Article Text

Abstract
Objectives To assess the risk of losing remission, low disease activity (LDA) or radiographic progression in the case of (1) discontinuing or (2) tapering doses of biological disease-modifying antirheumatic drugs (bDMARDs) compared with continuation of the initial treatment regimen in rheumatoid arthritis (RA) patients with remission or LDA.
Materials and methods A systematic literature analysis was carried out through May 2017 on the PubMed, Embase, Cochrane and international congress databases, selecting controlled trials comparing bDMARDs discontinuation/tapering versus continuation in RA patients with remission or LDA. The meta-analysis assessed the risk ratio (RR) and 95% CI of losing remission or LDA and the risk of radiographic progression after (1) discontinuing and (2) tapering doses of bDMARDs versus continuing the initial treatment.
Results The meta-analysis comparing bDMARDs discontinuation versus continuation performed on nine trials showed an increased risk of losing remission (RR (95% CI)=1.97(1.43 to 2.73), P<0.0001) or LDA (RR (95% CI)=2.24(1.52 to 3.30), P<0.0001) and an increased risk of radiographic progression (RR (95% CI)=1.09(1.02 to 1.17), P=0.01) in case of bDMARD discontinuation. The meta-analysis comparing bDMARDs tapering versus continuation performed on 11 trials showed an increased risk of losing remission (RR (95% CI)=1.23(1.06 to 1.42), P=0.006) but no increased risk of losing LDA (RR (95% CI)=1.02 (0.85 to 1.23), P=0.81) nor any increased risk of radiographic progression (RR (95% CI)=1.09(0.94 to 1.26), P=0.26) in case of bDMARD tapering.
Conclusion Discontinuation of bDMARDs leads to an increased risk of losing remission or LDA and radiographic progression, while tapering doses of bDMARDs does not increase the risk of relapse (LDA) or radiographic progression, even though there is an increased risk of losing remission.
- rheumatoid arthritis
- das28
- dmards (biologic)
Statistics from Altmetric.com
Introduction
Optimum care for rheumatoid arthritis (RA) is necessary to prevent joint destruction and to reduce functional disabilities. According to the latest European recommendations,1 treatment strategy should be based on (1) early treatment, (2) frequent and regular assessment of disease activity (or ‘tight control’)2 and (3) treatment intensification until a satisfactory level of disease activity is obtained (‘treat-to-target’ strategy).3
By analogy to the treatment strategies used in diabetes, dyslipidaemia and hypertension, treatment objectives have been proposed for RA care. Even though the objective to achieve is still being extensively debated4 and many definitions of remission have been proposed, the recommendations for RA care encourage remission (DAS28-ESR <2.6) as the goal or, failing that, low disease activity (LDA) (DAS28-ESR <3.2).5 6
While the lowest activity level possible should be maintained to limit radiographic progression,7 it is legitimate to question the need to maintain intensive treatment once stable remission has been obtained.8 The latest European1 and American9 recommendations propose a decrease or even discontinuation of biological disease-modifying antirheumatic drugs (bDMARDs) for patients with RA in persistent remission, after having tapered glucocorticoids, in order to decrease the risk of serious infections10 and to reduce the costs of bDMARDs.11
A systematic analysis of the Cochrane Library12 performed in 2014, including seven studies (1203 patients) focused on two antitumour necrosis factors (TNFs) (adalimumab and etanercept), estimated that anti-TNF tapering appears as effective as continuing anti-TNFs in terms of clinical effectiveness and disability, although there is minimal radiographic progression. However, discontinuing anti-TNF was associated with worse functional and radiographic outcomes. Another systematic analysis of the literature,13 including 15 studies focused on various anti-TNF agents, assessed the occurrence of flare-ups at approximately 30% after discontinuing or tapering anti-TNFs.
To investigate the risk of losing remission, LDA or radiographic progression in case of bDMARD discontinuation or tapering compared with the continuation of the initial treatment regimen, in RA in remission or LDA, we carried out a systematic analysis of the literature with a meta-analysis.
Methods
This meta-analysis is reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols statement.14
Article selection process
We carried out a systematic analysis of the literature looking for prospective controlled trials studying the reduction or discontinuation of bDMARDs (except for rituximab) in patients with RA in stable remission or LDA. The PubMed, Embase and Cochrane databases were consulted through May 2017 using a Boolean association of keywords (see online supplementary text). Abstracts from articles submitted to international conferences for the past 10 years (American College of Rheumatology, European League Against Rheumatism (EULAR) and Société Française de Rhumatologie) were also taken into account.
Supplementary file 1
This search was carried out independently by two investigators in Toulouse (SH) and Montpellier (NF) in December 2014, and then updated independently by two investigators in Toulouse (SH and AC) through October 2017. The article inclusion criteria applied to the title and abstract reading were: (1) studies involving RA; (2) prospective controlled trials, randomised or not; (3) studies comparing bDMARDs (all bDMARDs except rituximab) discontinuation, bDMARD tapering (meaning dose reduction or spacing, according to the last EULAR recommendation terminology1) versus continuation of the initial treatment regimen; and (4) patients included in the studies had to be in remission or LDA under bDMARDS before bDMARD discontinuation or tapering. The other inclusion criteria applied after full-text reading were: (1) the bDMARD tapering protocol had to be described in the trial; (2) the endpoints assessed had to be at least one of the following: evidence of a flare, loss of remission, loss of LDA or structural progression defined by a total Sharp score progression ≥0.5. The study covered all bDMARDs except for rituximab because of the wide range of retreatment protocols available for this particular bDMARD. There were no restrictions concerning disease duration, time spent in remission or LDA, duration of treatment or concomitant use of conventional synthetic disease-modifying antirheumatic drug (csDMARDs). The limits were English or French language. The exclusion criteria were: (1) retrospective trials, (2) trials that did not include a control arm (continuation of the initial treatment regimen), (3) trials studying rituximab; and (4) trials tailoring the bDMARD regimen for a reason other than achieving remission or LDA.
Data extraction
Data collection was performed using a predefined standardised grid. The specific collected data are available in online supplementary text. If data were missing in the article, the corresponding authors were contacted by email.
Study quality assessment
Risk of bias was assessed using the Cochrane Collaboration’s assessment tool and is available in online supplementary text.15
Analyses
For the meta-analysis, the estimated event was the number of patients who had not maintained remission or LDA in each treatment group (discontinuation or tapering vs continuation of the initial treatment regimen). A risk ratio (RR) was estimated for each study included in the meta-analysis. All meta-analyses were performed using the inverse variance approach, which assumes a fixed effect model, to determine the weight given to each study. This provided a common weighted RR estimate with a 95% CI, taking into account the weight of the different samples. RRs and 95% CIs were shown on forest plots. Statistical heterogeneity among the selected studies was tested on the basis of the Q-test (χ²), using a significant level of 0.05, and reported with the I² statistic in which high values of I², ranging from 0% to 100%, represent strong heterogeneity. In case of significant heterogeneity, a random effect model was applied to reduce heterogeneity. Bias of publication were searched using funnel plots and Egger test. All computations were performed using the RevMan V.5.1.6 software package developed by Nordic Cochrane Centre (Review Manager (computer program), V.5.1. Copenhagen: The Nordic Cochrane Centre, the Cochrane Collaboration, 2011). P values lower than 0.05 were considered significant.
Results
Study selection
The literature search could identify 13 published articles16–28 and four abstracts29–32 that could be used in the meta-analysis (figure 1). Nine published articles16 18 20–23 25 26 28 concerned a bDMARD discontinuation strategy. Seven published articles17 19 21 24–27 and four abstracts29–32 concerned a bDMARD tapering strategy (decreasing dose or spacing strategy) (table 1).

Flow chart of the selected studies. ACR, American College of Rheumatology; EULAR, European League Against Rheumatism; SFR, Société Française de Rhumatologie.
Characteristics of published articles and abstracts ((ABSTRACT)) selected for the meta-analysis
We contacted four corresponding authors by email17 19 31 32 who answered the authors, in order to obtain missing data on the number of relapsed patients or 12-month data instead of 18-month data.
BbDMARDs were introduced in case of MTX-inappropriate response in seven studies,19 21–23 28–30 in MTX-naïve patients in three studies20 26 27 and data about csDMARD intake before the trial was not available in seven studies.12 16–18 31 32 The bDMARD targeted objective was remission in six studies,19 22 23 27–29 LDA in four studies20 21 26 32 and not noticed in seven studies.12 16–18 25 30 31
Study quality assessments and risk of publication bias
The assessment of the quality of the studies and risk of bias are presented in online supplementary table S1 and figures S2.16
Clinical and structural results of meta-analysis on studies comparing bDMARD discontinuation versus bDMARD continuation
Among the nine articles studying bDMARDs discontinuation after achieving LDA or remission,16 18 20–23 25 26 28 1054 patients continued bDMARDs and 766 patients discontinued bDMARDS. The monitoring period was 1 year for all studies. Three articles concerned adalimumab,16 20 23 three concerned etanercept,21 25 28 one concerned abatacept,22 one concerned certolizumab pegol26 and one concerned various anti-TNF.18 Six studies concerned established RA, and three studies concerned recent RA. Five studies provided data on radiographic progression at 1 year20–22 26 28; however, one study28 could not be used for the meta-analysis because of insufficient data.
Discontinuation of bDMARDs was associated with an increased risk of losing remission (RR (95% CI)=1.97 (1.43 to 2.73), P<0.0001) in comparison with bDMARD continuation with 60% of heterogeneity, even when using a random model (P=0.02) (figure 2A). The loss of remission was observed in 57.2% of patients who discontinued treatment versus 28.8% of patients who continued. The risk of losing remission after bDMARD discontinuation was lower among patients with recent RA (45%) than among patients with established RA (66.1%).

Risk ratio (95% CI) of losing remission, LDA or structural progression after bDMARD discontinuation in comparison with bDMARD continuation. (A) Risk ratio (95% CI) of losing remission after bDMARD discontinuation in comparison with bDMARD continuation. (B) Risk ratio (95% CI) of losing LDA after bDMARD discontinuation in comparison with bDMARD continuation. (C) Risk ratio (95% CI) of structural progression after bDMARD discontinuation in comparison with bDMARD continuation. bDMARD, biological disease-modifying antirheumatic drugs; LDA, low disease activity.
Discontinuation of bDMARDs was associated with an increased RR (95% CI) of losing LDA (RR (95% CI)=2.24 (1.52 to 3.30), P<0.0001) in comparison with bDMARD continuation. Heterogeneity was significant even after using a random effect model (I²=80%) (figure 2B). The loss of LDA (DAS28 >3.2) was observed in 49.9% of patients after discontinuation of treatment versus 21.1% of patients who continued. The risk of losing LDA after bDMARD discontinuation was lower among patients with recent RA (37.22%) than among patients with established RA (52.6%).
Discontinuation of bDMARDs was associated with an increased RR (95% CI) of radiographic progression (RR (95% CI)=1.09 (1.02 to 1.17), P=0.01) in comparison with bDMARD continuation. There was no heterogeneity (I²=0%) (figure 2C).
Since two studies were observational controlled studies with no randomisation,22 23 a sensibility analysis was performed removing these two studies (online supplementary figure S3). However, this new analysis did neither modify the direction of the results nor the heterogeneity.
Clinical and structural results of meta-analysis on studies comparing bDMARD tapering versus bDMARD continuation
Among the 11 articles studying bDMARD tapering after achieving LDA or remission,17 19 21 24–27 29–32 755 patients continued bDMARDs and 835 patients reduced bDMARD dose. Four studies investigated a dose spacing strategy,17 24 26 31 while seven studies investigated a dose decreasing strategy.19 21 25 27 31 Four articles concerned etanercept,19 21 25 29 one concerned adalimumab,32 one concerned abatacept,27 one concerned certolizumab pegol,26 three concerned various anti-TNF17 24 30 and one abstract concerned tocilizumab.31 The monitoring period was 6 months for three studies,29 30 32 12 months for five studies21 25–27 31 and 18 months for three studies.17 19 24 After correspondence with the authors, we obtained 12-month data (instead of 18 months) for two studies.17 19 Five studies concerned established RA,17 19 21 24 25 two studies concerned recent RA26 27 and four abstracts did not contain any information about the duration of RA.29–32 Radiographic data were available for five studies.17 21 24 26 32
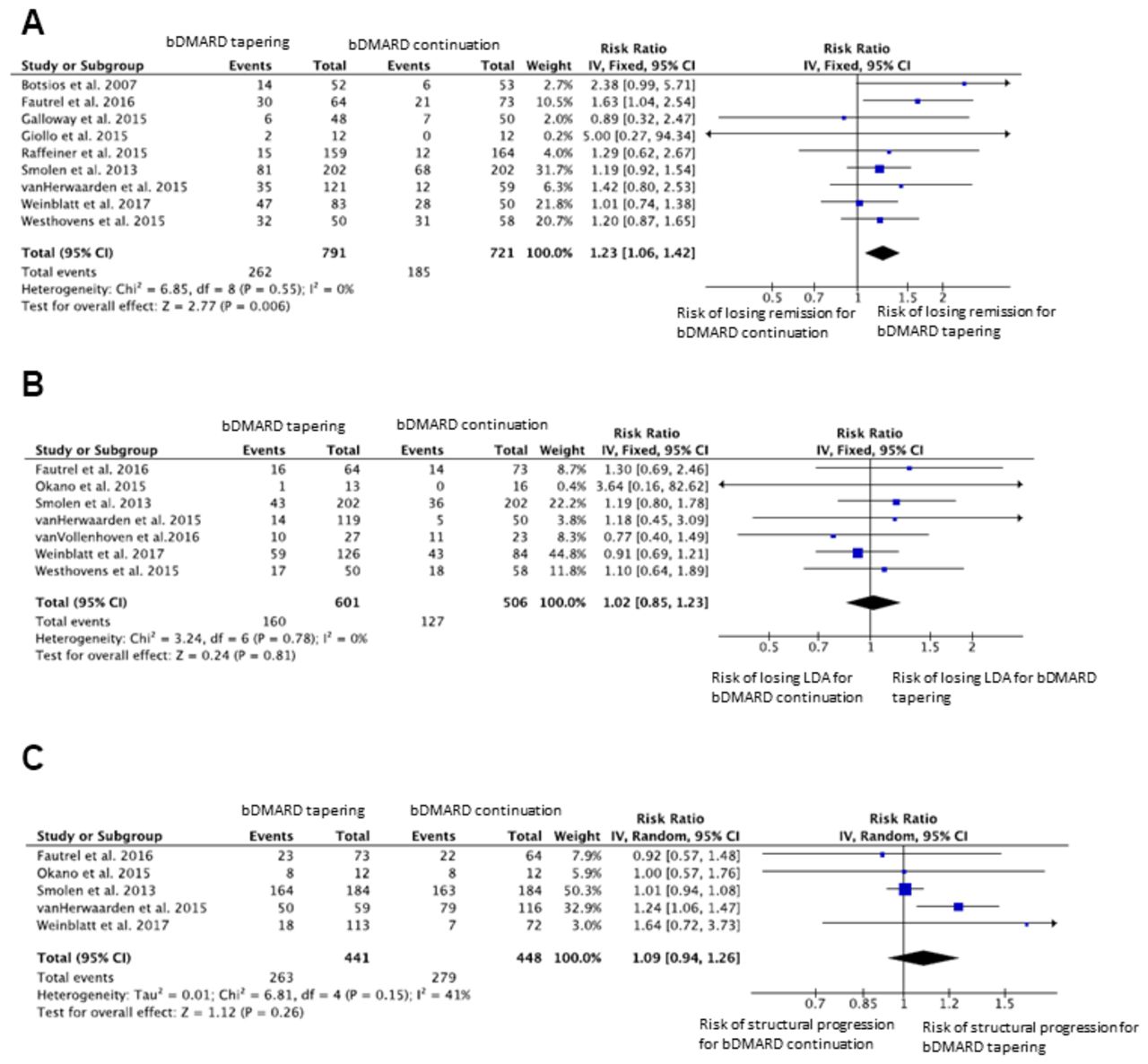
Tapering the dose of bDMARDs was associated with a statistically significant increase in the risk of losing remission (RR (95% CI)=1.23 (1.06 to 1.42), P=0.006) in comparison with bDMARD continuation with no heterogeneity (I²=0%) (figure 3A). A loss of remission was observed in 33.1% of patients who tapered bDMARD dose versus 25.7% of the patients who continued treatment. As one abstract used in this analysis was presented on 2007 and not published, another analysis was performed removing this abstract (online supplementary figure S4) and did not modify the direction of the results.
{kind=link}
{kind=link}
{kind=link}
Risk ratio (95% CI) of losing remission, LDA or radiographic progression after bDMARD tapering in comparison with bDMARD continuation. (A) Risk ratio (95% CI) of losing remission after bDMARD tapering in comparison with bDMARD continuation. (B) Risk ratio (95% CI) of losing LDA after bDMARD tapering in comparison with bDMARD continuation. (C) Risk ratio (95% CI) of radiographic progression after bDMARD tapering in comparison with bDMARD continuation. bDMARD, biological disease-modifying antirheumatic drugs; LDA, low disease activity.
Tapering the dose of bDMARDs was not associated with a statistically significant increase in the risk of losing LDA (RR (95% CI)=1.02 (0.85 to 1.23), P=0.81) in comparison with bDMARD continuation with no heterogeneity (I²=0%) (figure 3b). LDA was lost in 26.6% of patients who tapered bDMARD dose versus 25.1% of patients who continued treatment.
Tapering the dose of bDMARDs was not associated with an increased RR (95% CI) of radiographic progression (RR (95% CI)=1.09 (0.94 to 1.26), P=0.26) in comparison with bDMARD continuation with moderate heterogeneity (I²=41%) (figure 3C).
Risk factors of losing or maintaining remission or LDA after bDMARD discontinuation or tapering
Six studies presented in online supplementary table S5 looked for predictive factors for maintaining or losing remission or LDA after bDMARD discontinuation or tapering.17 18 22 23 25
Clinical results of bDMARD readministration after loss of remission or LDA
Eight articles studied the readministration of bDMARDs after a loss of remission or LDA: 40.8%–91% of patients returned to remission after variable monitoring periods (3–12 months).16–19 23 25–27 There was no increase in the number of adverse events, notably allergic reactions, reported after bDMARD readministration.
Discussion
The present meta-analysis assessed the risk of losing remission, LDA and structural progression in cases of bDMARD discontinuation or tapering compared with the continuation of the initial treatment regimen, in RA in remission or LDA. Whereas discontinuation of bDMARDs exposes the patient to an increased risk of relapse and radiographic progression, tapering doses of bDMARDs does not increase the risk of losing LDA, nor the risk of radiographic progression, even though there is an increased risk of losing remission, in comparison with continuation of the initial treatment regimen.
Our meta-analysis enabled us to identify 17 controlled therapeutic trials studying the discontinuation or tapering dose of bDMARDs in patients with RA in remission or LDA. Most of these studies were of good methodological quality, although two studies were not randomised, leaving discontinuation of bDMARDs up to the patient.22 23 The absence of randomisation can be justified, as is the case in the HONOR study,23 by the wish not to impose strategies that have not yet proved their worth on patients or for a prospective exploitation of the data related to discontinuation of a bDMARD imposed by the end of a therapeutic trial. Seven studies were open studies16–18 22–24 28 due to a spacing dose strategy or a ‘treat-to-target’ strategy, which requires knowledge of the treatment used.
Two recent articles33 34 were not included, because they did not meet the inclusion criteria. In the HOPEFUL 2 study,34 only 85% of the patients in the discontinuation group and 84% in the continuation group were in remission at the time of biotherapy discontinuation. In the RETRO study,33 only 40.6% of the patients were receiving bDMARDs. We contacted the corresponding author who provided us the rate of relapse in this specific population. The rate of loss of remission after bDMARD discontinuation was higher in our meta-analysis (42.8% in the RETRO study vs 56.7% in our meta-analysis), which may potentially be explained by the fact that the RETRO study protocol called for a 50% dose reduction for 6 months before total discontinuation of the bDMARD.
There were disparities on the methodological issues of the studies included in our meta-analysis. The first one concerns the duration of RA: one article on discontinuation20 and three articles26–28 concerned recent RA, while the others concerned established RA.16 17 19 22–25 It appears that the risk of losing remission is lower after the discontinuation of bDMARD in patients with recent RA in comparison with established RA (45% vs 66%), although it is not possible to draw any formal conclusion due to the small volume of data. The second one concerns the type of bDMARDs: 15 studies involved anti-TNF agents,16–21 24–26 28–30 32 34 two involved abatacept22 27 and one involved tocilizumab.31 It is possible that the bDMARD itself may have an impact on the risk of relapse, but we have too little data to answer this question. The third one concerns the follow-up period after bDMARD discontinuation or tapering. While all the studies on bDMARD discontinuation had a 12-month duration, there was a certain degree of heterogeneity in the length of the monitoring period among the different tapering studies. Thanks to the help received from BF (STRASS study)17 and BR,19 we were able to get 12-month data for these two studies.
Our meta-analysis shows an increased risk of losing remission or LDA after discontinuation of bDMARDs in comparison with the continuation of the initial treatment regimen. These results reinforce those of the meta-analysis published by the Cochrane Library,12 in which there was a reduction in the probability of maintaining LDA in case of anti-TNF discontinuation (RR (95% CI)=0.43 (0.27 to 0.68), P=0.00004). Our meta-analysis reveals no statistically significant increase in the risk of losing LDA, even though there was a significant increase in the risk of losing remission, after bDMARD dose reduction in comparison with the continuation of the initial treatment regimen. These results differ from those of the meta-analysis published by the Cochrane Library,12 which showed a lower probability of maintaining LDA when bDMARD doses were reduced (RR (95% CI)=0.87 (0.78 to 0.98), P=0.02). These differences might be explained by the fact that our meta-analysis includes 17 articles, 9 of which were not available when the Cochrane Library undertook its systematic analysis of the literature in September 2013. The results of another meta-analysis13 published in 2015 suggested that tapering or stopping bDMARDs was possible in more than one-third of patients in LDA or remission; however, there was a high level of heterogeneity due to the simultaneous inclusion of anti-TNF discontinuation studies and anti-TNF dose reduction studies, whether retrospective or prospective.
Furthermore, our meta-analysis shows that the discontinuation of bDMARDs exposes the patient to an increased risk of radiographic progression, while reducing doses of bDMARDs does not increase this risk, in comparison with continuation of the initial treatment regimen. Only one article21 included in the Cochrane Library’s meta-analysis provided data on radiographic progression, whereas we were able to include seven articles containing data on radiographic progression.17 20–22 24 26 32 The length of the monitoring periods in the studies varied between 6 months and 18 months, which is probably too short to be able to reliably interpret the radiographic data. The results of the meta-analysis on radiographic progression after discontinuation of treatment have borderline statistical significance, but differences in structural progression values are minimal and have questionable value in terms of the clinical relevance and metrological performances of the radiographic scores.
Our meta-analysis reveals that, in RA patients with remission or LDA, discontinuation of bDMARDs leads to an increased risk of losing remission or LDA and radiographic progression, while tapering doses of bDMARDs does not increase the risk of relapse (LDA) or radiographic progression, even though there is an increased risk of losing remission, in comparison with continuation of the initial bDMARD regimen. Given the increased risk of infections attributable to the higher doses10 and the direct cost of bDMARDs,35 36 a dose reduction strategy (lowering or spacing doses) appears to be a reasonable option for patients with RA in stable remission or LDA.
Acknowledgments
We are grateful to the professors and organisers of ASLER seminary (for Systematic Analysis of the Literature in Rheumatology) for their useful advice in the writing of this manuscript. We wish to thank Abbott who provided logistic support in the organisation of sessions about the implementation of a meta-analysis and remained independent of the collection, analysis and interpretation of data. We are grateful to Professor G Schett, who provided us additional data from the RETRO study.
References
Footnotes
SH and AR-W contributed equally.
Handling editor Josef S Smolen
Contributors SH and ARW equally contributed to the conception of the study, the article selection process, the data collection, the data analysis, the results interpretation and the manuscript writing and approval. CL and NF contributed to the conception of the study, the article selection process and data collection. TB was in charge of the statistical analyses. BF, BR and MR sent additional data from their trials that permitted to improve the data pooling. YD, AC and ARC contributed to the conception of the study, results interpretation and manuscript approval. All authors take responsibility for the integrity of the work as a whole, from inception to published article, and they should indicate that they had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. They give permission to reproduce published material, report sensitive personal information, to use illustrations of identifiable persons, or to name persons for their contributions.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Ethics Committee approvals of each trial was obtained for all the studies selected in this meta-analysis.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement This study involved only published reports and none unpublished information. No database was used for this study.