Article Text

Abstract
Interosseous tendon inflammation (ITI) has been described in rheumatoid arthritis (RA). Whether ITI occurs in at-risk individuals before the onset of clinical synovitis is unknown.
Objectives To investigate, by MRI, ITI in anti-cyclic citrullinated peptide (CCP)-positive at-risk individuals (CCP +at risk) and to describe the anatomy, prevalence and clinical associations across the RA continuum.
Methods Hand MRI was performed in 93 CCP + at risk, 47 early RA (ERA), 28 established ‘late’ RA (LRA) and 20 healthy controls (HC) and scored for ITI, flexor tenosynovitis (TSV) and RA MRI scoring at the metacarpophalangeal joints (MCPJs). Cadaveric and histological studies were performed to explore the anatomical basis for MRI ITI.
Results The proportion of subjects with ITI and the number of inflamed interosseous tendons (ITs) increased along the disease continuum (p<0.001): 19% of CCP +at risk, 49% of ERA and 57% of LRA had ≥1 IT inflamed . ITI was not found in any HC. ITI was more frequently identified in tender MCPJs compared with nontender MCPJs (28% vs 12%, respectively). No IT tenosynovial sheath was identified in cadavers on dissection or histological studies suggesting MRI findings represent peritendonitis. Dye studies indicated no communication between the IT and the joint.
Conclusions ITI occurs in CCP + at-risk individuals and can precede the onset of clinical synovitis. The ITs may be important nonsynovial extracapsular targets in the development and progression of RA.
- early rheumatoid arthritis
- anti-CCP
- MRI
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Individuals at risk of rheumatoid arthritis (RA), including those with anti-cyclic citrullinated protein (CCP) antibodies, often develop musculoskeletal symptoms before the onset of clinical or subclinical synovitis.
MRI tenosynovitis of the flexor tendons is a prevalent finding in at-risk individuals.
There is a high prevalence of interosseous tendon inflammation (ITI) in the hands of patients with established RA.
What does this study add?
MRI ITI may be associated with clinical metacarpophalangeal joint tenderness and could explain symptoms in at-risk individuals who do not have clinical synovitis.
ITI occurs in anti-CCP-positive at-risk individuals without clinical synovitis.
Cadaveric and histological studies show that the interosseous tendons do not have a tendon sheath and do not directly communicate with the joint capsule.
Introduction
Rheumatoid arthritis (RA) is conventionally considered as a disease of the synovial joints. However, individuals at risk of RA (including those with anti-citrullinated protein antibodies, ACPA) often develop musculoskeletal (MSK) symptoms before the onset of clinical synovitis (ie, synovitis determined on physical examination) or subclinical synovitis (ie, synovitis determined on high-resolution imaging but not physical examination).1–3 Extracapsular structures may be important early targets of RA-related inflammation. This may involve the tenosynovium or potentially even tendons without a tenosynovial sheath (ie, peritendonitis). Indeed, tenosynovitis appears to be an early and prevalent MRI lesion in at-risk individuals, both in patients with clinically suspect arthralgia (CSA)4 and ACPA-positive at-risk individuals.5 Tenosynovitis of the wrist and finger flexor tendons is also the strongest predictor of progression to arthritis in patients with CSA.4 Furthermore, tenosynovitis is a frequent presentation of RA, causes significant disability and occurs in remission, where it is predictive of flares.6
Unlike tenosynovitis of the wrist and finger flexor tendons, the involvement of other extracapsular structures critical to hand function has not been completely elucidated. For example, the interosseous muscles of the hands are regarded as the cornerstone of hand function7 and their tendons run adjacent to the metacarpophalangeal joints (MCPJs). Occupation-related overuse injuries of these muscles and their tendons have been described.8 A recent study identified a high frequency of inflammation of the interosseous tendons (ITs) in patients with RA.9 Whether these tendons become inflamed in at-risk individuals and whether they may be responsible for symptoms in these subjects is unknown. We therefore sought to comprehensively investigate interosseous tendon inflammation (ITI) across the RA continuum by describing the anatomy, histology, prevalence and clinical associations in both anti-cyclic citrullinated peptide positive at-risk (CCP +at risk) individuals and patients with RA.
The main aim of this study was to assess whether MRI ITI is present in CCP +at-risk individuals without clinical synovitis. As we hypothesised MRI ITI would be present in CCP +at risk, the secondary aim of the study was to determine whether MRI ITI is associated with clinical features in CCP +at-risk individuals.
Methods
Design
A retrospective analysis of MRI and clinical data of CCP +at-risk individuals, patients with RA and healthy controls (HCs) were undertaken.
In order to understand whether ITI should be considered a tenosynovitis or a peritendonitis, cadaveric and histological studies were performed to explore the anatomical basis for MRI ITI.
Clinical subjects
Anti-CCP-positive at-risk individuals with MSK symptoms but no clinical synovitis (CCP +at risk), disease-modifying anti-rheumatic drug (DMARD)-naïve early RA patients (ERA), established ‘late’ RA patients (LRA) and asymptomatic HC were recruited at Chapel Allerton Hospital, Leeds, UK. Informed consent was received from all subjects.
The Leeds CCP +at risk cohort has been previously described.3 10 Patients aged >18 years presenting to their general practitioners or other health professionals with new-onset MSK symptoms (eg, arthralgia, epicondylitis, subacromial bursitis) but no clinical synovitis were invited to participate. Primary care recruitment was adopted by the UK Primary Care Clinical Research Network. Anti-CCP testing was performed centrally using the commercially available anti-CCP2 (immunocap method; Phadia, Sweden). Those with a positive test were invited to attend a dedicated research clinic in Leeds where recruitment for the current MRI study was undertaken. Patients from the Leeds early arthritis clinic who were anti-CCP positive but did not have clinical synovitis were also recruited.
ERA patients had not received DMARDs at the time of imaging. LRA patients had ≥1 year disease duration (total duration of reported symptoms), were anti-CCP and/or rheumatoid factor positive and had active disease (disease activity score 28≥3.2). These patients had received ≥1 DMARD and underwent MRI prior to receiving rituximab as part of a separate study.11
HCs included staff members from the University of Leeds and members of the local community. None of the controls had any MSK symptoms at the time of recruitment.
Demographic and clinical details were recorded at the time of imaging assessments. All subjects (except HC) underwent MSK examination by a rheumatologist prior to the imaging assessments and swollen and tender MCPJ counts were recorded. Blood testing for C-reactive protein (CRP) was performed at the clinical visit.
MRI
All subjects underwent MRI of the most symptomatic or dominant hand and wrist (see online supplementary materials for full details). For all CCP +at risk, patients with ERA and HC, MRI scans were performed on a 3T Siemans Verio system (Erlangen, Germany). Due to logistical issues, all patients with LRA were scanned on a 1.5T Siemans Avanto (see online supplementary materials for further details of MRI systems). All MRI scans were independently scored for the presence or absence of ITI by two MSK radiologists (AG and ER). The radiologists were blinded to all patient details and studies were presented to them in a random order with respect to disease status. Any discrepancies in scoring between the two radiologists were reviewed at the end of the reporting exercise and a consensus score was agreed. The consensus score was then used in the analysis. ITI was defined as the presence of enhancing tissue surrounding the tendon which was evident in two planes.9 Eight tendons were assessed in each hand (ie, each MRI study): the tendons of the dorsal interossei,1–4 the palmar interossei1–3 and the abductor digiti minimi.
Supplemental material
In addition to IT scoring, all MRI studies were scored for the presence of synovitis, bone marrow oedema (BME) and erosions at MCPJs 2–5 according to the Outcome Measures in Rheumatology RA MRI scoring (RAMRIS) system.12 Tenosynovitis of the flexor digitorum tendons was scored dichotomously as ‘present’ or ‘absent’ in keeping with the dichotomous scoring of ITI. In the majority of studies (including all CCP +at risk studies), RAMRIS and tenosynovitis scoring were performed by the same radiologists that scored ITI (AG and ER), and a consensus score was used in the analysis. However, in a small number of cases, only scores from a single radiologist were available and these were therefore used in the analysis. In all cases, the radiologists were blinded to all patient details and studies were presented to them in a random order according to disease status.
Anatomical study
To assess the relationship between the ITs and the adjacent MCPJ, 20 fresh hand specimens from anonymous donors were obtained (Anatomy Department, Universitat de Barcelona). The first dorsal interosseous muscle and tendon were identified by ultrasound (US) from the myotendinous junction to the capsular insertion. The adjacent second MCPJ was also identified on US. Using US guidance, a green dye (green acrylic paint mixed 50:50 with water) was injected along the IT proximal to its capsular insertion. Similarly, a blue dye (blue acrylic paint mixed 50:50 with water) was injected into the second MCPJ space using US guidance. Specimens were then frozen and transverse sections were made. Ethical approval for this study was obtained by the Universitat de Barcelona, Spain.
To further confirm the absence of a tendon sheath around the ITs, two embalmed adult human cadaver hands were dissected. The distal attachment of the first dorsal IT was identified by dissection and processed for histological analysis (Department of Anatomy and Embryology, Complutense University of Madrid). The specimens were fixed in 10% formalin and embedded in paraffin. Each specimen was sliced as a whole on a single plane. Sections of 7 µm were cut and stained with haematoxylin–eosin and Mallory’s trichrome dye. Additionally, the first dorsal IT insertion was investigated in two human fetuses aged 14 weeks (greatest length 115 mm in both). The specimens belong to the collection kept at the Department of Anatomy and Embryology at UCM. Sections of 12 µm were cut and stained with haematoxylin–eosin. Digital photomicrographs were taken with a Nikon DXM 1200 labour microscope (Nikon Corp., Tokyo, Japan) and edited using Act One and Adobe Photoshop CS6 software. Ethical approval for this study was obtained by Complutense University of Madrid.
Statistical analysis
The number of inflamed ITs was compared between subject groups using a Jonckheere-Terpstra test in order to assess whether the median number of sites increased according to disease along the RA continuum. In all analyses where MRI-detected synovitis, BME and erosions are reported at joint level, only those joints where inflammation scores were over and above that seen in the same anatomical location in symptom-free controls of the same age range were included (ie, true subclinical inflammation).13 Adjustment for symptom-free controls was performed in order to account for the observation that MRI-detected inflammation is prevalent in the general population, especially in older people and at certain anatomical sites, for example, MCPJs 2 and 3.13 True subclinical inflammation was considered to be present if that joint or bone was (i) scored positive for inflammation and (ii) the score obtained at that joint or bone was present in <5% of age-matched symptom-free persons.13 Tenosynovitis could not be adjusted for in this way as this was scored dichotomously (ie, present or absent) rather than semiquantitatively in this study.
Results
Clinical study
Baseline characteristics
In all, 93 CCP +at risk, 47 ERA, 28 LRA and 20 HC were included. The frequency of tender and swollen MCPJs and CRP level increased along the RA continuum with increasing disease duration (table 1). Overall, MRI inflammation (synovitis, tenosynovitis, BME, erosions) at the MCPJs also increased in a similar fashion (see online supplementary materials).
Baseline characteristics of all participants
MRI Interosseous tendon inflammation
MRI ITI was observed as enhancing tissue around the midportion of the tendon, proximal to the enthesis (figure 1). The proportion of patients with ITI increased along the RA continuum (table 2); 18/93 (19%) CCP +at risk, 23/47 (49%) ERA and 16/28 (57%) LRA patients had inflammation of at least one IT. Of note, no ITI was identified in any HC. The number of inflamed IT per patient also increased along the RA continuum (Jonckheere-Terpstra J=5.90, p<0.001). In all patient groups, ITs associated with MCPJ2 and MCPJ5 were most frequently affected (table 2), although trends with respect to increasing ITI prevalence across the groups were similar in all locations. Of note, ITI was identified in both anti-CCP-positive and anti-CCP-negative ERA patients: 17/34 (50%) of anti-CCP-positive ERA patients had ITI compared with 6/13 (46%) of anti-CCP-negative ERA patients. The two radiologists showed an excellent level of agreement for the identification of ITI in this study: kappa (k)=0.893 (SE=0.025), comparable to that demonstrated in the original description of MRI ITI (kappa, k=0.91; SE=0.03).9

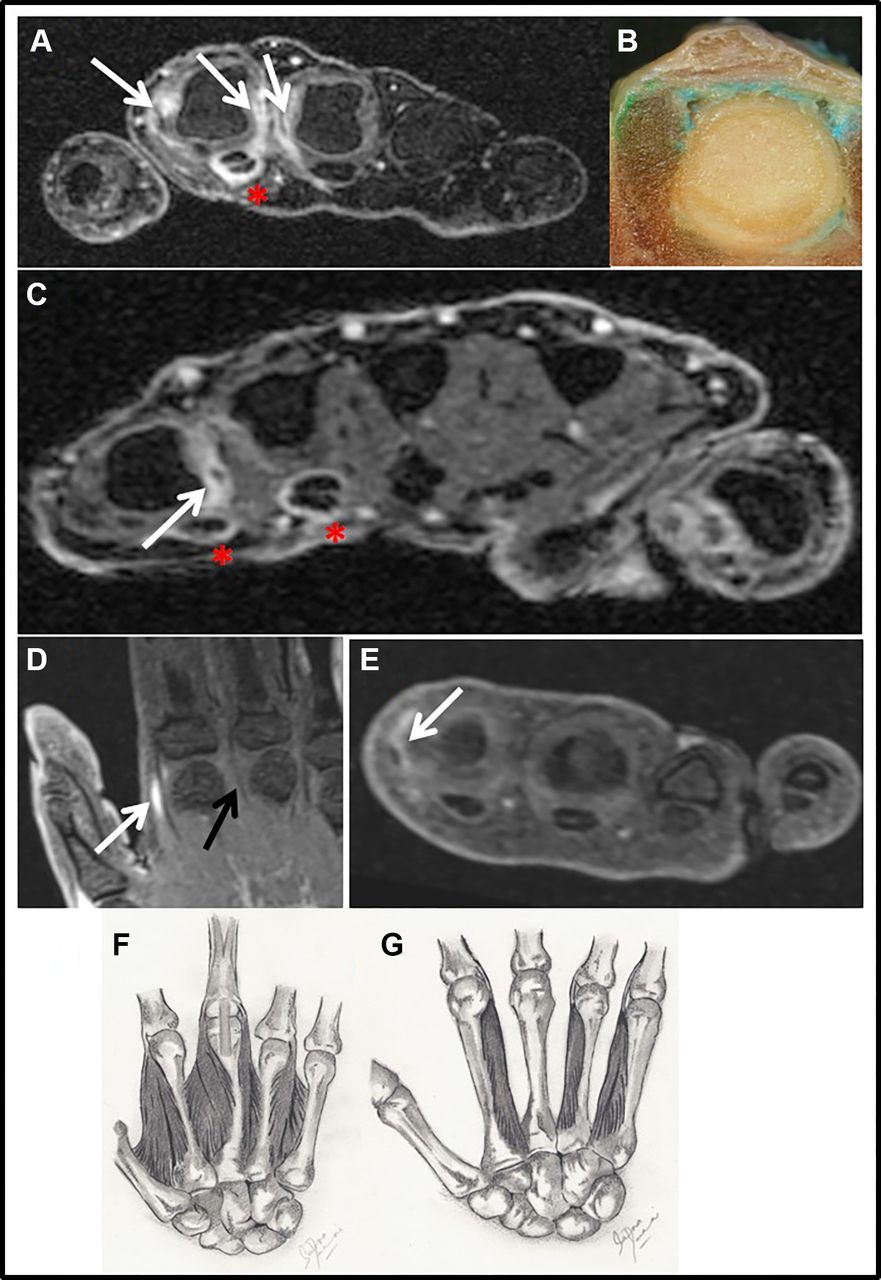
IT inflammation in anti-CCP +at-risk individuals. (A) Inflammation of the first and second dorsal ITs and first palmar IT (arrows). MCPJ inflammation is present at the second and third MCPJs and flexor tenosynovitis of the second finger is also observed (asterix). (B) Transverse section of cadaveric second MCPJ following ultrasound-guided dye injections. Green dye has accumulated around the superficial margin of the interosseous muscle but remains outside the MCPJ capsule. Blue dye injected into the joint remains within the joint capsule. (C) Inflammation of the third palmar IT. Flexor tenosynovitis is also present (asterix). (D) Inflammation of the first dorsal IT (white arrow). There is no inflammation in the adjacent MCPJ or of the second dorsal IT (black arrow). (E) Isolated inflammation of the second dorsal IT (arrow). No adjacent synovitis or tenosynovitis is seen. (F) Illustration of the anatomy of the dorsal ITs of the hand. The interossei originate from the medial and lateral aspects of the metacarpals and attach into the extensor hood and proximal phalanx of each finger. (G) Illustration of the anatomy of the palmar ITs. The three palmar interossei attach to the index, ring and little fingers. CCP, cyclic citrullinated peptide; ITs, Interosseous tendons; MCPJ, metacarpophalangeal joint.
Interosseous tendon inflammation according to RA status
Association between ITI and clinical features
The prevalence of MCPJ tenderness increased with disease duration (tables 1 and 3). ITI was more frequently identified in tender MCPJs compared with nontender MCPJs; 28% of all tender MCPJs had an associated ITI, whereas only 12% of nontender MCPJs had an associated ITI (table 3). Synovitis, BME, erosions and tenosynovitis were also more frequently identified in tender MCPJs compared with nontender MCPJs (table 3).
Clinical and MRI features according to clinical tenderness at MCP joints (MCPJs 2–5) for CCP+ and RA subjects (n=162)
Early morning stiffness (EMS) duration (minutes) was not markedly different in CCP +at risk with ITI (ie, at least one inflamed IT at any site) compared with those without ITI (median IQR 10 (0, 60) vs 5 (0, 10)). Similarly, the presence of synovitis, BME, tenosynovitis or erosions at ≥1 MCPJ did not appear to be associated with EMS duration (online supplementary materials). The number of affected MCPJs was not associated with EMS duration for any of the MRI features.
Anatomical study
Detailed dissection of fresh hand specimens revealed no identifiable synovial tendon sheath around the IT of the cadaveric specimens. Identification of the blue and green dye on transverse sections was achieved in 13/20 (65%) specimens (figure 1b). Blue dye was localised in the intra-articular space and was not seen outside the joint capsule. In contrast, green dye was localised around the ITs and interosseous muscle and was not seen within the joint capsule. These findings suggest an absence of communication between intracapsular synovial membrane and the adjacent IT.
Cadaveric dissection revealing the first dorsal IT and its attachment is shown in online supplementary figure 1. Histological examination of the first dorsal IT from a fetal hand (figure 2A, B) and adult hand (figure 2C–G) confirmed the presence of an epitendon, but no synovial sheath surrounding the tendon could be identified.
Supplemental material

{kind=link}
{kind=link}
Histological examination of the first dorsal IT. (A) Frontal section of the metacarpophalangeal joint of a human fetus (14 weeks after conception) with haematoxylin–eosin staining. (B) High-power magnification of black square in A: 1, superficial first dorsal IT; 2, deep first IT inserting into the base of the proximal phalanx; 3, insertion of the deep tendon of the first interosseous into the joint capsule. MT, second metatarsal head; PH, proximal phalanx; PS, synovial plica; V, blood vessel. (C) Frontal section of the myotendinous junction of the first dorsal IT in an adult cadaver with Mallory’s trichrome stain. The tendon is formed by CF arranged longitudinally. The EPT surrounds the tendon (illustrated by black line). (D) High-power magnification of the square in C shows muscle fascicles separated by endomysium and surrounded by PM. PM is continuous with peritendon that surrounds CF. (E) Frontal section of the distal insertion of the first dorsal IT in an adult cadaver with Mallory’s trichrome stain. 1, Superficial first dorsal IT; 2, deep first dorsal IT. (F) High-power magnification of the black square in E shows the EPT containing blood vessels. There is no tendon sheath surrounding the EPT. (G) High-power magnification of the red square in E. Blood vessels are seen in the EPT with no surrounding tendon sheath. CF, collagen fascicles; EPT, epitendon; IT, interosseous tendon; PM, perimysium
Discussion
Individuals at risk of RA often experience a prodrome of joint pain and stiffness before the onset of clinical synovitis. This may reflect the earliest phase of RA inflammation, which in many cases will progress to full-blown disease. However, the cause of these symptoms and their relevance to disease progression are not clear. Understanding this phase of disease is likely to deliver important insights into pathogenesis and also inform future preventative strategies.
This study is the first to demonstrate that the IT of the hands are inflamed in anti-CCP-positive at-risk individuals and may represent an extracapsular cause for early symptoms in the absence of clinical synovitis. We have also demonstrated that, on cadaveric dissection and histological examination, these tendons do not have a tenosynovial sheath and do not directly communicate with the joint capsule. This, alongside the observation that fluid is not seen around these tendons on MRI,9 suggests MRI ITI represents an additional nonsynovial target of inflammation in the RA continuum (ie, peritendonitis rather than a true tenosynovitis).
ITI was identified in 19% of CCP +at-risk individuals with increasing prevalence with RA disease progression. The number of inflamed tendons in each patient also increased with disease progression. Of note, we did not identify any ITI in the HCs. This is in keeping with the observation that MRI tendon inflammation is rarely seen in healthy subjects.13
The association between specific clinical features (EMS duration, MCPJ tenderness) and MRI inflammation in anti-CCP-positive at-risk individuals has not previously been reported. However, Van Steenbergen et al have previously reported no association between EMS duration and MRI inflammation in individuals with CSA.14 While we found no association between ITI and EMS duration, there was an increased frequency of ITI in tender MCPJs compared with nontender MCPJs. This is an interesting finding, particularly as small joint tenderness is predictive of arthritis development in CCP +at-risk subjects.10 The potential association between clinical features and ITI should be further explored in a prospective study, where IT tenderness and flexor tendon tenderness at the MCPJs could be specifically assessed by clinical examination.
In line with our findings, others have demonstrated that tendon inflammation is prevalent in the hands of patients with early arthritis15 and at-risk individuals.4 5 In these studies, tendon inflammation was mainly characterised by tenosynovitis, although isolated peritendinous inflammation of the digital extensor tendons was described in patients with ERA15; our current data extend the concept of early extracapsular inflammation and suggest nonsynovial tendon inflammation, that is, peritendonitis, may also be an important disease target in at-risk individuals who do not have clinical synovitis.
While the dye injections in our cadaveric study revealed no communication between the IT and adjacent MCPJ, the specimens used were from anonymous donors who did not appear to have RA. It is not known if this would be different in the setting of established RA-related MCPJ inflammation.
Although we have identified ITI as an early feature in the RA disease continuum, it is not clear how specific this lesion is for anti-CCP-related inflammation (or autoimmune-related inflammation). Indeed, we identified a similar prevalence of ITI in anti-CCP-positive ERA patients compared with anti-CCP-negative ERA patients, suggesting ITI is unlikely to be an ACPA-specific phenomenon. Furthermore, although MRI peritendinous inflammation has been reported in established RA, this finding is not necessarily disease specific. It is also possible that ITI may occur due to mechanical factors in some patients with hand arthralgia. Future work should, therefore, investigate whether ITI also occurs in symptomatic anti-CCP-negative patients with arthralgia and also in other rheumatic diseases.
In conclusion, this study has identified MRI inflammation of the hand ITs in CCP +at-risk individuals who do not have clinical synovitis. This lesion was more frequently seen in tender MCPJs compared with nontender MCPJs. These data suggest that the ITs may be an early nonsynovial extracapsular target of RA inflammation. Further longitudinal data are needed to investigate whether ITI predicts the development of clinical and subclinical synovitis in individuals at risk of RA.
Acknowledgments
We would like to thank Dr Daniel Glinatsi, Prof Mikkel Ostergaard and Dr Paul Bird for contributing clinical data. We would like to thank Rob Evans and Brian Chaka for radiography support.
References
Footnotes
Handling editor Josef S Smolen
Contributors KM recruited patients, collected and analysed the data and wrote the manuscript. MADA designed the study and helped prepare the manuscript. ER scored the MRI scans. EMAH led the statistical analysis. LH recruited patients and collected data. IM, MP, JRM, JN and EN performed the cadaveric and histological studies. JLN was one of the study clinicians. ALT and JEF recruited patients and collected clinical data. AJG and PE designed and led the study. All coauthors read and revised the manuscript.
Funding The study was supported by the National Institute for Health Research (NIHR) Leeds Clinical Research Facility.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval NHS Health Research Authority National Research Ethics Service Committee Yorkshire & the Humber – Leeds West.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional unpublished data are currently available.