Article Text

Abstract
Objective Anti-citrullinated protein antibodies (ACPA) are highly specific for rheumatoid arthritis (RA), but the diagnostic accuracy of ACPA in the general population has not been thoroughly assessed. We aimed to assess the diagnostic accuracy of ACPA for RA in the general population and to further characterise the citrullinated peptide recognition pattern.
Methods Serum samples from a large population-representative twin cohort consisting of 12 590 individuals were analysed for the presence of ACPA using anti-CCP2 ELISA. All ACPA-positive samples were further tested on ELISAs for four peptide-specific ACPA. RA cases were identified by linkage to the Swedish National Patient Register at inclusion and after a median follow-up of 37 months (IQR 31–49).
Results 350 out of 12 590 individuals had a positive anti-CCP2 test, measuring ACPA. Of these, 103 had an RA diagnosis at the time of blood donation and inclusion. During a median follow-up of 3 years, an additional 21 of the remaining 247 ACPA-positive individuals developed RA. Overall, a positive anti-CCP2 test had a positive predictive value of 29% for prevalent RA at inclusion (negative predictive value of 99.6%). High titres (>3× cut-off) of anti-CCP2 increased the positive predictive value to 48% (negative predictive value of 99.5%). ACPA-positive individuals without RA had lower anti-CCP2 titres and fewer peptide-specific ACPA than ACPA-positive patients with RA and higher C reactive protein levels than ACPA-negative individuals without RA.
Conclusion Presence of ACPA and especially high titres of anti-CCP2 have a high diagnostic accuracy for an RA diagnosis in a population setting.
- Rheumatoid Arthritis
- Autoantibodies
- Ant-CCP
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) is a complex autoimmune disease progressing throughout distinct preclinical phases, ranging from presence of genetic and environmental risk factors and/or asymptomatic systemic autoimmunity to unclassified symptoms and/or arthritis.1 During these phases, presence of asymptomatic systemic autoimmunity in the form of anti-citrullinated protein antibodies (ACPA) has been suggested to be the most specific diagnostic biomarker for RA, or risk of RA development.2 ,3
To date, most studies of ACPA have typically been performed in selected patient cohorts pertaining to specific preclinical RA phases, such as in cohorts of patients with arthralgia,4 cohorts of patients with RA where serum samples antedating the RA diagnosis are available2 ,5–11 and cohorts of patients with early RA.12 These studies demonstrate that ACPA appear up to several years before disease onset and predict RA development. Further, diversification with recognition of an increasing number of citrullinated peptides and concomitant rise in ACPA titres occur before disease onset,5 ,10 ,11 to reach a fairly stable repertoire once the RA classification criteria are fulfilled.13 ,14 A few small studies have been performed on individuals without signs and/or symptoms of the disease but at an elevated risk of developing arthritis (eg, symptom-free first-degree relatives of patients with RA), indicating lower titres and fewer ACPA reactivities as compared with their RA probands, but higher concentrations compared with population controls.8 ,15–18
In contrast to the wealth of studies of ACPA in such selected patient cohorts, there is a scarcity of studies investigating ACPA in a population setting, where one might expect to find all phases and combinations of phases represented, from being an individual having or not having any risk of developing RA up to actually having RA. We have previously reported on the presence and distribution of ACPA in a large unselected population-based twin cohort showing strong correlation with environmental factors. Taking advantage of this large population-derived cohort, that is followed prospectively, we investigated the discriminatory capacity of ACPA on diagnosing RA and further characterised the citrullinated peptide recognition pattern using follow-up information not previous reported.
Methods
Study subjects
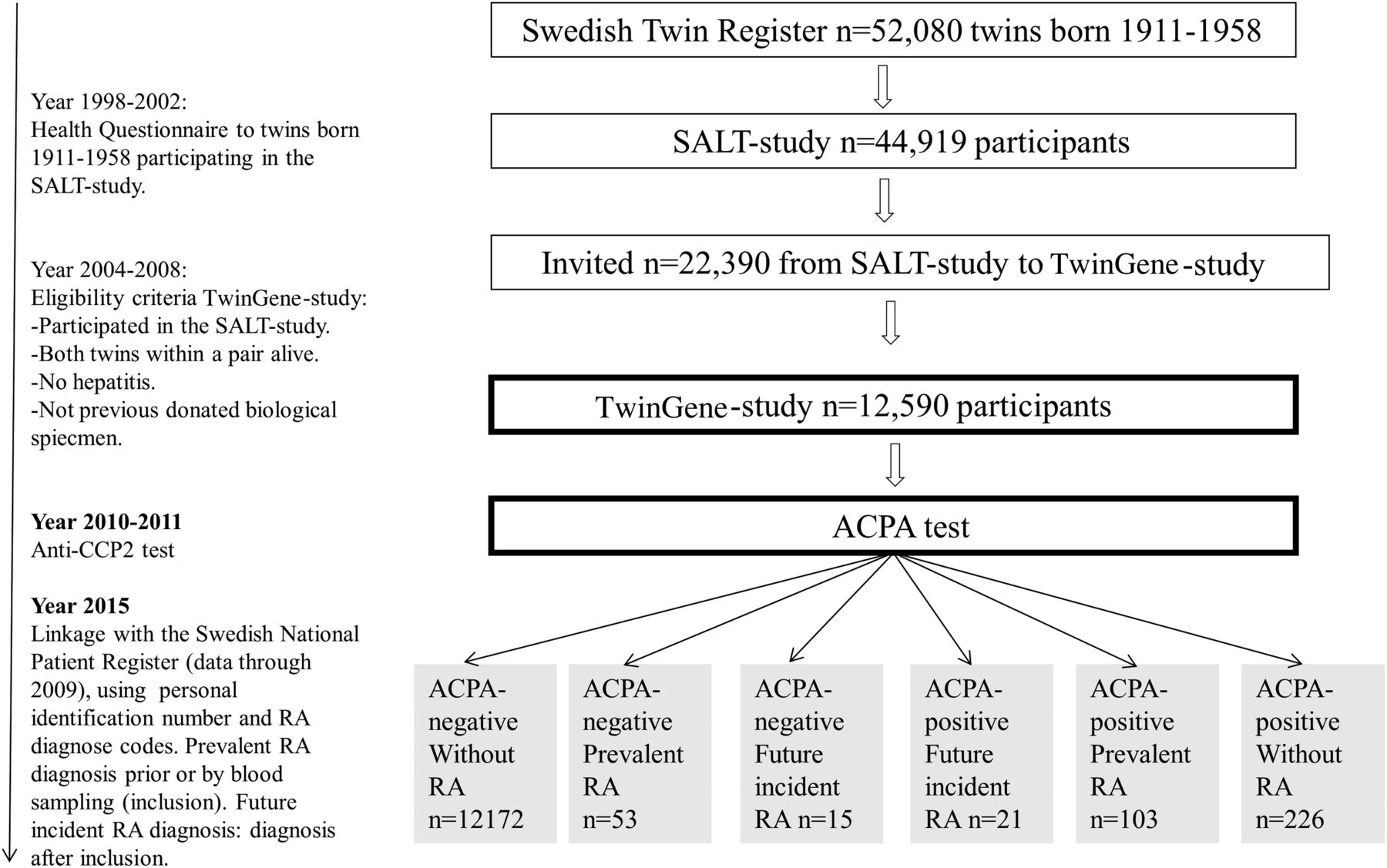
A total of 12 590 twins participating in the Swedish TwinGene study 2004–2008 were included in this study. Eligible twins were born 1958 or earlier in Sweden and part of the national Swedish Twin Registry. Recruitment was thus based on twinship and Swedish residency, but was not dependent on any symptoms or signs of arthritis or of previous testing for ACPA. For details on subject recruitment, see Refs 19–23 The inclusion of individuals started with the oldest age-groups. Detailed demographic characterisation of the tested individuals is presented in table 1 and an overview of participant recruitment and data collection is presented in figure 1. The occurrence of human leucocyte antigen shared epitope alleles (HLA-SE) and smoking among participating twins is similar to previously reported prevalence in the Swedish population.24 ,25
Participants in the TwinGene-study with and without rheumatoid arthritis (RA)

Overview of study recruitment and data collection. ACPA, Anti-citrullinated protein antibody; RA, rheumatoid arthritis.
ACPA testing
All 12 590 serum samples were analysed in 2010 for the presence of ACPA, using an anti-CCP2 ELISA (Immunoscan CCPlus, Malmö, Sweden, Euro Diagnostica),26 ,27 as previously described,19 and supervised by a senior laboratory manager. Samples were defined as being ACPA-positive if anti-CCP2 levels were ≥25 AU/mL as recommended by the manufacturer. High titre was defined in accordance to European League against Rheumatism/American College of Rheumatology 2010 RA classification criteria as three times higher than the cut-off value.28
All ACPA-positive serum samples (n=350) were tested for ACPA reactivities, that is, the presence of antibodies against citrullinated (cit-) and native forms of α-enolase peptide 1 (CEP-1, aa 5–21 with citrulline at positions 9 and 15), vimentin peptide (aa 60–75 with citrulline at positions 64, 69 and 71), fibrinogen α-chain peptide (aa 563–583 with citrulline at position 573) and/or triple-helical peptides of the C1 epitope of type II collagen (cit-C1, aa 359–369 with citrulline at positions 360 and 365),29–32 using peptide-coated ELISA as previously described.19 The cut-off was set using the arbitrary unit (AU) value at 98 percentile in control sera from 152 healthy donors.19 Data about RA diagnosis were not available at the time point for ACPA testing.
C reactive protein (CRP) levels and information on the presence of HLA-SE (DRB1) were available for 11 989 and 10 802 individuals, respectively.19 ,21 CRP levels were analysed by a near-infrared particle immunoassay rate method (measurement interval 0.2–380 mg/L) using Beckman reagents on Synchron LX20 automated equipment (Beckman Coulter, Fullerton, California, USA) and performed by the Karolinska University Hospital Laboratory.33 HLA-SE (classified as HLA DRB1 0101, 0102, 0401, 0404, 0405, 0408 or 1001 alleles) was imputed using genotypes derived from the OmniExpress bead chip (SNP&SEQ Technology Platform, Uppsala).19 ,34 Previous validation comparing imputed data with high-resolution and low-resolution genotyping have revealed a detection accuracy of 84%–96%.35
RA diagnosis
We linked the TwinGene database with the Swedish National Patient Register from the National Board of Health and Welfare (data through 2009) using the personal identification number as linkage key. The index test results were not available to the assessors of the reference standard. The Swedish National Patient Register covers all healthcare and contains information about diagnosis at hospital discharges since 1964 and visits at outpatient non-primary care specialist clinics since 2001. An individual was considered to have RA if an International Classification of Diseases (ICD) code corresponding to RA (ICD7: 722,00 (arthritis rheumatoides); ICD8: 712,38 (arthritis rheumatoides alia definite), 712,39 (arthritis rheumatoides NUD); ICD9: 714A (RA), 714B (Felty’s syndrome), 714C (other RA with visceral or systemic involvement), 714W (other specified RA); ICD10: M05 (seropositive RA), M060 (seronegative RA), M068 (other specified RA), M069 (RA, unspecified)) was identified. Validation using RA classification criteria36 and information from underlying medical files suggest a positive predictive value (PPV) of RA using these algorithms of around 90%.37 ,38 Individuals listed with RA at least once prior to or by the time point for blood donation were considered to have prevalent RA. Individuals first listed with a RA diagnosis between the time of study inclusion and register linkage were considered to have future incident RA. Individuals in the TwinGene cohort who tested positive for anti-CCP2 but had not received a RA diagnosis by the time of register linkage were considered to have ACPA without RA.
Statistical analysis and reporting
Sensitivity, specificity, PPV and negative predictive value (NPV) and positive likelihood ratio (PLR) and negative likelihood ratio (NLR) for prevalent RA at inclusion were estimated by 2×2 tables. Relative risks (RRs) of anti-CCP2-positive individuals having prevalent RA at inclusion were estimated by log binomial regression, adjusting for sex and with a general estimation equation (GEE) analysis. GEE estimates SE by using a sandwich covariance estimator that corrects for the correlated data structure. Differences between anti-CCP2 titres and CRP concentrations were analysed with the Wilcoxon rank-sum test. Correlation between anti-CCP2 titres and the number of ACPA reactivities was analysed by the Spearman's rank test. p Values <0.05 were considered significant. Statistical analyses were performed with SAS software (V.9.3). We used the STARD checklist for accurate reporting of diagnostic accuracy.39 The Ethical Review Board at Karolinska Institutet approved the study.
Results
Identification of prevalent, future incident RA and ACPA-positive RA
Among the 12 590 individuals included (median age 64 (first to third quartiles: 60–70), 55% women), 156 (1.2%) had received a diagnosis of RA at the time of inclusion and were hence referred to as prevalent RA cases (table 1). The first registered prevalent RA diagnosis was set at a median of 64 months (first to third quartiles: 39–205) prior inclusion.
During a median follow-up period of 37 months (first to third quartiles: 31–49) after inclusion, an additional number of 36 individuals (0.3%) received a first-ever RA diagnosis (in median 21 month after inclusion (1st–3rd quartile: 8–27)) and were hence categorised as future incident RA. Incidence rate was estimated to be 88 per 100 000 person-years.
Among the 12 590 individuals, 350 (2.8%) were positive for ACPA (measured with the anti-CCP2 test). Based on the anti-CCP2 test and using the same RA diagnosis algorithm as described above, 103 individuals (0.8%) were identified with ACPA-positive prevalent RA and 21 individuals (0.2%) were identified with ACPA-positive future incident RA, while 226 (1.8%) were identified as ACPA-positive individuals without RA during follow-up from inclusion into the study.
ACPA and CRP in relation to RA diagnosis
Anti-CCP2 titres in ACPA-positive individuals without RA were lower (median 51 AU/mL (first to third quartiles: 34–149) than those of individuals who later developed incident ACPA-positive RA (median 193 AU/ml (first to third quartiles: 149–781)) and compared with those who had prevalent ACPA-positive RA (median 508 (first to third quartiles: 194–1060)), (p<0.0001) (figure 2A).

Anti-citrullinated protein antibodies (ACPA), ACPA reactivities, C reactive protein (CRP) and rheumatoid arthritis (RA) in a population-derived cohort are shown. (A) Detected ACPA (anti-CCP2) concentration among ACPA-positive individuals without RA, with future incident RA or with prevalent RA is shown. Box illustrates median and first to third quartiles. Whiskers represent minimum and maximum. The Y axis is cut with two dashed lines, at cut-off: 25 AU/mL and at high concentration of 75 AU/mL. (B) CRP concentration among individuals without RA, with future incident RA or with prevalent RA stratified by anti-CCP2-titre-negative (<25 AU/mL), low anti-CCP2 titre -positive (25–75 AU/mL) and high anti-CCP2 titre-positive (>75 AU/mL) status is shown. Box illustrates median and first to third quartiles. *p Value <0.05; # denotes significant differences, p value <0.05, as compared with ACPA-negative no incident/prevalent RA. Whiskers represent minimum and maximum. (C) Prevalence of ACPA reactivities among ACPA (anti-CCP2)-positive individuals without RA, with future incident RA or with prevalent RA is shown. Data about anti-cit enolase/anti-cit fibrinogen/anti-cit-C1 were missing in 4/11/20 individuals and patients. (D) Plotted association between anti-CCP2 concentration and number of ACPA reactivities among ACPA (anti-CCP2)-positive individuals without RA is shown. AU, arbitrary unit.
Significant differences in the median CRP levels were observed between ACPA-negative individuals (median 1.7; first to third quartiles: 0.7–3.4) and all ACPA-positive individuals (median 2.8; first to third quartiles: 1.2–6.4; p<0.0001) (data not shown). Median CRP levels in ACPA-negative individuals were significantly lower compared with individuals with high anti-CCP2 titres (with or without prevalent RA) (median 4.0; first to third quartiles: 1.6–10.2; p<0.0001) and with individuals with ACPA-negative future incident and prevalent RA (median 3.7; first to third quartiles: 1.4–7.6; p<0.0001) (figure 2B). We also observed differences in the prevalence of ACPA reactivities, such that fewer ACPA-positive individuals without RA (compared with those with RA) tested positive for different ACPA reactivities (figure 2C). Among ACPA-positive individuals without RA, 26% (59/223) tested positive for anti-cit-enolase, 12% (27/226) for anti-cit-vimentin, 8% (18/218) for anti-cit-fibrinogen and 15% (31/209) for anti-cit-C1. Among individuals who later developed incident ACPA-positive RA during follow-up, 52% (11/21) tested positive for anti-cit-enolase, 52% (11/21) for anti-cit-vimentin, 29% (6/21) for anti-cit-fibrinogen and 20% (4/20) for anti-cit-C1. Among individuals with prevalent ACPA-positive RA, 76% (78/102) tested positive for anti-cit-enolase, 49% (50/103) for anti-cit-vimentin, 30% (30/100) for anti-cit-fibrinogen and 35% (35/101) for anti-cit-C1.
Anti-CCP2 titres further correlated with the number of detectable ACPA reactivities in ACPA-positive individuals without RA (r 0.63 (95% CI 0.54 to 0.70) p<0.0001, figure 2D), those later developing incident RA (r 0.79 (95% CI 0.55 to 0.91) p<0.0001) and those having prevalent RA (r 0.66 (95% CI 0.53 to 0.76) p<0.0001). A large majority of the ACPA-positive individuals without RA (148/226, 65%) and a minority of those who were ACPA-positive later developing incident RA (7/21, 33%) and those who had prevalent ACPA-positive RA (17/103, 17%) were negative for all tested specificities. When analysing prevalent combinations of different ACPA reactivities, no specific pattern was identified in the ACPA-positive individuals with or without future incident /prevalent RA (figure 3).

{kind=link}
{kind=link}
{kind=link}
Citrullinated peptide recognition pattern among anti-citrullinated protein antibodies (ACPA) (anti-CCP2)-positive individuals in a population-derived cohort is shown. Pie charts illustrate pattern of occurring ACPA reactivities in ACPA (anti-CCP2)-positive individuals without rheumatoid arthritis (RA), with future incident RA or with prevalent RA. cit-eno/ cit-vim/ cit-fib/cit-col denotes anti-cit enolase/vimentin/fibrinogen, respectively, C1 epitope of type II collagen; + denotes positive status.
Diagnostic accuracy of the ACPA test for prevalent RA
Based on the distribution of ACPA positivity among the 156 cases of prevalent RA at inclusion, the sensitivity and specificity of the anti-CCP2 test for RA was 66% and 98%, respectively. Using the high anti-CCP2 cut-off resulted in a sensitivity of 62% and a specificity of 99% (table 2).
Diagnostic accuracy of ACPA for prevalent rheumatoid arthritis (RA) at inclusion
The PPV for anti-CCP2 with regard to prevalent RA was 29% (95% CI 25 to 34) and 48% (95% CI 41 to 55) for the high anti-CCP2 cut-off. The NPVs were similar for anti-CCP2 test and high anti-CCP2 cut-off (99.6% and 99.5%). We further estimated the RR for having prevalent RA if the anti-CCP2 test were positive (table 3). Similar results were obtained with a binomial regression and a GEE model which take into account the twin dependency of the observations. The RR for RA was 64 (95% CI 46 to 88) if anti-CCP2 test was positive and 94 (95% CI 70 to 127) if high anti-CCP2 cut-off was positive (p value<0.0001 for both RR).
Relative risk (RR) for rheumatoid arthritis (RA) diagnosis associated with anti-citrullinated protein antibody positivity
Discussion
ACPA positivity has been shown to have a high specificity for RA in previous smaller studies8 ,40 ,41 and in a recent systematic review,42 but no such estimation is currently published in cohorts reflective of the general population. We took advantage of a unique population-derived twin cohort and were able to demonstrate a high RA diagnosis accuracy for ACPA measured with an anti-CCP2 test with regard to prevalent RA. High anti-CCP2 titres were associated with increased specificity for prevalent RA with only minor decrease in sensitivity and high titres associated with a broader citrullinated peptide recognition pattern and higher levels of CRP.
The RA prevalence in the investigated cohort (1.2%) and incidence rate (88 per 100 000 person-years) was similar to the expected in the general population of the same age,43 ,44 supporting representativeness despite the twin design. One important advantage of the current study is the lack of any other positive or negative selection criteria, such as presence of other diseases or comorbidities. This is in contrast to previous studies reporting on ACPA diagnosis accuracy in either blood donors (where many diseases and infections that theoretically increase the risk of seropositivity are excluded2) or selected populations such as first-degree relatives of probands with RA,16 patients with other autoimmune diseases than RA45 and healthy individuals not having any kind of autoimmune diseases.46 Also, with some 12 590 individuals the current study is so far the largest to report on the diagnostic accuracy of ACPA (the majority of previous published studies included less than 500 healthy controls,6–8 ,45 only one study included 2358 healthy blood donors).2 Our results are in accordance with these previous reports, demonstrating a high specificity of anti-CCP2 test for RA (range between 97% and 99.5%). Further, preliminary data in a population-derived Dutch cohort47 also support our results. In line with most of the previously published studies in prevalent RA, we noted a fair level of sensitivity.42 In contrast, studies performed in pre-RA cohorts tend to result in lower sensitivities, almost half as low as in prevalent RA, probably due to the cumulative appearance of ACPA up to 20 years before disease onset5 and lack of repetitive sampling in some individuals. We also report a higher specificity associated with high titres of ACPA, with increased PPV, and only minor changes in sensitivity and NPV. Furthermore, high anti-CCP2 associates with presence of more specificities and a higher level of CRP. A large majority of the ACPA-positive individuals developing incident RA during the 3 years follow-up had high levels of anti-CCP2 (18/21, 86%). Our findings are in line with previous studies,4 ,10 ,11 showing that increasing numbers of ACPA reactivities increase the risk of imminent RA and further suggest that a high ACPA titre is an equally good predictor as having multiple reactivities. The high ACPA titre and multiple reactivities might reflect a genuine repertoire diversification as previously suggested,4 ,11 ,32 ,48 ,49 but peptide cross-reactivity previously reported in some studies for ACPA50 ,51 could also play a role. We have previously reported that presence of HLA-SE is a risk factor for developing ACPA and having an ACPA-positive RA. Even though interesting, the low number of incident RA (n=36) preclude any other in-depth analysis and conclusion. Previous studies have reported on the frequency of ACPA positivity in the general population, but our present study is the first to report on the specific distribution of antibodies against specific citrullinated peptides in a similar setting19 ,46 with the advantage of a particular large cohort of ACPA-positive individuals without RA. Our finding that only a minority of the ACPA-positive individuals without RA tested positive at inclusion for any ACPA reactivities despite a median age similar to those already having ACPA-positive RA strengthens the importance of longitudinal follow-up to eventually identify those ACPA-positive individuals who might never develop RA.
There are several limitations to our results, some of them inherent to the study design. The age-inclusion criteria in the investigated cohort were chosen specifically to ensure an age-span representative for complex diseases such as RA. While this should have a minimal impact on our findings, our conclusions might not be directly applicable in younger populations. The definition of ACPA is given to those that in fact have antibodies to peptides included in the anti-CCP2 test. These peptides are unknown but earlier tests have shown that they have a very broad coverage and will capture most, but not all of ACPA reactivities produced. This will affect the interpretation of the specificity and sensitivity data of the various known citrullinated peptides used. Some of the individuals classified with only having future incident RA (and especially those identified with incident RA very close after blood donation) might actually already have had RA at the time of blood donation, leading to underestimation of prevalent RA. However, as the prevalence of RA in our cohort is largely similar to that reported by others, we assume only a minor impact of such misclassification. Even though the median age of the cohort corresponds to the age peak of RA incidence,44 it is still possible that more individuals in the ACPA-positive group will, with further follow-up, eventually develop RA. To account for the influence of recruitment timing on the follow-up duration, we compared the follow-up time of those developing RA with those not developing RA in the same age group and found no difference (data not shown). Also the lack of consecutive ACPA testing in same subjects is a limitation preventing estimation of the predictive values of variable ACPA status over time but will be an important task for future studies.
In conclusion, we have demonstrated that ACPA testing in a population-based setting has high specificity for prevalent RA. High anti-CCP titre entails better prediction for RA and is linked to multiple ACPA reactivities and higher CRP levels.
Acknowledgments
The authors would like to thank Professor Lars Klareskog for expert advice and facilitating access to biobank and register data.
References
Footnotes
Handling editor Tore K Kvien
Contributors All authors made substantial contributions to (1) conception and design, or analysis and interpretation of data (2) drafting the article or revising it critically for important intellectual content and (3) gave final approval of the version to be published.
Funding This work was supported by research funding from Innovative Medicine Initiative BTCure (115142-2), FP7-HEALTH-2012-INNOVATION-1 Euro-TEAM (305549-2), the Initial Training Networks seventh framework programme Osteoimmune (289150), the Swedish Research Council and the Swedish Foundation for Strategic Research.
Competing interests RH is a holder of a patent (US Patent 7 148 020) protecting the use of the CitC1 peptide.
Ethics approval The Regional Ethical Review Board, Stockholm.
Provenance and peer review Not commissioned; externally peer reviewed.