Article Text

Abstract
Background We aimed to describe the main features of Behçet's disease (BD) in children in the largest prospective cohort to date and to propose a classification.
Methods An international expert consensus group was formed to define a data set of minimal symptoms for the inclusion of patients. Patients were entered prospectively during 66 months. Experts classified patients on a consensus basis. The concordance of two international classifications was analysed in confirmed patients with BD. Comparisons of subgroups of patients helped define consensus criteria. BD-associated clinical manifestations were also investigated in three control diseases extracted from an independent data set (Eurofever).
Findings In total, 42 centres from 12 countries included 230 patients; data for 219 (M/F ratio=1) could be analysed. The experts classified 156 patients (71.2%) as having confirmed BD. Males more often than females showed cutaneous, ocular and vascular symptoms and females more often genital aphthosis. Age at disease onset and skin and vascular involvement were lower for European than non-European children. Oral aphthosis was the presenting sign for 81% (179/219) of patients. The mean delay to the second symptom was 2.9±2.2 years. International classifications were not concordant with the expert classification. Our paediatric classification contains six categories, a minimum of three signs (each in a distinct category) defining paediatric BD. Three clinical signs discriminated our cohort from the Eurofever cohorts.
Interpretation We present a comprehensive description of a large cohort of patients from both European and non-European countries and propose the first classification of paediatric BD for future therapeutic trials.
- Behcet's disease
- Epidemiology
- Fever Syndromes
Statistics from Altmetric.com
Introduction
Behçet's disease (BD) is a systemic inflammatory condition sharing the clinical features of both autoinflammatory disease and vasculitis.1 ,2 Its pathogenesis is still unclear, but the combination of genetic factors affecting the immune regulation and undetermined environmental triggers may explain the variability disease expression.3 The clinical spectrum of BD comprises a number of organ involvements; the pattern of skin lesions and the peculiar occurrence of thrombosis in all types of vessels represent important clues. In fact, the disease is now classified as a ‘variable vessel vasculitis’, which highlights the involvement of any artery and vein.4 Oral aphthosis is present in almost all patients with BD (98%).5 As well, BD manifestations are recurrent. Some heal without scar or sequelae, but others cause substantial morbidity, such as ophthalmological manifestations, which may cause blindness and vascular and cardiac involvements, the main causes of mortality.6
Although generally recognised in adulthood, the first BD symptoms may start early in life, and the disease is rarely completed before the age of 16 years in 4–26% of cases.7 At this age, the frequency of uveitis is lower than in adults and the rate of familial aggregation is high, which strongly suggests a genetic component.8–11
BD is diagnosed when a patient presents a combination of symptoms among the most frequently observed and/or the most typical of the disease. Several international groups have attempted to propose clinical criteria for classification or diagnostic criteria in adult patients with BD. The most currently used are those developed by an international study in 1990 (see online supplementary table S1).12 The sensitivity of the criteria appeared relatively low because they were not established in accordance with the geographical variations of BD phenotype. Revised criteria were proposed from a multinational collaboration of 27 countries: in addition to mucocutaneous and ocular features, the criteria included neurological and vascular involvement.13 However, we lack a suitable, validated definition of BD in children, and the diagnosis remains challenging. The diagnostic criteria of paediatric BD must be sensitive as well as specific because several other conditions, especially autoinflammatory diseases, inflammatory bowel diseases and immunodeficiency, can mimic BD.
The Paediatric Behçet's Disease (PEDBD) study was established to identify the clinical course of children presenting few symptoms of BD and for whom other diagnoses were ruled out. We wanted also to provide a paediatric BD classification to help in performing future therapeutic trials.
Aims of the PEDBD study
The primary objective was to establish a prospective cohort of paediatric patients presenting a minimal set of BD signs. The secondary objectives were as follows:
to identify a subgroup of patients with confirmed paediatric BD by an adjudication process involving expert consensus;
to define the natural history of BD by type of symptoms and their chronology of appearance;
to test the concordance of two international BD classification criteria with the developed expert classification, then define a paediatric classification;
to perform an external validation of the new paediatric classification by using data from patients with other autoinflammatory diseases as negative controls.
Patients and methods
Study design
First step: establishing an expert consensus group and minimal set of symptoms
The expert committee of four adult specialists and three paediatricians defined the minimal set of symptoms as follows: recurrent oral aphthosis, at least three times a year, associated with at least one of the following: genital ulceration or aphthosis, vessel thrombosis or aneurysm, erythema nodosum, acneiform lesions, papulopustular lesions, skin ulceration or aphthosis, positive pathergy test, uveitis (post or panuveitis), retinal vasculitis and family history of BD (if documented).
Inclusion/exclusion criteria for the PEDBD cohort
Patients needed to fulfil the criteria established by the expert committee and to sign an informed consent for participation according to the regulations of participating countries. They had to present a first symptom before age 16 and have no concomitant diseases interfering with BD evaluation. These were new or already known patients (maximum 3 years) and could be followed prospectively for at least 4 years. Exclusion criteria were patients who did not meet at least one of these criteria.
Second step: establishing an electronic database, international collaboration and data entry
An online database was designed following the national regulations in France and in accordance with local regulations in each participating countries. Inclusion and update visits were recorded into a standardised format. Our clinical research unit (HA, AA, CP) provided data management. The Paediatric Rheumatology European Society, Paediatric Rheumatology INternational Trials Organisation and International BD society members entered their patients anonymously.
Third step: annual review and case adjudication
The expert committee performed an annual chart review. In a round-robin format, the members collected votes to classify patients as having confirmed, probable and uncertain or no BD. Consensus was obtained with 80% agreement. Charts for patients were reviewed more than once, if necessary, until the PEDBD group closed the study, during the last meeting on 6 February 2014. Patients without diagnostic consensus at this deadline were not classified.
Fourth step: statistical analysis
The comparison of confirmed and unconfirmed patients with BD provided a preliminary classification, which was secondarily endorsed by consensus. Patients from the Eurofever registry were negative controls (see online supplementary information 1).4 Variables included in the PEDBD score were anonymously extracted and analysed. Criteria defining BD were based on symptoms appearing before the expert classification, and the analysis of natural history was based on symptoms collected during the whole study. For univariate analyses, continuous variables are summarised with mean (SD) and categorical variables as number (percentage). Missing data were described by calculating the percentage of the total effective data and were excluded from further analyses. For bivariate analyses, the primary outcome was the expert classification (confirmed and unconfirmed BD). Symptoms, determinants of symptoms and potential associated factors were compared. The association of qualitative variables and the primary outcome (confirmed BD) was analysed by Pearson's χ2 or Fisher's exact test and that of quantitative variables and the primary outcome was by Student's t or Mann–Whitney U test. For multivariate analysis, a logistic regression model with stepwise selection was used to investigate the association of symptoms and confirmed BD, reporting ORs and 95% CIs. Significance at p≤0.20 was required to be included and remain in the model. Potential interactions between variables were tested. A sensitivity analysis was performed to analyse whether headache should be included in neurological symptoms. For each subject, the number of criteria was calculated from symptoms retained in the model plus oral aphthosis. The optimal number of criteria distinguishing confirmed and unconfirmed BD was established by receiver operating characteristic (ROC) curve analysis. To assess sensitivity and specificity, the agreement between the BD classification and alternative classifications was analysed by the Kappa method.12 ,13 Symptom patterns and pathology type were explored by multiple correspondence analyses. Statistical analyses involved use of SAS V.9.3 (SAS Institute, Cary, North Carolina, USA).
Results
The total duration of the PEDBD study from the first to the last inclusion was 66 months.
Fulfilment of inclusion and non-inclusion criteria, and minor protocol deviations
In total, 227 patients were eligible and agreed to be included in the study; 53 (23.3%) were ≥16 years old at the inclusion visit. Overall, 220 had at least one symptom in addition to recurrent oral aphthosis; 7/227 (3.1%) had oral aphthosis associated with a family history of BD, and 8/227 (3.5%) who presented or showed another disease during the PEDBD study were excluded. Finally, data for 219 patients could be analysed during 717 follow-up visits (mean 3.2 visits per patient) (see online supplementary figure S1).
Epidemiological data and whole cohort
The 219 patients (109 males) originated from 42 centres in 12 countries (not shown). The ethnic distribution was approximately one-third European Caucasian, one-third Middle Eastern Caucasian and one-third North African (not shown). The mean age at first symptom was 7.4±4.2 years (median 7 years, range 0–15.9 years). In addition to recurrent oral aphthosis, patients had genital aphthosis 104/219 (47.5%), necrotic folliculitis, pustular or acneiform lesions 60/198 (30.3%), erythema nodosum 37/198 (18.7%), pathergy 42/94 (44.7%), anterior uveitis 52/219 (23.7%), posterior uveitis 47/219 (21.5%), retinal vasculitis 20/219 (9.1%), papilledema 17/219 (7.8%), anterior uveitis in association with at least another posterior finding 29/52 (18.6%), venous thrombosis 21/219 (9.6%), and arterial thrombosis or aneurysm 4/219 (1.8%).
Classification of PEDBD patients and comparison of confirmed and unconfirmed BD
The expert committee classified 156/219 patients (71.23%) as having confirmed BD and 63 as having unconfirmed BD (probable 26, uncertain 14, no consensus 18, not BD 5). Patients with confirmed and unconfirmed BD were comparable in sex ratio (M/F=1), family history of BD, consanguinity and disease duration since the first symptom to the first and last visit (table 1). However, age at first symptom, at first suspicion and at BD confirmation was higher for confirmed than unconfirmed patients. BD confirmation was associated with clinical symptoms of genital aphthosis (p=0.0004) and any of the following: cutaneous (pathergy test excluded from the analysis; p=0.0084), neurological (p=0.0022), ocular (p=0.0002) and vascular symptoms (p=0.0052) (see online supplementary table S2). It was associated with the cutaneous symptoms necrotic folliculitis/acneiform lesions/folliculitis (p=0.0169) and erythema nodosum (p=0.0279), as well as anterior and posterior uveitis (p=0.0150 and 0.0029), retinal vasculitis (p=0.0010) and papilledema (p=0.0022) but not presence of human leucocyte antigen B51 (p=0.2965) (not shown).
Epidemiological characteristics of the 219 Paediatric Behçet's Disease (PEDBD) patients with confirmed and unconfirmed Behçet's disease (BD)
Descriptive data for the 156 patients with confirmed BD
Of the 156 patients with confirmed BD, half were males (n=78) (table 1); about half (56.41%, n=88) lived in Europe (not shown). Among them, 86 (53.8%) were <16 years at BD confirmation. The main categories of clinical symptoms at BD confirmation are given in online supplementary table S2. More detailed clinical information is available in the online supplementary file additional information no 3.
Gender differences
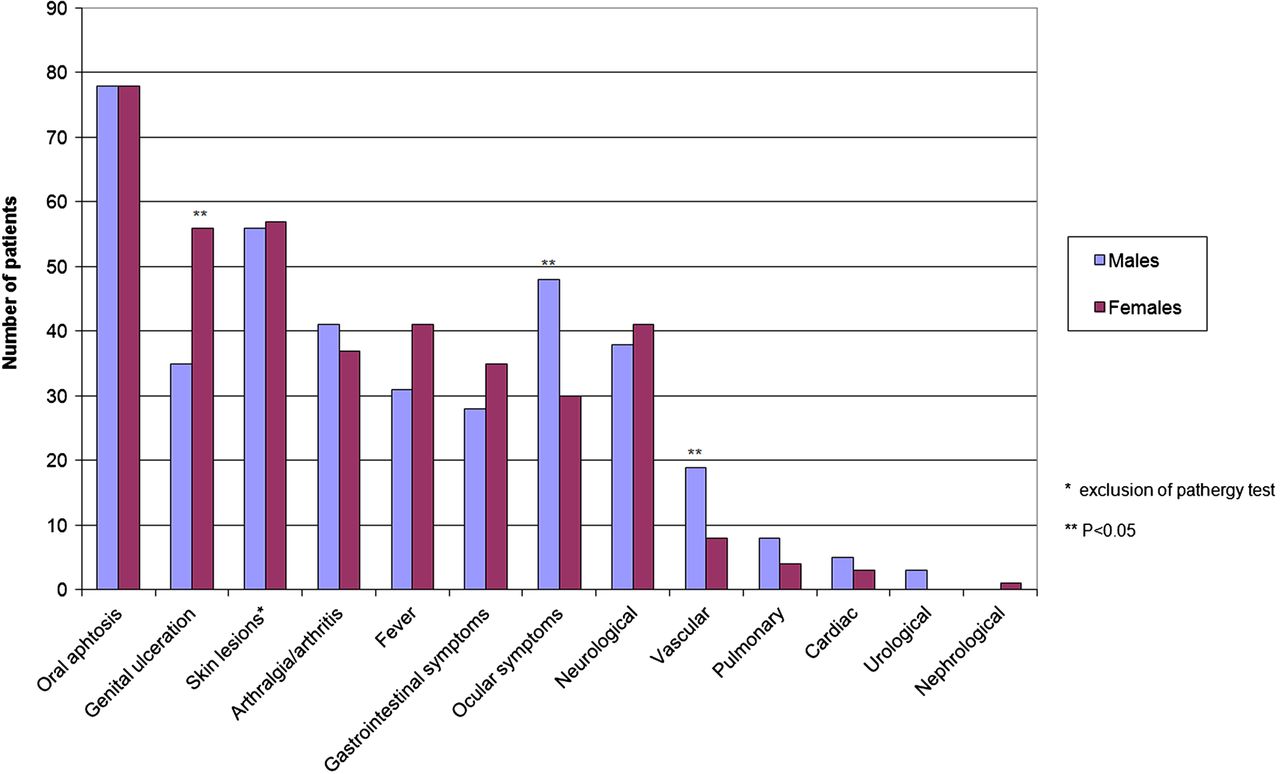
The mean number of attacks per year of oral aphthosis was similar for females and males with confirmed BD (11.32±10.87 and 13.16±14.23), as was the mean number of attacks of genital ulceration (3.42±4.46 and 3.85±4.40) (not shown). However, the sexes differed in distribution of clinical symptoms (figure 1). Indeed, genital ulceration was associated more with females than males (p=0.0006), and ocular symptoms as a whole and vascular symptoms were associated more with males (p=0.0039 and 0.0199). Considered individually, none of the cutaneous symptoms differed between the sexes. Among the ocular symptoms, males more than females showed posterior uveitis (p=0.0004), retinal vasculitis (p=0.0265) and papilledema (p=0.0348), as well as involvement of both eyes (p=0.0193), visual acuity <1/10 (p=0.5766) and venous thrombosis (p=0.0265). Cranial nerve palsy was more common, although not significantly, in females than males (p=0.1165).
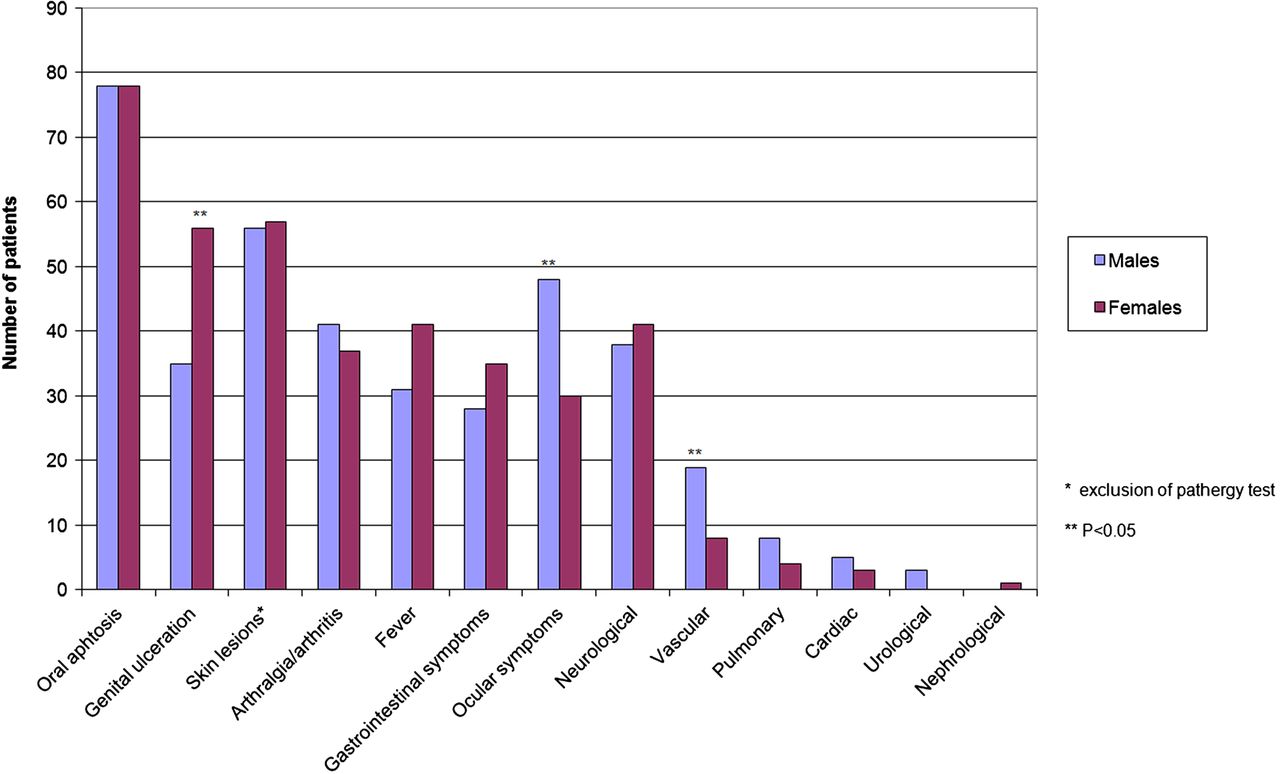
Frequency of symptoms in 156 patients with confirmed Behçet's disease according to the gender.
Regional differences
The age at first BD symptom was significantly lower for patients in European than non-European countries (6.84±4.66 vs 9.12±3.67; p=0.0017). European patients frequently showed articular (p=0.0527) (especially axial joints; p=0.0061 vs peripheral; p=0.0892), gastrointestinal (p<0.0001) and neurological symptoms (including headaches: p<0.0001; without headaches but with papilledema: p=0.05), and fever (p<0.0001). Conversely, some symptoms more frequent for non-European patients included necrotic folliculitis, pseudo folliculitis and acneiform lesions (each p<0.05). European and non-European patients did not differ in individual ocular symptoms, but European patients more frequently showed bilateral symptoms (p=0.0405) that resulted in visual loss (visual acuity <1/10; p=0.0447). Among neurological symptoms without headaches, only long-tract dysfunction was more frequent, although not significant, in European than non-European patients (p=0.0687). Vascular symptoms were more frequent in non-European patients.
Chronology of symptoms and pathways of entry in BD through the PEDBD cohort study
Oral aphthosis was the presenting symptom for 81% (179/219) of patients, followed by genital ulceration, skin symptoms and fever (20.5%). The chronology of symptoms in patients with and without confirmed BD is shown in figure 2 and online supplementary figure 2. The ages of onset of symptoms by classification are given in table 2. The mean ages at onset of oral aphthosis (8.74±4.21) and neurological symptoms were significantly higher for patients with confirmed than unconfirmed BD (p=0.0143 and 0.0144, respectively). The median delay between the first and second wave of symptoms in all patients was 2 years (range 1–12 years; mean 2.9±2.2 years) (see online supplementary figure 3), and the median delay between the second and third and third and fourth waves was 1.5 years (range 1–8 years, mean 2±1.6). New symptoms occurring during follow-up were more frequent for patients with than without confirmed BD (not shown). The mean delay between the first symptom and age at BD confirmation was 6.0±3.5 years. One patient died of multiple thromboses.
Age of onset of Behçet's disease (BD) symptoms for patients with confirmed and unconfirmed BD by expert classification (Paediatric Behçet's Disease (PEDBD))

{kind=link}
{kind=link}
Chronology of symptoms in 156 patients with confirmed Behçet's disease.
Comparison of expert classification with international criteria for BD
In all, 115/156 PEDBD patients fulfilled the ISG criteria (sensitivity 73.7%, specificity 100%; κ coefficient 0.62). In general, PEDBD patients discordant with the ISG criteria had only one of genital, skin and ocular symptoms. The new international PEDBD classification evaluated without the pathergy test had higher sensitivity (91.7%; 143/156 patients fulfilling both classifications) but lower specificity (42.9%, κ=0.39). The addition of the pathergy test did not improve performance (κ=0.44; sensitivity 96.2%, specificity 41.3%). The discordance was not improved with oral plus genital aphthosis or oral aphthosis plus ocular symptoms (κ=0.49).
Preliminary classification of paediatric BD according to the PEDBD data
Symptoms associated with BD confirmation were considered simultaneously. The categories of signs were genital ulceration and cutaneous, ocular, neurological and vascular symptoms. Several hypotheses were tested for neurological symptoms because only headaches and papilledema appeared significantly associated with confirmed BD. Two of the hypotheses are given in online supplementary table 3. All experts agreed to retain neurological symptoms as a whole; indeed, neurological symptoms were found in only confirmed patients with BD. The mean number of symptoms at the time of the expert classification was significantly higher for patients with confirmed than unconfirmed BD (3.15±0.89 vs 2.08±0.6; p<0.0001) (not shown). The ROC curve for three symptoms gave sensitivity 77% and specificity 88% (not shown). Taking into account both the category of signs and number of signs significantly associated with the experts’ confirmation of BD and the experts’ consensus, we proposed a first classification of BD in children (table 3).
Consensus classification of paediatric Behçet's disease (BD)
Comparisons with the Eurofever cohort
The Eurofever registry provided data for 410 patients (220 males; mean age 7.6±3.8 years, range 6 months to 16 years) with diseases distinct from BD, who were negative controls (ie, periodic fever adenitis pharyngitis and aphthosis (PFAPA) syndromes, n=259; cryopyrin-associated periodic syndrome (CAPS), n=86; and mevalonate kinase deficiency (MKD), n=65). The mean age for our BD-confirmed patients was higher (p<0.0001). Significant differences appeared for all categories and testing different hypotheses for ocular and neurological symptoms (table 4). For the Eurofever patients, the mean number of BD symptoms was lower for confirmed than unconfirmed patients with BD in the PEDBD population (p<0.0001) (eg, PFAPA 0.63±0.52, CAPS 0.52±0.76 and MKD 0.8±0.71 vs 3.15±0.89 and 2.08±0.6, respectively). Multiple correspondence analyses between PEDBD and Eurofever are given in online supplementary figure S4.
Frequency of symptoms among diseases and confirmed and unconfirmed paediatric Behçet's disease (BD)
Discussion
BD in children is rare and challenging to recognise. We aimed to describe the main features of the disease in the largest prospective cohort to date and propose a classification of paediatric BD. Among the 219 children included (equal males and females, symptoms appearing before age 16), the experts confirmed BD in 156 (71.2%). Males more often than females had cutaneous, ocular and vascular symptoms and females more often than males had genital aphthosis. Oral aphthosis was the presenting sign in 81% of patients. International classifications were not concordant with the experts’ classification. Our paediatric classification contains six categories, a minimum of three defining paediatric BD (table 3).
The main strengths of the PEDBD study are the international collaboration and its prospective study design assessing the natural history of BD. In addition, it is the first attempt to emphasise the shortcomings or limitations of the adult criteria for the paediatric population and introducing the main features in paediatric BD in the largest cohort of patients. Oral aphthosis was mandatory for inclusion because of its high frequency in children with BD (95%).9 ,11 ,14–17 Symptoms such as vascular symptoms and family history were included because they represented a considerable share of the features of paediatric patients. To attain our first objective, to establish a prospective cohort of paediatric patients presenting a minimal set of BD signs, a remarkable effort was made during 7 years to update patient information and classify the disease each year, independent of any predefined criteria. Confirmed BD was associated with genital aphthosis, skin manifestations, neurological and vascular symptoms as well as number of attacks of oral aphthosis, visual acuity <1/10 and the presence of a median number of three symptoms. Patients with confirmed BD had an equal sex ratio and most lived outside Europe (56%). Cutaneous signs were the most frequent, and ocular symptoms and genital aphthosis were less frequently observed than in adults. Females more often than males had genital aphthosis, whereas males more often than females had ocular and vascular symptoms.7 ,9 ,18 ,19 Age at onset and articular, gastrointestinal and neurological symptoms during follow-up were more frequent in European than non-European patients, who also had had more skin and vascular involvement, in accordance with several BD cohorts and registries.7 ,9 ,20 ,21 Interestingly, European patients more frequently had bilateral lesions (p=0.0405) and visual loss (p=0.0447). A lower degree of awareness of BD uveitis in European than non-European patients could delay appropriate treatment. The second BD symptom appeared at a median of 2 years (mean 2.9±2.2) and BD confirmation at 6.0±3.5 years.8 Oral ulceration was the first symptom in most cases and was generally followed by cutaneous signs, fever, articular or gastrointestinal signs. Ocular and vascular symptoms appeared later in general. The ocular involvement was associated with severe prognosis for 12.3% (27/219) of patients with visual acuity <1/10; three had permanent blindness.
To meet our final objective, we compared our 156 confirmed patients with BD with two of the international classifications designed for an adult population.12 ,13 Both had low concordance with our expert classification. We propose a new consensus classification for paediatric BD (table 3). Six categories of symptoms were considered with their descriptions. Papilledema and headaches were the only neurological symptoms significantly associated with confirmed BD. Finally, we agreed to consider neurological symptoms as a whole but without headaches, which are not specific enough in BD.22 Our PEDBD classification does not consider a positive pathergy test result and does not mention oral aphthosis as a mandatory criteria. All symptoms categories have the same weight, especially because we do not know their respective frequencies in the general paediatric population. The new paediatric BD classification could differentiate confirmed BD, with a significantly increased number of symptoms, from unconfirmed BD and PFAPA, MKD and CAPS, as negative controls.
To conclude, we have reported the widest cohort study ever performed to define paediatric BD and its natural history. The contribution of three cohorts of children from the Eurofever registry reinforces the validity of the new classification of paediatric BD, which will be a reference for further therapeutic trials, even if it still requires external validation by an independent cohort of patients with paediatric BD.
Acknowledgments
Thanks to N Levy, K Bertaux, Marseille, France; K Sylla, A Letierce, L Coutard, Kremlin–Bicêtre, France, for the clinical research department of the AP-HP, and the Eurofever network. And to Laura Smales for reviewing English editing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figures
- Data supplement 3 - Online tables
Footnotes
Handling editor Tore K Kvien
Collaborators PED-BD international expert committee: S Ozen, H Ozdogan, A Gul, F Shahram, M Hofer, M Gattorno, R Cimaz, I Koné-Paut. The PEDBD group: French collaborators: K Retornaz, AL Jurquet, I Touitou, M Barat, Montpellier; P Quartier, A Faye, Paris, V Despert, Rennes, C Pajot, Toulouse, I Lemelle, Nancy, JL Boussioux, Martigues, TA Tran, Nimes. International collaborators: N Mikou, S Benamour, Casablanca and W Bono, Fes, Morocco; O Kasapcopur, H Ozdogan, A Gul, Istanbul, Turkey; S Al Mayouf, Riyadh, Saudi Arabia; R Khubchandani, Mumbai, India; S Assad Khalil, Alexandria, Egypt; F Davatchi, Tehran, Iran; S Hansmann, Tübingen, Germany; S Nielsen, Copenhagen, Denmark; A Benzaoui, Oran and K Tir, Algiers, Algeria; N Ruperto, A Naseli, Genoa and L Lepore, Trieste, Italy.
Contributors IK-P conceived and coordinated the study. She also obtained the grant and wrote the manuscript. IK-P, FS, MD-B, LC, RC, MG, JO, MH and SO participated each year in the consensus conference to classify PEDBD patients. All authors, except HA, AA and CP, made substantial contributions to the acquisition of data. HA contributed to the study design. IK-P, MG, AA, CP, HA and SO made substantial contributions to the analysis and interpretation of data. MG and SF provided patient data for the negative control (Eurofever data) for external validation of the paediatric BD classification. MG, FS, RC, JA, SO and CP helped draft the manuscript. All authors read and approved the final manuscript.
Funding This study was supported by the AP-HP Programme hospitalier de recherche clinique, (PHRC2007) of the French ministry of health (no. AOR07002).
Competing interests IK-P has received consultancy fees from SOBI Biovitrum, Novartis, Pfizer, Abbvie, Roche Chugai and speaker fees from Pfizer and Novartis. She also received clinical research support from SOBI Biovitrum and Roche Chugai. JA has received consulting fees from Pfizer, Abbvie, SOBI, Roche and Novartis and a research grant from Roche and Novartis. MH has received consulting fees from Novartis and Abbvie and research grant from Abbvie. IT-T has received personal fees from Servier and Abbvie. JK-D and MG has received speaker fees from Novartis and SOBI. SO has received speaker fees from SOBI and consulting fees from Novartis.
Ethics approval IRB approval was obtained.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional unpublished data are available to the main investigators and statisticians in a database located at the research unit of the Bicêtre hospital.