Article Text

Abstract
Background There is significant unmet need in patients with ankylosing spondylitis (AS) who have inadequate response or intolerance to anti-tumour necrosis factor (TNF) treatment. Secukinumab, an anti-interleukin-17A monoclonal antibody, significantly improved signs and symptoms of AS in the MEASURE 2 study (NCT01649375).
Methods Subjects with active AS (N=219) received secukinumab (150 or 75 mg) or placebo at baseline, weeks 1, 2, 3 and 4, and every 4 weeks thereafter. Randomisation was stratified by prior anti-TNF use: anti-TNF-naive or inadequate response/intolerance to one anti-TNF (anti-TNF-IR). The primary endpoint was Assessment of SpondyloArthritis International Society criteria (ASAS) 20 at week 16.
Results At week 16, 68.2% of anti-TNF-naive subjects treated with secukinumab 150 mg achieved ASAS20 compared with 31.1% treated with placebo (p<0.001). In the anti-TNF-IR group, 50.0% of subjects treated with secukinumab 150 mg achieved an ASAS20 response compared with 24.1% treated with placebo (p<0.05). Numerically greater improvements were observed with secukinumab than with placebo for most secondary endpoints. Clinical responses were sustained through week 52.
Conclusions Secukinumab 150 mg provided sustained improvements in signs and symptoms of AS in anti-TNF-naive and anti-TNF-IR subjects through 52 weeks of therapy.
Trial registration number NCT01649375.
- Anti-TNF
- Ankylosing Spondylitis
- Treatment
Statistics from Altmetric.com
Introduction
Ankylosing spondylitis (AS) is a chronic inflammatory disease which primarily affects the axial skeleton.1 It is characterised by the erosion and fusion of the spinal vertebrae and sacroiliac joints,2 which often results in progressive, irreversible structural damage, deterioration of function, disability and reduced quality of life (QoL).3 ,4
Current therapeutic options are limited for patients with AS. Non-steroidal anti-inflammatory drugs are often insufficient to control disease symptoms and, although anti-tumour necrosis factor (TNF) therapy is recommended for patients with persistent disease activity despite conventional treatment, up to 40% of patients with AS become intolerant to these agents or fail to achieve adequate disease control.5 ,6
Treatment with secukinumab (human anti-interleukin (IL)-17A IgG1k monoclonal antibody) significantly improved the signs and symptoms of AS when compared with placebo treatment in two phase 3 trials (MEASURE 1 (intravenous followed by subcutaneous (s.c.) administration; NCT01358175) and MEASURE 2 (s.c. administration; NCT01649375)).7 In MEASURE 2, 61% and 41% of subjects treated with secukinumab 150 mg and 75 mg, respectively, achieved an Assessment of SpondyloArthritis International Society 20 (ASAS20) response at week 16, compared with 28% given placebo.7 All pre-defined secondary endpoints except ASAS partial remission were met with secukinumab 150 mg s.c. The clinical responses observed at week 16 were sustained through 52 weeks of therapy.7 Responses with secukinumab 75 mg were not significantly different from placebo for the primary endpoint or for secondary endpoints based on hierarchical testing.7 The safety profile was consistent with other studies of secukinumab in AS, psoriatic arthritis and moderate-to-severe plaque psoriasis.7–11
Here, we present the results of a pre-specified subgroup analysis of MEASURE 2 to investigate the efficacy of secukinumab in subjects who were naive to anti-TNF therapy (anti-TNF-naive) and in those with a history of inadequate response or reported intolerance to anti-TNF therapy (anti-TNF-IR).
Patients and methods
MEASURE 2 is an ongoing randomised, double-blind, placebo-controlled, 5-year, phase 3 trial. A complete description of enrolment criteria, study procedures and study design has been reported previously.7
Eligible subjects were aged ≥18 years with AS fulfilling the modified New York criteria, a score of ≥4 (0–10) on the Bath AS Disease Activity Index (BASDAI), and a spinal pain score of ≥40 mm on a 100 mm visual analogue scale, despite treatment with their maximum tolerated dose of non-steroidal anti-inflammatory drugs (NSAIDs). Written informed consent was obtained from all subjects.
Subjects previously treated with only one anti-TNF agent were eligible to participate in the study if they had had an inadequate response after receiving the approved dose for ≥3 months or were unable to tolerate at least one dose (anti-TNF-IR). The online Supplementary Methods file provides further information regarding allowed medication and exclusion criteria.
Supplementary methods
Subjects with active AS were randomised 1:1:1 to secukinumab 150 mg, secukinumab 75 mg or placebo, administered at baseline, weeks 1, 2, 3 and 4, and every 4 weeks thereafter. Randomisation was stratified by anti-TNF history: anti-TNF-naive, or inadequate response or intolerance to one previous anti-TNF agent (anti-TNF-IR).
The primary efficacy endpoint was the proportion of subjects achieving an ASAS20 response (improvement of ≥20% and ≥1 unit on a 10-unit scale in at least three of the four core ASAS domains, with no worsening of ≥20% and ≥1 unit in the fourth) at week 16. Secondary endpoints at week 16 are described in the online Supplementary Methods file. Exploratory endpoints included efficacy assessments through week 52.
Primary and secondary efficacy endpoint analyses included all subjects according to treatment assigned at randomisation. Efficacy analyses in anti-TNF-naive and anti-TNF-IR subgroups were pre-specified.
Logistic regression with treatment regimen and anti-TNF status as factors, and weight as a covariate, was used to evaluate the effect of secukinumab versus placebo for binary variables. Missing response values, including those due to discontinuation, were imputed as non-response (non-responder imputation (NRI)). A mixed-effects model (MMRM) was used to analyse continuous variables. Data are presented by NRI/MMRM and observed analyses at week 52. Further information is provided in the online Supplementary Methods file.
Results
Subjects (N=219) were randomly assigned to treatment with s.c. secukinumab 150 mg (n=72), secukinumab 75 mg (n=73) or placebo (n=74) from 28 October 2012 through 29 July 2013. Of 219 randomised subjects, 61.2% were anti-TNF-naive and 38.8% were anti-TNF-IR. Demographic and baseline characteristics were similar across the subgroups (table 1) with fewer female patients in the anti-TNF-naive placebo group than in the respective secukinumab groups. Characteristics were comparable to the overall study population.7 At week 16, 200 (91.3%) subjects remained in the study and 181 (82.6%) subjects completed 52 weeks of treatment.
Demographic and baseline characteristics
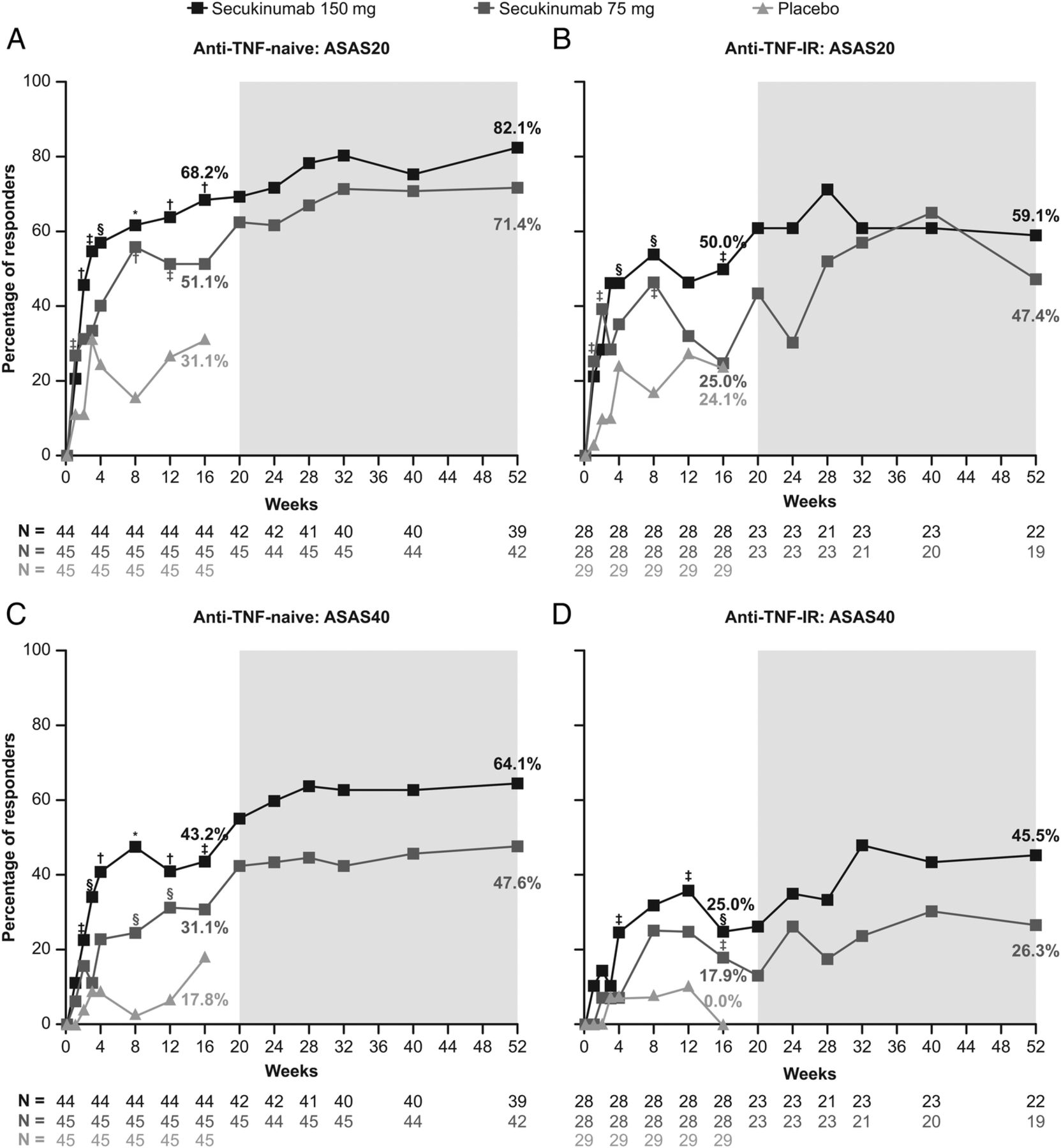
At week 16, a higher proportion of subjects treated with secukinumab 150 mg achieved ASAS20 responses in both anti-TNF-naive and anti-TNF-IR subgroups than in the placebo group (table 2 and figure 1). In the anti-TNF-naive group, 68.2% of subjects treated with secukinumab 150 mg achieved ASAS20 responses (p<0.001 vs placebo), compared with 51.1% of subjects treated with secukinumab 75 mg (p>0.05 vs placebo) and 31.1% of subjects treated with placebo. In the anti-TNF-IR group, 50.0% of subjects treated with secukinumab 150 mg achieved ASAS20 responses (p<0.05 vs placebo), compared with 25.0% of subjects treated with secukinumab 75 mg (p>0.05 vs placebo), and 24.1% of subjects treated with placebo.
Measures of disease activity and health-related quality of life (secondary endpoints) at week 16 (NRI and MMRM analysis)

{kind=link}
Assessment of SpondyloArthritis International Society 20 (ASAS20) and ASAS40 response in anti-TNF-naive and anti-TNF-IR subjects (non-responder imputation (NRI) data to week 16; observed data from weeks 20–52). Shown are the proportions of subjects with ASAS20 responses (improvement of ≥20% and absolute improvement of ≥1 unit (on a 10-unit scale) in at least three of the four main Assessment of SpondyloArthritis International Society criteria (ASAS) domains, with no worsening of ≥20% in the remaining domain) and the proportion with ASAS40 responses (improvement of ≥40% and absolute improvement of ≥2 units (on a 10-unit scale) in at least three of the four main ASAS domains, with no worsening in the remaining domain) in MEASURE 2. Randomisation was stratified by prior anti-TNF use: anti-TNF-naive (left panels) or inadequate response/intolerance to one anti-TNF (anti-TNF-IR; right panels). Missing data were imputed as non-response (NRI) up to week 16. Observed data are presented from week 20 to week 52 (indicated by the grey box in each panel). *p<0.0001; †p<0.001; §p<0.01; ‡p<0.05 vs placebo. TNF, tumour necrosis factor.
At week 16, secukinumab 150 mg also achieved greater improvements versus placebo for ASAS40, ASAS 5/6, high-sensitivity C-reactive protein and the Short Form-36 Physical Component Summary (SF-36 PCS) in both anti-TNF-naive and anti-TNF-IR subjects and for the Ankylosing Spondylitis Quality of Life questionnaire (ASQoL) and BASDAI for anti-TNF-naive subjects (p<0.05 for all comparisons vs placebo) (table 2 and figure 1). There were also numerical improvements in ASAS partial remission with secukinumab 150 mg, which did not reach statistical significance versus placebo. Responses were generally greater in anti-TNF-naive than in anti-TNF-IR subjects.
Improvements in ASAS20 response rates observed at week 16 with secukinumab 150 mg were sustained or continued to improve through week 52 in both anti-TNF-naive and anti-TNF-IR subjects (see figure 1 and online supplementary table S1 (observed data at week 52)). Using a conservative estimate of efficacy at week 52, with missing values imputed as non-response (see online supplementary table S2), the proportions of subjects with an ASAS20 response at week 52 in the anti-TNF-naive group were 72.7% (150 mg) and 66.7% (75 mg). In the anti-TNF-IR group, ASAS20 response rates were 46.4% (150 mg) and 32.1% (75 mg).
Supplementary tables
Improvements in secondary endpoints observed at week 16 were sustained or continued to improve through week 52 in anti-TNF-naive and anti-TNF-IR subjects (see online supplementary figure S1 and online supplementary tables S1 and S2).
Supplementary figure
Discussion
Previous results from MEASURE 1 and MEASURE 2 have shown that secukinumab 150 mg provides clinically significant and sustained improvements in the signs and symptoms of AS.7 The data from this pre-specified subgroup analysis demonstrated that secukinumab 150 mg was effective for subjects who were naive to anti-TNF treatment as well as those who had failed to achieve adequate disease control with, or who were intolerant to, anti-TNF treatment. The improvements observed with secukinumab were generally higher in the anti-TNF-naive subjects compared with anti-TNF-IR subjects.
Secukinumab 150 mg was associated with a reduction in inflammation and improvements in physical function and health-related QoL in both anti-TNF-naive and anti-TNF-IR subjects. Improvements at week 16 were sustained or continued to improve through week 52 in both anti-TNF subgroups.
Responses with the secukinumab 75 mg dose were consistently lower than those with the 150 mg dose in both anti-TNF-naive and anti-TNF-IR subjects. These data provide confirmation that secukinumab 150 mg is an appropriate dose for subjects with active AS. Secukinumab 150 mg has recently been approved (US and EU) for the treatment of adults with active AS.
Reported ASAS20 response rates for anti-TNF agents in anti-TNF-naive subjects are 58–61%12–15 at weeks 12–24, which, by indirect comparison, is comparable to that observed with secukinumab 150 mg in anti-TNF-naive subjects in this study (68.2%).
There are several anti-TNF therapies available for the treatment of AS; however, up to 40% of patients are unresponsive (primary or secondary treatment failure) or intolerant to these agents.5 ,6 According to recent results from the Danish DANBIO registry, ASAS20 response rates for anti-TNF-IR patients are typically lower than those for anti-TNF-naive patients16–19 as observed in this study. The data from MEASURE 2 suggest that IL-17A inhibition may also be an effective therapeutic strategy for patients with an inadequate response/intolerance to TNF antagonists.
A limitation of this study is that it was not designed to show statistical superiority versus placebo by anti-TNF status. It also did not investigate the efficacy of secukinumab in subjects who were unresponsive or intolerant to multiple anti-TNF agents. In addition, the anti-TNF-IR group was not large enough to allow conclusions to be drawn regarding comparative efficacy when further subdivided into primary versus secondary treatment failure or intolerance categories.
In conclusion, secukinumab 150 mg s.c. provided clinically significant and sustained improvements in the signs and symptoms of AS in both anti-TNF-naive and anti-TNF-IR subjects through 52 weeks of therapy.
Acknowledgments
The authors would like to thank the subjects who participated in the study, the study investigators, and John Gallagher, medical communications consultant for Novartis Pharma AG. The initial draft of the manuscript was written by Ellie Ling, the funding for which was provided by Novartis.
References
Supplementary materials
Lay summary
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Tore K Kvien
Contributors BP, MA and HBR were involved in the conception and design of the study, and/or analysis and interpretation of data, and drafting of the manuscript and revising it critically for important intellectual content. JS, AD, HM-O, JAA, RB and TJ-C were involved in the acquisition of data, and drafting of the manuscript and revising it critically for important intellectual content. All authors read and approved the final manuscript.
Funding This clinical trial was sponsored by Novartis Pharma AG. Editorial support was funded by Novartis.
Competing interests JS has received honoraria for consultancy or for being a member of speakers' bureaux from the following companies: Abbvie, Janssen, Lilly, Merck (MSD), Novartis, Pfizer and UCB. AD has received research grants, consulting fees and/or speaking fees (less than $10 000 each) from AbbVie, Amgen, Janssen and Pfizer, and (more than $10 000 each) from Novartis and UCB. HM-O has received speaker fees from Novartis. JAA has received research grants from Ardea, Astra Zeneca, Bristol-Myers Squibb, Celgene, Centocor, Galapagos, Genentech, GlaxoSmithKline, Human Genome Sciences, Janssen, Eli Lilly, Merck, Mesoblast, Novartis, Novo Nordisk, Pfizer, Roche, UCB Biosciences, Sanofi-Aventis, Takeda and Vertex, and has served on the speakers’ bureau for AbbVie, Celgene and UCB. RB and TJ-C report no conflict of interest. MA and HBR report employment and stock ownership from Novartis Pharmaceuticals. BP reports employment and stock ownership from Novartis Pharmaceuticals, and a patent pending on secukinumab for the treatment of non-radiographic axial spondyloarthritis.
Patient consent Obtained.
Ethics approval The institutional review board at each participating centre.
Provenance and peer review Not commissioned; externally peer reviewed.