Article Text

Abstract
Background Survival in systemic lupus erythematosus (SLE) has improved substantially in the last 50 years. The aim of the present study was to assess the evolution of the all-cause, cause-specific and age-specific standardised mortality ratios (SMRs) of patients with lupus in Ontario, Canada.
Patients and methods Between 1971 and 2013, 1732 patients were followed in the Toronto Lupus Clinic. Causes of death were retrieved from death certificates, autopsy reports, hospital records or the records of the family physicians. They were categorised as atherosclerotic, infectious, malignancy, active lupus and others. For the calculation of the SMR (indirect standardisation method), data from the general population of Ontario, Canada were used (Statistics Canada).
Results Two hundred and forty-nine patients (205 women) died (infections 24.5%, atherosclerosis 15.7%, active lupus 13.3%, malignancy 9.6%); mean age was 53.2±16.6 years and mean disease duration 15.2±11.7 years. The all-cause SMR was substantially decreased from the 1970s (13.5, 95% CI 8.6 to 18.5) to recent years (2.2, 95% CI 1.4 to 3.1). Similar trends were observed for atherosclerosis, infections and malignancies over time. The all-cause age-specific SMR was particularly high in younger (19–39 years old) patients (SMR=12.4, 95% CI 9.7 to 15.1) as compared with individuals older than 40 years (SMR=3.1, 95% CI 2.6 to 3.6). The cause-specific SMR was also higher in younger patients, particularly for infections and malignancies.
Conclusions The all-cause and cause-specific SMR significantly decreased over time, likely reflecting the advances in the management of SLE and certain comorbidities. The all-cause and cause-specific SMR was particularly high for younger patients (<40 years old).
- systemic lupus erythematosus
- standardized mortality ratio
- causes of death
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Mortality has improved in systemic lupus erythematosus (SLE) over the last 50 years. However, the standardised mortality ratio (SMR) is still approximately 3, indicating that patients with SLE are three times more likely to die from any cause as compared with patients without lupus.
What does this study add?
In this study, we showed that the all-cause and cause-specific (atherosclerosis, infections, malignancies) SMR of patients with SLE have been significantly decreased from 1971 to 2013.
How might this impact on clinical practice or future developments?
SMR (all-cause and cause-specific) was particularly higher in patients younger than 40 years old. These findings underline the need to optimise the management of the disease and its major comorbidities, particularly in the younger age groups.
Introduction
Survival in systemic lupus erythematosus (SLE) has improved considerably in the last 60 years. The 5-year survival rate was estimated at 50% in 1955,1 while it reached 64%–87% in the 1980s and >95% in the early 2000s.2–5 Accordingly, the 10-year survival rate was reported at 87%–93% in the 1990s6 7 and 96.3% in the contemporary years.8 A recent systematic review and meta-analysis of 125 studies in adult patients with lupus corroborated these findings with a pooled 5-year survival of 95% for the developed countries from 2008 to 2016.9 However, their calculations were more modest for the 10-year survival, which reached 89% for the same period; the authors also reported that the 15-year survival was 82%.9
Given that life expectancy has also greatly improved in the general population for the same period,10 standardised indices that are age-adjusted would better describe the real trends in SLE mortality. The standardised mortality ratio (SMR) represents the ratio of the number of deaths observed in a given cohort divided by the deaths reported in the general population for the same time period. The first population-based study of SMR in SLE was conducted in Sweden and reported that the all-cause SMR was 3.63 (95% CI 3.49 to 3.78) from 1964 to 1995.11 Several studies were published after that and were recently reviewed by two independent groups.12 13 In these meta-analyses, Yurkovich et al 12 and Lee et al 13 reported an all-cause SMR of 2.98 (95% CI 2.32 to 3.83) and 2.66 (95% CI 2.09 to 3.39), respectively.
However, both studies provided an overall estimate of the SMR throughout the observation period without analysing the trend of SMR over time. The aim of the present study was to assess the evolution of the all-cause and cause-specific SMRs of patients with lupus from 1971 to 2013 in Ontario, Canada.
Patients and methods
For the purposes of the present study, the long-term longitudinal cohort of the University of Toronto Lupus Clinic (UTLC) was investigated from 1971 to 2013. During that period, 1732 patients with SLE were followed regularly in the clinic. Data beyond 2013 were not used since, up to the time of writing, the cause-specific death counts by age/gender in Ontario, Canada were not available.
All patients fulfilled the revised American College of Rheumatology criteria for the classification of SLE14 or had three criteria and a supportive biopsy (kidney). Patients are followed regularly at intervals of 2–6 months according to a standardised research protocol, which is regularly updated.15 This protocol captures demographic, clinical, immunological and therapeutic variables as well as most comorbidities. Regarding mortality, the protocol captures the cause (primary and secondary), location and date of death. For the present study, only the primary causes of death were considered. Causes of death are recorded in the database based on autopsy reports, death certificates, hospital discharge summaries or the records of the family physicians for each patient.
In the context of this study, causes of death were categorised as atherosclerotic, infection, malignancy, active lupus and others. Patients were also categorised according to the age at death in 10-year intervals (15–24, 25–34 etc up to 85–94) and in a dichotomous manner (younger or older than 40 years).
For the calculation of the SMR, mortality data from the general population of Ontario, Canada retrieved from Statistics Canada for the same time period were used to derive the expected number of events in our study population. The ratio of observed to expected events provided the SMR. Primary causes of death are available in Ontario since 1980. As such, cause-specific SMRs could be calculated after that time. From 1971 to 1979, only the all-cause SMR was calculated. Causes of death were defined according to the 10th revision of the International Classification of Diseases (ICD-10) and grouped into infections, malignancies, atherosclerotic and others. Corresponding ICD-10 code categories for infections included A00–B99, J09–J18 (respiratory infections), N30 (urinary tract infections) and R65.2 (sepsis due to unidentified micro-organism). Corresponding codes for malignancies included C00–D49 whereas the respective codes for atherosclerosis included I20–25 (ischaemic coronary heart disease), I60–68 (cerebrovascular diseases), I70–75 (peripheral vascular disease) and I96 (gangrene). The same ICD-10 codes were applied to the UTLC cohort as well. The code M32 (SLE) was only applied to the UTLC cohort and not the general population.
Patient and public involvement
Included patients are/were participating in the studies of the University of Toronto Lupus Clinic after signed informed consent. Relevant data for the general population of Ontario, Canada were retrieved from Statistics Canada (as described above).
Statistical analysis
Descriptive statistics were represented by mean±SD for continuous variables and counts (per cent) for count variables. The indirect standardisation method was used for the calculation of SMR. Ninety-five per cent CIs are reported for SMR where relevant. The procedure STDRATE in SAS V.9.4 was used to calculate all-cause and cause-specific SMR.
Results
Two hundred and forty-nine patients (205 women) who had been enrolled in the UTLC cohort died between 1971 and 2013. The most common causes of death were infections (n=61, 24.5%), atherosclerosis (n=39, 15.7%), active lupus (n=33, 13.3%) and malignancy (n=24, 9.6%). Concerning active lupus, the precise causes of death were multiple organ failure syndrome (in the absence of sepsis, n=8), active lupus nephritis with rapidly progressive glomerulonephritis (n=7), central nervous system vasculitis or cerebritis (n=6), lupus myocarditis (n=4), mesenteric vasculitis (n=3), diffuse alveolar haemorrhage/lupus pneumonitis (n=3), thrombotic thrombocytopenic purpura (n=1) and pericarditis/cardiac tamponade (n=1), all in the context of active disease. Sixty-seven patients died from other causes (mainly renal failure, chronic obstructive pulmonary disease, gastrointestinal bleeding, pulmonary embolism etc) whereas the cause was unknown in 25 (10%). The mean age at death was 53.2±16.6 years and mean disease duration 15.2±11.7 years. The mean age at death was significantly increased from 42.2±12.9 years in the 1970s to 58.8±14.6 years during the recent years 2010–2013 (details in figure 1). For the same time span, the potential years of life lost were decreased from 33.5 in the 1970s to 23.6 between 2010 and 2013 (figure 1).

Mean age at death of the UTLC patients through the decades (solid line). The life expectancy of the general Canadian population at the same time points is also depicted (dashed line) along with the potential years of life lost (lower dashed line).
All-cause and cause-specific SMRsstandardized mortality ratios over time
The all-cause SMR over the entire period 1971–2013 was 4.1 (95% CI 3.6 to 4.6). Regarding its evolution over time, there was a significant decrease from 13.5 (95% CI 8.6 to 18.5) in the 1970s to 2.2 (95% CI 1.4 to 3.1) during 2010–2013. Likewise, the overall 1980–2013 cause-specific SMR was 4.7 (95% CI 3.4 to 6.0) for atherosclerosis, 4.4 (95% CI 3.3 to 5.5) for infections and 3.4 (95% CI 2.2 to 4.6) for malignancies. However, these cause-specific SMRs were considerably decreased from the 1980s to 2010–2013. The evolution of all-cause and cause-specific SMRs over the decades is shown in table 1.
All-cause and cause-specific standardised mortality ratios* for SLE from 1971 to 2013
Age-specific SMR
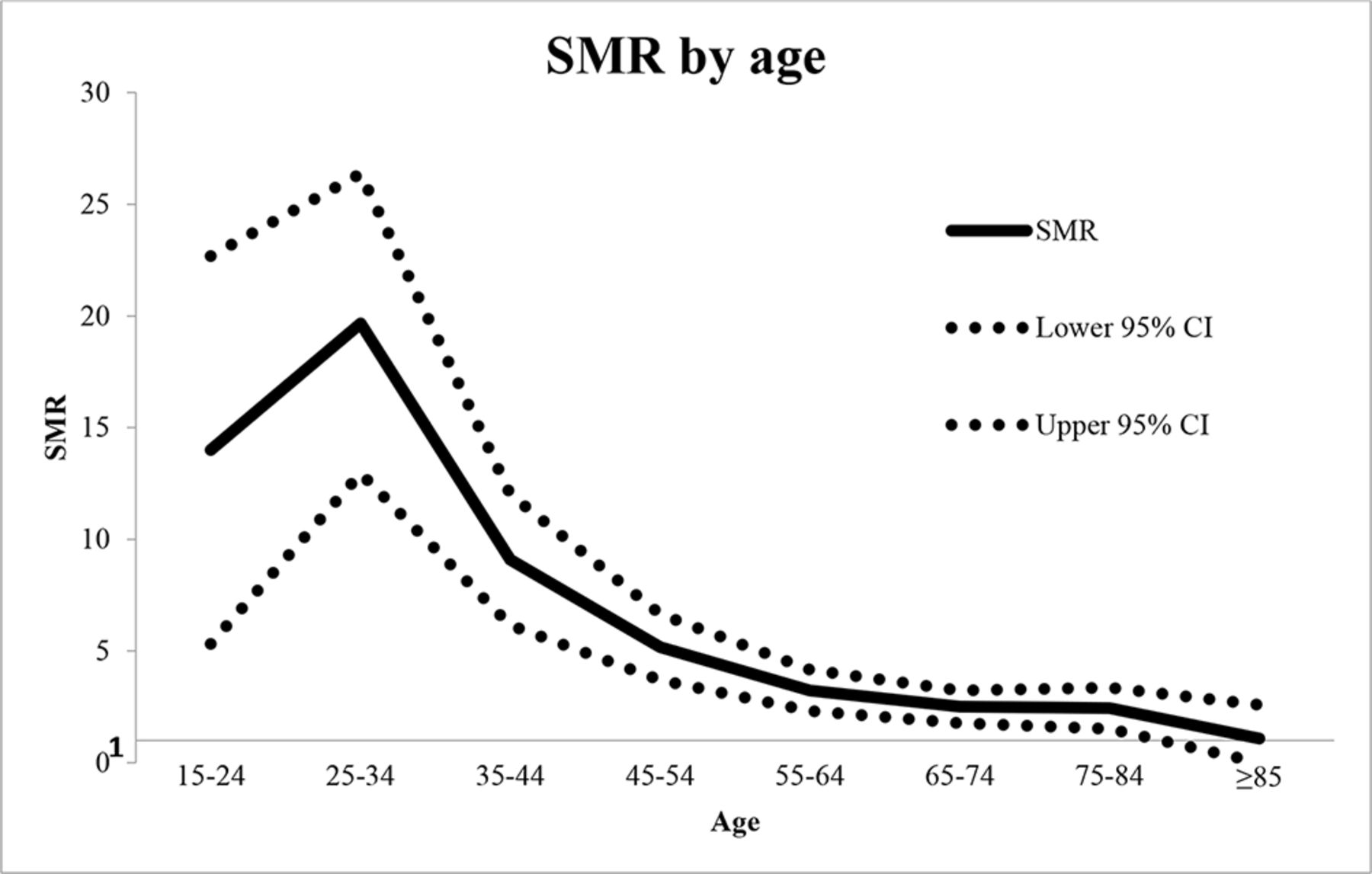
The all-cause SMR by decades of age was the highest in the age group 25–34 (19.7, 95% CI 13 to 26.4) and was gradually decreased in older age groups. Details are given in table 2 and figure 2. The age-specific SMR was particularly high in younger (19–39 years old) patients (all-cause SMR=12.4, 95% CI 9.7 to 15.1) as compared with the patients who were older than 40 years (all-cause SMR=3.1, 95% CI 2.6 to 3.6). Likewise, cause-specific SMRs were significantly higher in this age group (19–39 years) as compared with patients who were ≥40 years old (table 3).
Age-specific SMR (all-cause) for UTLC patients in Ontario, Canada 1971–2013
All-cause and cause-specific standardised mortality ratios* (SMRs) for patients 19–39 years old and ≥40 years 1980–2013

{kind=link}
{kind=link}
Age-specific standardised mortality ratio (SMR) for all causes according to the age at death divided in decades. The SMR was particularly high in young ages (19–44 years) while it remained significantly higher than one even for patients who died between 75 and 84 years of age. For patients older than 85 years, the mortality rate was not different than that of the general population of Ontario, Canada.
Discussion
In the present study, we showed that all-cause and cause-specific SMRs (for infections, atherosclerosis and malignancies) were progressively substantially decreased in Ontario, Canada from 1971 to 2013. In addition, all-cause and cause-specific SMRs were considerably higher for patients 19–39 years old as compared with patients 40 years of age and older. With regards to age, the mortality rate was always higher than that of the general population in all age groups except for the patients who were older than 85 years at the time of death.
The significant decrease of the all-cause SMR over time was first reported by Bjornadal et al in Sweden (from 1964 to 199511) and then by Bernatsky et al in a multiethnic cohort (from 1970 to 2000).16 For the latter study, data were collected from 23 centres and 9547 patients (1255 deaths); the all-cause SMR was 2.4 (95% CI 2.3 to 2.5) from 1970 to 2001 with a substantial decrease from the 1970s to the 1990s.16 Furthermore, Yurkovich et al reported a meta-SMR of 2.98 (95% CI 2.3 to 3.8) based on a meta-analysis of 12 studies (27 123 patients, 4993 deaths from 1950 to 2008),12 whereas that was 2.66 (95% CI 2.09 to 3.39) in a more recent meta-analysis (15 studies, 26 101 patients, 4640 deaths).13 Our study yielded a significantly higher all-cause SMR (4.1, 95% CI 3.6 to 4.6, from 1971 to 2013), although that was comparable after 2000 (3.2, 95% CI 2.4 to 4). Concerning the study of Bernatsky et al, the difference could be attributed to the population diversity, with centres from Sweden, Iceland and Scotland displaying an all-cause SMR less than 2 even from the 1990s.16 On the contrary, Canadian centres had an all-cause SMR greater than 3. With regards to the meta-analyses, the range of the all-cause SMR was rather wide (from 0.95 to 7.23), while a significant proportion of the patients were duplicated in the included studies.12
The noticeable improvement of the mortality rate in SLE reflects the better identification of the patients, possibly related to the introduction of the 1982 American College of Rheumatology criteria for the classification of SLE,17 as well as the improved management of the disease itself and the comorbidities that often complicate its course, such as atherosclerotic disease and infections. In our study, atherosclerosis had an overall SMR of 4.7 with a substantial decrease from 8.3 in the 1980s to 3.2 in the most recent years 2010–2013. Bernatsky et al reported an SMR of 1.7 that remained practically unaltered from 1970 to 2001.16 Similarly, the SMR for cardiovascular causes of death was 2.72 (95% CI 1.83 to 4.04)12 and 2.25 (95% CI 1.30 to 3.89)13 in the two meta-analyses, which were heavily influenced by the study of Bernatsky et al that contributed approximately 67% of the total patients. That can probably be attributed to the different definitions applied. Indeed, Bernatsky et al used the term ‘circulatory’ diseases, which incorporates all diseases of the heart and pulmonary vasculature, even those entities without an atherosclerotic background such as myocarditis or valvular diseases. In contrast, we used only the ICD-10 codes that apply to atherosclerotic disease (either cardiac or cerebrovascular). Bjornadal et al reported an SMR of 2.97 (95% CI 2.78 to 3.16) for coronary heart disease and stroke in Sweden for the period 1964–1995.11
Concerning the infection-related mortality, our findings are similar to those reported by previous studies. The overall SMR was 4.4, quite close to the 4.98 that was reported from both meta-analyses.12 13 Of note, there was a substantial decrease of the SMR from 14.2 in the 1980s to 0.9 in 2010–2013, implying that infections overall did not confer an excessive risk for death in patients with SLE in contemporary years. This finding should be interpreted with caution since the number of deaths was small and the duration of that period (4 years, 2010–2013) was shorter than the other periods (10 years). Regarding malignancies, both meta-analyses reported that the risk of death was not significantly increased in patients with lupus with an SMR of 1.19 (95% CI 0.89 to 1.59) and 1.16 (95% CI 0.57 to 2.36), respectively.12 13 In contrast, we observed an overall SMR of 3.4 from 1971 to 2013 that was decreased and became not significant in 2010–2013 (1.4, 95% CI 0.2 to 2.7). Of note, the two meta-analyses were based on the same two studies11 16 for the extrapolation of the infection-related and malignancy-related SMR.12 13
Interestingly, the all-cause SMR was four times higher in patients 20–39 years of age as compared with those over 40. For infections and malignancies, in particular, the relative risk was 8.6 and 10.6, respectively, while atherosclerosis had a relative risk of 3.1. Furthermore, the all-cause SMR was decreasing for increasing age, and it was similar to that of the general population only for the age group >85 years. These results are in agreement with Bernatsky et al who reported an all-cause SMR of 10.7 for patients <40 years old and 1.4 for patients >60 years old.16 Similarly, Bjornadal et al described an all-cause SMR of 11.1 for patients 20–39 years old that decreased to 2.91 for the individuals who were older than 60.11 A more recent epidemiologic study of the entire female population of the USA showed that SLE was ranking 10th in the causes of death for the ages 15–24 and 14th for the ages 25–34 and 35–44.18
Limitations of the present study include the relatively small number of deaths that does not allow for further categorisation of the patients (eg, men/women, history of renal involvement or not, therapy etc). The medications used for disease management are an important confounder in such outcomes. However, a further subcategorisation of the patients according to their treatment would decrease the sample sizes significantly and influence the statistical power of the analysis. In addition, the lack of ascertainment of the cause of death in 25 patients might have influenced the cause-specific SMRs. Such data (unknown cause of death) are rarely provided in similar reports. In the study of Bernatsky et al,16 763/1255 deaths were attributed to the common causes of circulatory and renal diseases, infections and malignancies. The precise number of deaths with unknown cause (of the 492) was not provided. In our study, the SMR for deaths specifically due to active lupus could not be calculated since this information was not available for the general population. Moreover, the suboptimal reliability of the death certificates must be considered. In a systematic review of 53 distinct autopsy serries, it was reported that a major error (clinically missed diagnosis involving a primary cause of death) occurred in 23.5% (median).19 Of note, the cardiovascular, infectious and neoplastic diseases have shown the highest rates of agreement between clinical diagnoses and autopsy reports (exceeding 90%).20
In conclusion, the all-cause and cause-specific (atherosclerosis, infections, malignancies) SMR for patients with lupus has decreased substantially from the 1970s to recent years. The SMR (all-cause and cause-specific) is significantly higher for younger patients (19–39 years old) as compared with individuals older than 40. There is an excessive risk of all-cause mortality in SLE for all ages except for the age group >85 years.
References
Footnotes
Handling editor Josef S Smolen
Contributors All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published. MU had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding KT is supported by the Lupus Program, Centre for Prognosis Studies in the Rheumatic Diseases.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The study was approved by the University Health Network Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All authors were involved in the study conception and design, acquisition of data, and analysis and interpretation of data.