/or has received honoraria from Actelion, Abbvie, Roche and Geneva Romfarm in the area of systemic sclerosis and its complications. CC has received travel grants from Roche. YA has/had consultancy relationship and/or has received grants from Actelion, Bayer, BMS, Boehringer-Ingelheim, Inventiva, Roche, Sanofi-Aventis in the area of systemic sclerosis.
Patient consent for publication Obtained.
Ethics approval Each participating centre obtained approval of the local ethics committee and all registered patients granted their informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional unpublished data from the study are available.