Article Text

Abstract
Objectives Association between periodontal disease (PD) and rheumatoid arthritis (RA) has been extensively described, but direct evidence of causal involvement of PD in RA is missing. We investigated the priming role of oral Porphyromonas gingivalis (P. gingivalis) in PD and subsequent RA and we assessed biomarkers of bone resorption and arthritis development in rats.
Methods Lewis rats were orally exposed to either P. gingivalis, Prevotella intermedia or control gel for 1 month and then followed for 8 months. The onset and development of PD was assessed by serology, gingivitis severity and micro-CT (µCT). We investigated arthritis development using circulating proinflammatory markers, anticyclic citrullinated peptide (CCP), anticitrullinated protein antibody (ACPA), ankle histology and µCT.
Results PD was only observed in the P. gingivalis treated rats, as early as 1 month postexposure. Joint and systemic inflammation were detected only in the P. gingivalis group after 4 and 8 months. At 8 months, inflammatory cell infiltrate was observed in ankle joints and paralleled cortical erosions and overall cortical bone reduction. Furthermore, anti-CCP2 correlated with local and systemic bone loss.
Conclusions In our long-term study, PD induced by oral exposure to P. gingivalis triggered seropositive arthritis, with systemic inflammation and bone erosions. This is the first in vivo demonstration of arthritis induced by oral priming with P. gingivalis.
- arthritis
- periodontitis
- bone loss
- ACPA
- aetiology
Statistics from Altmetric.com
Key messages
Exact mechanisms explaining the association between periodontal disease and rheumatoid arthritis remain unknown.
Porphyromonas gingivalis, but not Provatella intermedia, induces periodontis and ankle joint inflammation at clinical, biological and histological levels with bone loss and erosion.
Our data reinforce the role of P. gingivalis in arthritis induction.
This model shares some similitude with rheumatoid arthritis: involvement of periodontis and anticyclic citrullinated peptide 2 development.
Introduction
Periodontal disease (PD) and rheumatoid arthritis (RA) are two inflammatory diseases that share many features including local inflammation-induced bone loss.1 Despite clinical association between PD onset and development of RA, few studies have investigated the direct mechanisms. One of the suspected mechanisms in the bacteria-induced PD leading to RA is the development of antibodies at the site of inflammation against citrullinated proteins. Among all the bacteria inducing PD and found during RA,2 Porphyromonas gingivalis (P. gingivalis) was the first identified to induce citrullination. P. gingivalis and gingival citrullinated proteins were previously detected in gingival biopsies from patients with RA, who had also high blood concentrations of anti-P. gingivalis antibodies.3 In addition, correlations between circulating anti-P. gingivalis antibodies and anti-citrullinated protein antibodies (ACPA) were also reported.3 Nevertheless, involvement of P. gingivalis in RA onset is still controversial.4 5 The presence of P. gingivalis or PD exacerbates experimental arthritis, and experimental arthritis exacerbates PD.6 7 A major limitation in these studies is the lack of a demonstrated specific role of a particular PD-inducing bacterium in RA, since any generic proinflammatory stimulation can worsen arthritis burden independently of the role of PD associated organisms. Therefore, we have investigated the effects of oral exposure to P. gingivalis during onset and development of arthritis and compared its effect with Prevotella intermedia (P. intermedia), another gram-negative bacteria also associated with PD.8
Methods
Thirty female Lewis rats were randomly divided into three groups (10 per group) and orally exposed to a carboxymethylcellulose sodium salt gel containing P. gingivalis W50 (ATCC #53978; PG group), P. intermedia (ATCC#25611; PI group) or the gel alone (CTRL group).9 Baseline was defined as the first day of exposure. Animal experiments were performed accordingly to the Animal Research: Reporting of In Vivo Experiments guidelines for the use of laboratory animals. Five rats per group were sacrificed after 1 month and the others at 8 months. Rat in vivo monitoring,10 periodontitis validation, biochemistry assays and determination,11 microcomputed analysis and bone histology methods12 were described in the supplementary methods section. Non-parametric tests were performed with p values under 0.05 considered as statistically significant.
Results
Seropositive periodontitis with alveolar bone crest regression and mandibular bone erosions developed within 8 months only in the PG group
Gingival erythema was observed in the PI and PG groups, while mandible tissue destruction was recorded only in the PG group (figure 1A). One or more large bone erosions (≥600 µm) were only observed in the PG group, mostly localised to the mesial area around the first root of the first molar (M1R1) (figure 1B; online supplementary figure S1A-C). Intra-alveolar osteopenia was only reported in the PG group (online supplementary figure S1D-E;<0.05). Anti-P. gingivalis and anti-P. intermedia antibodies were increased in the serum at 4 and 8 months compared with 1 month in PG and PI groups (figure 1C; p<0.01). Anti-CCP2 antibodies were detected after 4 months in the PG group (figure 1D; p<0.05) with a trend to correlate with anti-P. gingivalis serology (online supplementary S1F; r=0.90, p=0.08). Additionally, comparative immunoglobulin (Ig)M anti-IgG concentrations were higher in the PG group from the end of oral exposure to the end of the experiment (figure 1D; p<0.05). To assess the specificity of anti-CCP2, we detected anti-citrullinated peptide antibodies from 30 peptides citrullinated forms of the beta chain of fibrinogen and detected a positivity for three peptides (figure 1E; p<0.05). However, the uncitrullinated control peptides were also reactive. Following confirmation of PD induction, we investigated the presence of arthritis.
Supplemental material
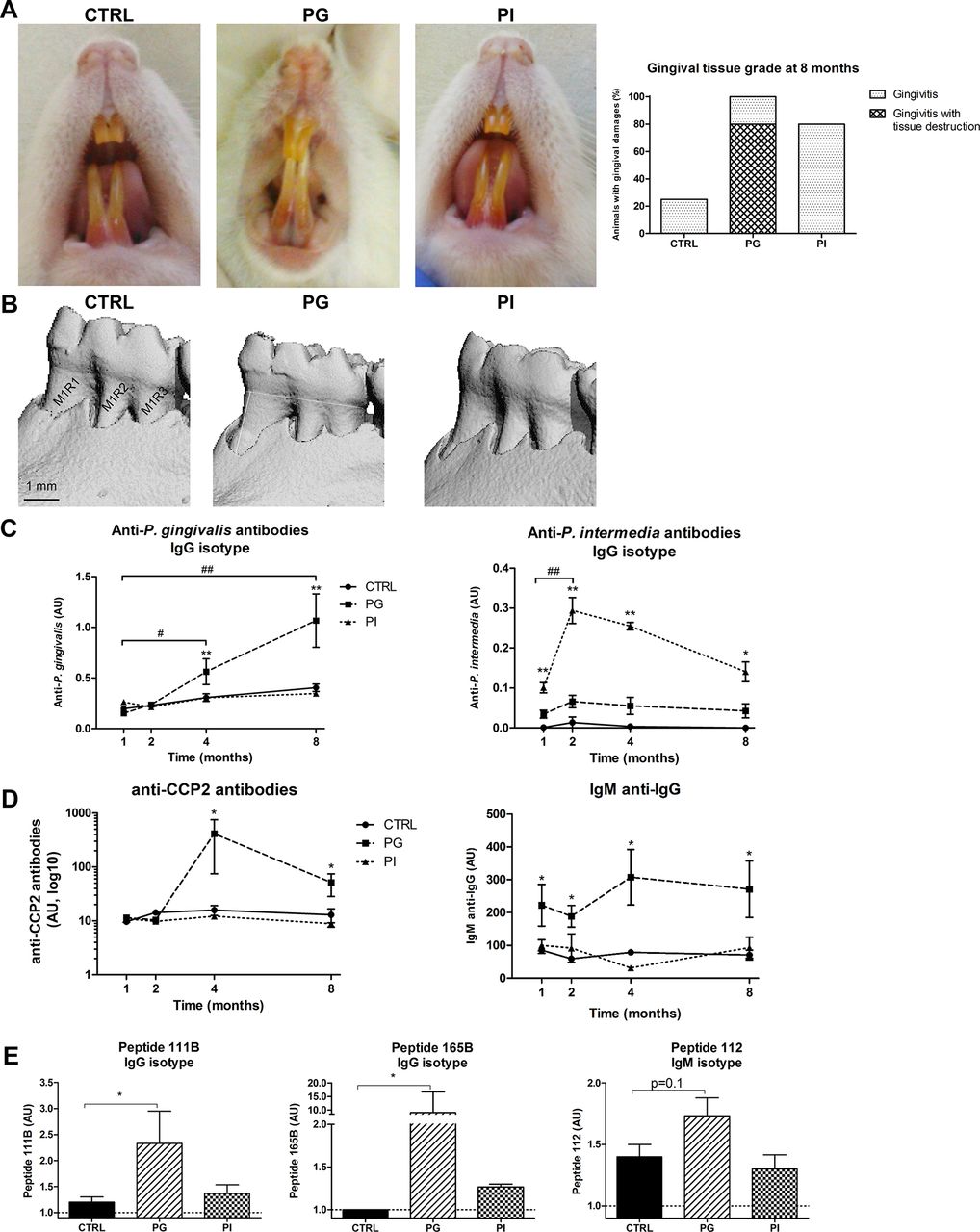
Periodontitis was observed in rats exposed to PG group. (A) Representative pictures of rat mouth: healthy in CTRL (left), gingival missing in PG (middle) and gingival inflamed in PI (right) groups, with gingival tissue scoring (right panel). (B) µCT pictures of mandibles of CTRL (left), PG (middle) and PI (right). CTRL and PG pictures are representative, while the PI rat pictured was the only one with a mandible erosion (≤300 µm). Other PI rat mandibles were similar to CTRL rat mandibles. Scale bar: 1 mm. (C) Immunisation was confirmed with serology assays: anti-P. gingivalis antibodies detection in the PG group and anti-P. intermedia antibodies in the PI group. (D) Strong induction of anti-CCP2 antibodies from 4 months and IgM anti-IgG from 1 month only in PG. (E) Three citrullinated peptides recognised by sera only in PG group. ELISA plates were coated with 30 citrullinated peptides and blocked with BSA. Sera were diluted at 1/80. After washing, peroxidase-conjugated antimurine IgG was added. The OD was read at 405 nm. The background OD was obtained by adding each serum to a well without peptide. Values are means with SEM. Statistics: group effect: *p<0.05, **p<0.01; time effect: #p<0.05, ##p<0.01. ABC, alveolar bone crest; AU, arbitrary units; BSA, bovine serum albumin; BS/BV, bone surface/bone volume; BV/TV, bone volume/tissue volume; CCP-2, circular citrullinated protein peptide 2; CEJ, cement–enamel junction tangents; CTRL, control group; Ig, immunoglobulin; M, molar; µCT, micro-CT; OD, optical density; PG, Porphyromonas gingivalis exposed group; PI, P revotella intermedia exposed group; R, root.
Clinical, biological and histological markers showed joint inflammation in the PG group
Ankle circumferences were higher in rats from the PG group than in other groups at the end of oral infection and also at 4 and 8 months (figure 2A; p<0.05 for months 1 and 4 and p<0.001 for month 8) following normalisation to body mass (which was lower in the PG group at 7 and 8 months) (figure 2B; p<0.05). From month 1 to month 8, interleukin (IL)-17 and CXC ligand 1/cytokine-induced neutrophil chemoattractant-1 (CXCL1/CINC-1) concentrations were higher in the PG animals (figure 2C–D; p<0.05). Finally, histological assessment of ankles for 8 months demonstrated the presence of inflammatory cell infiltrate in the PG rats (figure 2E). Therefore, arthritis was observed at the ankle joint after PD induction by P. gingivalis. We then asked whether bone erosion could be detected.

Only Porphyromonas gingivalis induced all the hallmarks of prearthritis followed by joint inflammation. (A) Ankle circumferences measured with digital callipers increased only in the PG group. (B) Animal body mass was recorded and reported a low weight in the PG group. (C) Serum IL-17 and (D) CXCL1/CINC-1 were highest in the PG group at 1 and 8 months. (E) Inflammatory infiltrate in ankle joints was observed (circle) with H&E staining only in the PG group. Scale bar: 500 µm. Statistics: group effect: *p<0.05, ***p<0.001; time effect: #p<0.05. AU, arbitrary units; CCP-2, circular citrullinated protein peptide 2; CTRL, control group; CXCL1/CINC-1, CXC ligand 1/cytokine-induced neutrophil chemoattractant-1; IL-17, interleukin 17; PG, P. gingivalis exposed group; PI, P revotella intermedia exposed group; ×100, 100 times magnification.
P.gingivalis induced osteoclast activity, bone erosions and quantitative bone loss in the ankle
Tartrate-resistant acid phosphatase+osteoclast number was elevated in the ankles of the PG rats (figure 3A–B). Bone erosions were detected in the cortical layer of the ankle bones of the PG rats as measured by micro-CT (µCT), especially the navicular bone. These changes were not found in the PI or CTRL groups (figure 3C). PG rats showed significantly higher cortical porosity (Ct.Por) and lower cortical thickness (Ct.Th) (figure 3D; p<0.05), and although the data did not reach significance, displayed reduced trabecular number (Tb.N) and increased trabecular separation (Tb.Sp) (figure 3E; p=0.06 and 0.11). At 8 months, anti-CCP2 correlated with a strong trend (given the small number of experimental animals) with the mandibular tissue mineral density (TMD) loss (figure 3F left), ankle Ct.Por (middle) and ankle Tb.N (right). Thus, higher levels of anti-CCP2 were associated with alveolar bone loss and ankle bone loss. Moreover, anti-CCP2 levels at 4 months were predictive of mandibular and joint bone loss at 8 months (mandibular TMD changes (figure 3G left) ankle Ct.TMD (figure 3G middle) and ankle Tb.N (figure 3G right); r=−0.78, p=0.04).

{kind=link}
{kind=link}
{kind=link}
(A) Increased staining of TRAcP+osteoclasts (purple) in the PG group. (C) Representative µCT 2D images of ankle erosions (white arrows) in the PG group at 8 months. Osteoclast activity and microarchitecture parameters alterations were enhanced in the PG group. Scale bar: 100 µm. (B) Osteoclast analysis included Oc/S/BS and Oc.Le. (C) µCT analysis for cortical and trabecular navicular bone. (D) Cortical µCT analysis included Ct.Por and Ct.Th. (E) Trabecular analysis included Tb.N and Tb.Sp. (F) Correlation assessment of anti-CCP2 with local and systemic bone loss at 8 months, together with prediction of anti-CCP2 at 4 months. Correlations were tested at 8 months between anti-CCP2 and mandibular TMD, ankle Ct.Por and ankle Tb.N in the PG group only. Spearman correlations: rS. (G) Linear regression (coefficient: r; *p<0.05) at 4 months provided insights in anti-CCP2 prediction to (D) mandible TMD, (E) ankle Ct.TMD and (F) ankle Tb.N. Statistics: group effect: *p<0.05, **p<0.01. CCP, citrullinated cyclic peptide; CTRL, control group; Ct.Por, cortical porosity; Ct.Th, cortical thickness; µCT, micro-CT; Oc/S/BS, osteoclast surface/bone surface; Oc.Le, osteoclast length; PG, Porphyromonas gingivalis exposed group; Pi, P revotella intermedia exposed group; Tb.N, trabecular number; Tb.Sp, trabecular separation; TMD, tissue mineral density; TRAcP, tartrate-resistant acid phosphatase.
Discussion
Epidemiological associations between PD, induced by periodontopathogenic bacteria, and rheumatoid arthritis (RA) have been largely described, but reproducible animal models to investigate the direct relationship between PD and RA are desperately needed. Herein, we define a novel model of PD-induced RA and that oral exposure to P. gingivalis induces severe PD, leading to elevations of anti-CCP2, IL-17 and CXCL1 levels and subsequent synovial inflammation and bone destruction. We also show that oral exposure to P. gingivalis induces deep mesial erosions of M1R1, which is the major local consequence of oral exposure to P. gingivalis, consistent with prior reports.13 Finally, compared with P. intermedia, exposure to P. gingivalis induced overt PD in Lewis rats, while P. intermedia resulted in mild gingivitis with small erosions on mesial periodontal bone.
The contribution of P. gingivalis to protein citrullination in the pathogenesis of PD and subsequent anti-CCP2 production in RA has already been documented, but the data is conflicting.14 In our model, anti-CCP2 was detected in the serum 4 months after PD induction, and at the same time as anti-P. gingivalis antibodies. The identified citrullinated epitope detected was similar to those recently observed in a model of T cell immunisation to PAD in mice.11 These recognised peptides encompassed resides 420–479 of the beta chain of human fibrinogen. Moreover, expression of these two markers was correlated at all times only in the PG group, demonstrating its specificity to P. gingivalis exposure. However, we were not able to demonstrate specificity against citrullinated sequence compared with non-citrullinated sequence, as previously reported in rodents.15 Our rat model also mimics the results observed in human RA disease where IgM anti-IgG and anti-CCP2 are elevated and correlated with anti-P. gingivalis antibodies.16
Rat ankle bone loss following oral P. gingivalis exposure was observed after 8 months of initial P. gingivalis exposure. P. gingivalis induced is comparable to the bone loss observed during other experimental RA models such as the rat adjuvant-induced arthritis model.17 As in patients with RA, bone loss was mostly related to osteoclast activation. PG rats bone was less impacted when compared with the cortical bone. The animals with greater alterations in bone parameters were those with earlier anti-CCP2 positivity. Therefore, we successfully correlated anti-CCP2 levels with ankle bone loss. Moreover, anti-CCP2 at 4 months could efficiently predict reduction in bone mass, confirming that ACPA is not only a good biomarker, but might also be directly involved in the mechanisms leading to bone loss. P. gingivalis exposure led to anti-CCP2 production and subsequent bone resorption. This is consistent with previous studies of ACPA administration to healthy mice where ACPA showed high affinity to the bone marrow site18 and led to a reduction in bone mass.19 In line with this findings, marginal jawbone loss was associated with presymptomatic ACPA-positive subjects.20 Finally, ACPA increased the expression of CXCL1/CINC-1 in mouse osteoclasts cultures.18 Therefore, our PG rat model mimics this sequence of RA development. Biofilms in PD are composed of several strains, with P. gingivalis and P. intermedia considered as the most aggressive organisms in these films. However, involvement of other bacteria from the red complex associated to P. gingivalis was not excluded. Given the role of P. gingivalis as a major cause of PD and PD-induced arthritis, the consequences of exposure to P. gingivalis and co-infection with other oral pathogens remain to be investigated.
Supplemental material
References
Footnotes
Handling editor Josef S Smolen
Contributors GC, MRG, VBB, SP and HM designed the study. GC, MRG, IA and RC performed the experiments. GC, LM, IA, SP and HM analysed the data. GC and HM wrote the manuscript. All authors approved the final version.
Funding This work was funded by Aide à la Recherche médicale de proximité (AIRE) and Aide à la Recherche Médicale Ondaine et Environs.
Competing interests HM reports grants, personal fees and non-financial support from Pfizer, grants, personal fees and non-financial support from AbbVie, grants, non-financial support and other from Nordic Pharma, grants, personal fees and non-financial support from MSD, grants and other from UCB, personal fees and non-financial support from BMS, personal fees, non-financial support and other from Novartis, personal fees from Roche Chugai, personal fees from Janssen, personal fees from Biogen, personal fees from Biogaran, grants, personal fees and other from Sanofi, outside the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.