Article Text

Abstract
Objective Disease-modifying antirheumatic drug (DMARD)-free sustained remission, the sustained absence of synovitis after cessation of DMARD therapy, is a relevant long-term outcome of rheumatoid arthritis (RA) if (1) its occurrence is promoted by treatment and (2) this status reflects resolution of symptoms and disability. This study investigated both items.
Methods 1007 patients with RA diagnosed between 1993 and 2011, included in the Leiden Early Arthritis Clinic, were studied on achieving DMARD-free sustained remission. Patients included in 1993–1995 were initially treated with non-steroidal anti-inflammatory drugs, in 1996–1998 mild DMARDs were started early, from 1999 onwards methotrexate was initiated promptly and from 2005 onwards disease activity score (DAS)-steered treatment was common. Remission rates were compared using Kaplan–Meier curves and Cox proportional regression.
Results In total, 155 patients achieved DMARD-free sustained remission. Specific treatment strategies were significantly associated with achieving remission (p<0.001). Cox regression adjusted for anticitrullinated protein antibody/rheumatoid factor, swollen joint count, erythrocyte sedimentation rate, C-reactive protein revealed HRs for DMARD-free sustained remission of 1.13 (95% CI 0.48 to 2.64) in patients diagnosed in 1996–1998, 2.39 (1.07 to 5.32) in patients treated with early methotrexate (inclusion 1999–2004) and 3.72 (1.60 to 8.62) in those treated early with methotrexate and DAS-steered therapy (inclusion 2005–2011). At the time of remission, the Health Assessment Questionnaire was at the level of the general population (median 0.13, IQR 0–0.63). Also, patient-rated visual analogue scale (VAS) morning stiffness, fatigue, pain and disease activity were low (median (IQR) mm, 14 (2–27), 10 (0–47), 6 (0–20), 7 (0–20), respectively).
Conclusions More intensive treatment strategies increased the chance for DMARD-free sustained remission, indicating that RA chronicity can be influenced. Patients with RA achieving DMARD-free sustained remission have a normalised functional status.
- Rheumatoid Arthritis
- Outcomes research
- Patient perspective
Statistics from Altmetric.com
Introduction
The disease prospects of patients newly diagnosed with rheumatoid arthritis (RA) today are much better than they were decades ago.1 The severity of joint destruction has decreased during the last years, and nowadays, clinically relevant joint destruction has become infrequent in Western countries. These advances are the result of several changes in treatment strategies. Whereas in the early 1990s disease-modifying antirheumatic drugs (DMARDs) were commenced within two years after symptom onset, DMARDs are—according to current guidelines—started directly after the diagnosis RA is made. Second, more potent DMARDs have been introduced as first-line therapy and biologics have become available. Finally, during the last 10 years disease activity-guided treatment adjustments have become common.
Since joint destruction has become less relevant long-term disease outcome, other long-term outcomes will become more important. DMARD-free sustained remission is defined as the absence of sustained synovitis after cessation of DMARD therapy and is an interesting long-term outcome as it reflects loss of arthritis persistence. Because this definition intends to reflect a final disease outcome, it is different from remission outcomes that are assessed to measure treatment efficacy (for instance, clinical remission or low-disease activity). Observational studies and clinical trials have reported that DMARD-free sustained remission can be achieved in approximately 10–15% of the patients with RA.2–6
Several questions regarding the outcome DMARD-free sustained remission remain to be answered. First, it is yet unknown whether this disease outcome is modifiable with antirheumatic treatment. We hypothesised that disease persistence (measured by its counterpart DMARD-free sustained remission) is influenced by treatment. To study this, we evaluated if patients that were treated with current treatment regimens achieve DMARD-free sustained remission more often than patients that were treated one or two decennia ago. If no difference could be observed, DMARD-free sustained remission is not a relevant long-term treatment goal; however, if up-to-date treatment strategies increase the occurrence of DMARD-free sustained remission, it is an important outcome to pursue. Second, the definition of DMARD-free sustained remission is based on joint swelling exclusively (that requires being persistently absent). In order to explore the quality of this disease outcome for patients, we studied the functional status and patient-reported symptoms such as pain and morning stiffness at the time when DMARD-free sustained remission was achieved. Finally, we answered the question whether variation in time after diagnosis until achieving DMARD-free sustained remission might reflect different patient subsets. We hence evaluated if patients that achieved DMARD-free sustained remission early, intermediate or late in disease course differed in clinical, functional or patient-reported symptoms.
Patients and methods
Patient population
Patients studied were included consecutively in the Leiden Early Arthritis Clinic (EAC) between February 1993 and April 2011. The EAC is described elsewhere in detail.7 In short, inclusion required the presence of confirmed synovitis and a symptom duration <2 years. At baseline and yearly follow-up visits, questionnaires were filled, joint counts performed and laboratory investigations made.
From the total cohort (n=2731), patients that fulfilled the 1987 American College of Rheumatology criteria for RA8 during the first year were selected (n=1007). Patients with RA were treated according to routine care and the rheumatologists’ judgements. The treatment strategies that were usually applied changed over time. Generally, patients included in 1993–1995 were initially treated with non-steroidal anti-inflammatory drugs (NSAIDs) and DMARDs were started with delay, patients included in 1996–1998 were treated with mild DMARDs (mainly hydroxychloroquine or sulphasalazine) promptly after diagnosis and patients included from 1999 onwards were treated initially with methotrexate. Disease activity score (DAS)-steered treatment adjustments became common from 2005 onwards. These inclusion periods were used as a proxy for the changes in treatment strategies.
DMARD-free sustained remission
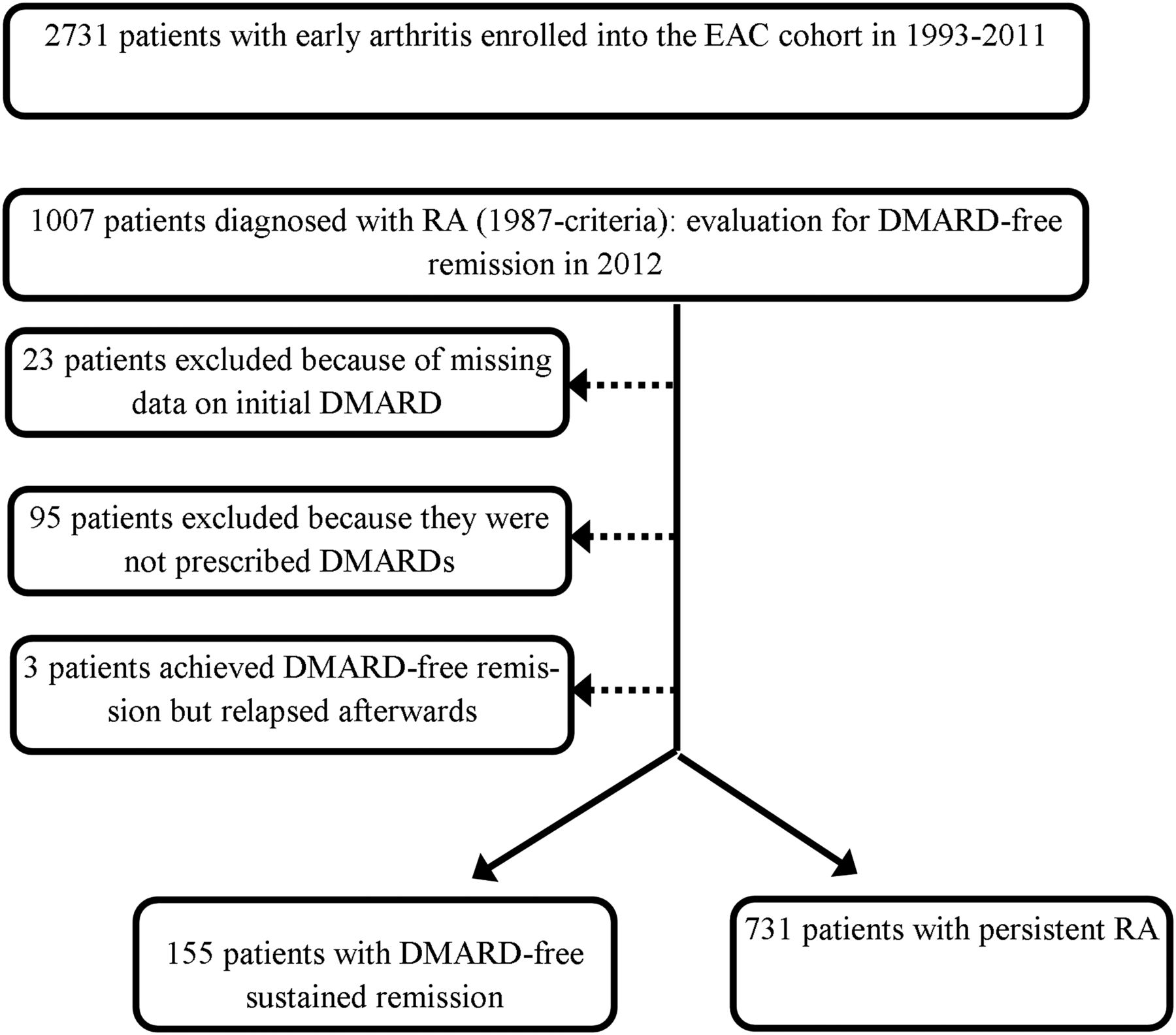
The outcome DMARD-free sustained remission was defined as the sustained absence of synovitis (by physical examination) after discontinuation of DMARD therapy (including biologics and systemic or intra-articular corticosteroids) for the entire follow-up and at least for one year after DMARD withdrawal.4 ,9 This stringent definition of remission is the opposite of disease persistence. All medical files were explored on this outcome until 5 April 2012. Patients that had achieved DMARD-free sustained remission but relapsed later on (n=3) were excluded (figure 1).

Flow diagram of the selection of the study participants. DMARD, disease-modifying antirheumatic drug; EAC, Leiden Early Arthritis Clinic; RA, rheumatoid arthritis.
The time till achieving DMARD-free sustained remission was rather arbitrarily divided into three groups: the ‘early remission’ group, when remission was achieved within three years after baseline, the ‘intermediate remission’ group, when remission was achieved between 3 and 5 years after baseline, and the ‘late remission’ group, when remission was obtained after 5–13 years.
Statistical analysis
The χ2, t test, one-way analysis of variance and Kruskal–Wallis tests for group comparisons were used. Rates of achieving DMARD-free sustained remission were evaluated using Kaplan–Meier analysis with period of inclusion entered as grouping factor. The date of remission was defined as 1 year after the date at which DMARDs were withdrawn due to remission of disease. Time to remission was measured as the time from date of inclusion in the cohort to the date of remission. Cases that did not achieve remission were right-censored by their last known date of assessment. Equality of time-to-event function between the groups was tested with log-rank test. Cox proportional hazards regression models were used incorporating adjustments for the anticitrullinated protein antibody (ACPA)/rheumatoid factor (RF) status and measures of inflammation (swollen joint count (SJC), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR)).
A multivariate normal regression was used to depict the course of several features over time; it was not intended to test for statistical significances. Because Health Assessment Questionnaire (HAQ) and patient-assessed outcomes are known to vary with age and to be different for men and women,10 ,11 adjustments were made for age and gender. The multivariate normal regression takes advantage of within-patient correlation in repeated measurements and can handle missing data. The remission group, effect of time and interaction term between these variables were entered as categorical variables into the model. The best-fit covariance matrix (unstructured) was chosen according to the smaller value of the Akaike information criterion. Analyses were performed with the IBM SPSS, V.22 (SPSS, Chicago Illinois, USA).
Results
Frequency of DMARD-free sustained remission over time
Table 1 presents the baseline characteristics of the 155 patients with RA who achieved DMARD-free sustained remission and the 731 patients who did not achieve it. In line with what has previously been described,4 patients who achieved DMARD-free sustained remission, compared with those who did not, were less often ACPA or RF positive (18% vs 62%, and 31% vs 65%, both p≤0.001) and had shorter symptom duration at inclusion (median (IQR) of 3 months (2–7) vs 5 months (2–9), p≤0.001). Patients who achieved remission, compared with those who still had persistent RA through the study period, did not have milder disease characteristics at baseline in terms of SJC, tender joint count (TJC), ESR, CRP, HAQ, morning stiffness, fatigue and frequency of high titre of ACPA.
Baseline characteristics of the patients with RA in the study in total and according to achieved DMARD-free sustained remission or not during the follow-up
Subsequently, the patients with RA were split into the four inclusion periods. Patients included in the more recent inclusion periods were less often ACPA-positive, had lower SJC and lower levels of acute phase reactants but they had more pain and morning stiffness at the first visit (table 2). Of these statistical differences, the difference in SJC was mostly clinically relevant (the median SJC of 12 in 1996–1998 and of 6 in 2005–2011). Distribution of high and low titres of ACPA was equal in the inclusion periods. Figure 2 presents the Kaplan–Meier estimates of the percentages of patients achieving DMARD-free sustained remission stratified by periods of inclusion. Patients that were treated according to more recent treatment strategies achieved remission more often (p<0.001). The mean time to remission (SD) was 7.8 (3.4), 6.9 (4.0), 4.8 (2.7) and 3.1 (1.4) years for patients treated with the subsequent treatment strategies.
Baseline characteristics of the patients with RA according to period of inclusion

Kaplan–Meier estimates of the percentages of patients with rheumatoid arthritis achieving disease-modifying antirheumatic drug (DMARD)-free sustained remission, stratified for the different treatment strategies. The periods of inclusion were used as proxy for the differences in treatment strategy. Patients included in 1993–1995 were initially treated with non-steroidal anti-inflammatory drugs and DMARDs were initiated with delay, patients included in 1996–1998 were treated early with mild DMARDs (mainly hydroxychloroquine or sulphasalazine) and patients included from 1999 onwards were promptly treated with methotrexate (MTX) and disease activity score (DAS)-steered treatment adjustments became common from 2005 onwards. Pooled over strata p≤0.001 by log-rank test, test for trend p≤0.001. Remission was achieved in 7 patients out of 63 patients included in 1993–1995, in 24 out of 158 patients included in 1996–1998, in 66 out of 289 patients included in 1999–2004 and in 58 out of 376 patients included in 2005–2011.
To determine whether shorter follow-up for part of the patients in the last inclusion period and difference in follow-up time in different inclusion periods had influenced the results, the Kaplan–Meier analyses were repeated (1) limiting the latest inclusion period till January 2009, thus allowing for duration of follow-up of at least 3 years, and (2) limiting the maximal follow-up to 5 years. The difference between the treatment groups remained statistically significant (both analyses p<0.001, see online supplementary figure S1). The Kaplan–Meier analyses were also repeated in the ACPA-positive and ACPA-negative subgroups, both showing significant results (p=0.001 and 0.014, respectively), but DMARD-free remission was more frequent in the ACPA-negative groups (online supplementary figure S2).
In Cox proportional hazards regression, the association between achieving remission and treatment strategy was confirmed; with the inclusion period 1993–1995 (initial treatment with NSAIDs) as reference, the HRs (95% CI) for the patients initially treated with mild DMARDs (inclusion 1996–1998), initially treated with methotrexate (1999–2004) and then with methotrexate and DAS-steered treatment (2005–2011), were 1.5 (0.6 to 3.4), 2.9 (1.3 to 6.4) and 5.3 (2.3 to 12.1), respectively. After adjustment for serological status, baseline SJC, ESR and CRP the HRs were 1.13 (0.48 to 2.64), 2.39 (1.07 to 5.32) and 3.72 (1.60 to 8.62), respectively, showing an increased chance for DMARD-free sustained remission in patients treated according to more recent strategies.
Disease symptoms and functional status at the time of achieving DMARD-free sustained remission
The definition of DMARD-free sustained remission is based on the absence of swollen joints; other clinical measures and functional and patient-reported symptoms are not included in the definition. We therefore explored other disease-associated outcomes at the time of achieving remission. Of all 155 patients with remission, information on follow-up visits was missing in 48%. The missing data were completely not at random as patients with DMARD-free sustained remission declined their visit to the research nurse more often than patients with RA with persistent disease. Patients with complete data and with missing data at the time when DMARD-free sustained remission was achieved did not differ statistically significant by age, sex, symptom duration, year of inclusion and baseline disease characteristics, except for patients’ rated disease activity (median visual analogue scale (VAS) (mm) in patients with and without missing data 53 (36–72) and 47 (31–61), p=0.032). Obtained data were studied and missing data were not imputed.
The median TJC at the time of remission was 0 (IQR 0–1) and at a group level acute phase reactants were within normal limits (median (IQR) ESR 8 (5–11) mm/h and CRP 3 (3–5) mg/L). Regarding functional ability, we observed that the patients that achieved DMARD-free sustained remission had a median HAQ at diagnosis of 1.0 (IQR 0.62–1.50) (table 1) and at the time of remission of 0.13 (IQR 0–0.63) (table 3). The VAS fatigue median was 40 (12–60) mm at baseline but 10 (IQR 0–47) at the time DMARD-free sustained remission was obtained. Also, the VAS pain was low at the time of DMARD-free sustained remission, median 6 (IQR 0–20), while it was 48 (29–65) at baseline. The VAS morning stiffness decreased also to low levels in the patients that achieved remission; its median was 57 (36–76) mm at baseline and 14 (2–27) at the time of remission (table 3).
Disease characteristics of the patients with RA at the time of achieved DMARD-free sustained remission in total and by groups according to time to remission after inclusion
Analyses in patients with RA that achieved DMARD-free sustained remission early, intermediate or late in disease course
It was observed that the time till DMARD-free sustained remission varied between the patients. Theoretically, the rapidity with which DMARD-free remission is achieved may reflect differences in patient subsets. To explore this, characteristics of the patients that achieved DMARD-free sustained remission early (within 3 years), intermediate (3–5 years of disease) or late (5–13 years) in disease course were compared. No differences were observed either at baseline (online supplementary table S1) or at the time of achieved DMARD-free sustained remission (table 3). In order to illustrate the time course of HAQ and patient-reported symptoms in patients that achieved DMARD-free sustained remission early, intermediate and late in disease course, the median values as predicted by normal regression with adjustments for age and gender were plotted (figure 3). As a reference, the course of these variables for patients with persistent RA was plotted. The course of the CRP, ESR and TJC over time was depicted likewise (online supplementary figure S3). In all patients, the largest improvement was shown in the first year. Better outcomes across all measures were observed in the patients who achieved remission compared with those who did not.

{kind=link}
{kind=link}
{kind=link}
Depicted is the course of patient-reported disease features by time to achieved remission early, intermediate and late in disease course. Presented are predicted median values obtained by the multivariate normal regression model adjusted for age at inclusion and gender. Patients that achieved disease-modifying antirheumatic drug-free sustained remission within 3 years after inclusion, after 3–5 years or between 5 and 13 years were referred to as early, intermediate and late remission. The lines representing the remission subgroups terminate at follow-ups with available data. As reference, the predicted values for the group of patients that did not achieve remission (dotted lines) are also shown. HAQ, Health Assessment Questionnaire; RA, rheumatoid arthritis; VAS, visual analogue scale.
Discussion
This study explored the relevance of achieving DMARD-free sustained remission in two domains. Because DMARD-free sustained remission is generally considered to be an outcome that is obtained in only a minority of patients with RA and that the persistent nature of RA cannot be modified, the first aim was to evaluate whether the incidence of DMARD-free sustained remission changed with the use of up-to-date treatment strategies. The present data revealed indeed an increase in chance for DMARD-free sustained remission when patients were treated according to early and more intensive strategies in standard clinical practice. These findings are relevant as these data imply that also persistence of inflammation (which is the second hallmark of RA next to joint destruction) can be influenced. Significant differences were seen for the two most recent inclusion periods 1999–2011. Whether DAS-steered treatment is of additional value compared with initial methotrexate alone cannot be definitely concluded based on the present data as the follow-up duration of the inclusion period 2005–2011 was shorter than that of the other inclusion periods. But prompt treatment with methotrexate is clearly beneficial.
As DMARD-free sustained remission is defined by the findings of rheumatologists at physical examination, second, we evaluated whether this disease outcome is also relevant from the patient perspective. It was observed that when DMARD-free sustained remission was achieved the median HAQ score was 0.13. The mean HAQ for the normal population is reported to be 0.25;12 this suggests that the functional ability at the time DMARD-free sustained remission is achieved is normalised. Several patient-reported symptoms were studied. The VAS pain on a 100 mm scale in the general population is reported to be 11.5 and the VAS fatigue 20.5. Also, here the VAS scores at the time of DMARD-free remission (6 and 10, respectively) were lower than the reference values,13–16 suggesting that important RA-related symptoms as pain and fatigue have resolved. Together, these observations indicate that DMARD-free sustained remission is a disease outcome reflecting health state close to expected in the general population with regard to functioning and several RA-related symptoms.
DMARD-free sustained remission was defined as the absence of synovitis after DMARD cessation during the total follow-up that should be at least one year. The follow-up duration after DMARD cessation may potentially influence the outcome. Patients that have 1 or 2 years' follow-up after DMARD cessation might flare later on while they are now classified as being in DMARD-free sustained remission, whereas patients with a longer follow-up after DMARD cessation and who flared after several years of remission are not in the DMARD-free remission group. This might be an issue for the fourth inclusion group; all other inclusion groups were followed for many years. In a subanalysis, patients included after 2009 were excluded and patients included in 2004–2009 only were studied, thus allowing three follow-up years for all patients. The results were unchanged, suggesting a minor influence of the shorter follow-up of the fourth inclusion group.
Patients included in the more recent inclusion groups were less often ACPA-positive, the number of swollen joints fewer and acute phase reactants lower. Although all patients studied fulfilled the 1987 criteria for RA, this may suggest that these patients had somewhat milder disease at the time of diagnosis. Also when adjustments were made for these baseline differences, patients treated according to recent protocols achieved DMARD-free sustained remission significantly more often. The finding of changed RA over time with better clinical status in contrast to worse reported subjective disease measures has been reported before.17 This presumably reflects a change towards diagnosing (and treating) RA in a milder disease phase in recent years and higher patients' expectation of ‘well-being’ status.18
An optimal study design to determine the effect of treatment strategies on DMARD-free sustained remission is a randomised clinical trial. However, at present, it will not be considered ethical to perform a trial with study arms using outdated treatment strategies. We used the longitudinal data of our observational cohort in which patients were treated according to the rheumatologists’ expertise. We used the different time periods as proxies for different treatment strategies and the oldest inclusion group as reference.
It is known that the symptom duration at treatment initiation importantly affects the chance for DMARD-free sustained remission.19 There were no large differences in symptoms duration between the inclusion periods (table 2), and when symptom duration was added as adjustment factor, the HRs were mostly unchanged (data not shown). Hence, symptom duration did not confound the results.
The biological mechanisms underlying RA persistence are unknown. We questioned whether patients that achieved DMARD-free sustained remission early in the disease constitute a different subset of patients than those that achieve it later on. We compared patient characteristics and ACPA titres between these groups at baseline and at the time of DMARD-free sustained remission and observed no relevant differences.
DMARD-free sustained remission was also achieved in patients that carry autoantibodies. In total, 31% of the patients with DMARD-free sustained remission were RF-positive and 18% were ACPA-positive. Thus, the presence of autoantibodies does not absolutely impede achievement of this outcome. Exploratory analyses within ACPA-positive and ACPA-negative subgroups showed significant differences for the treatment strategies (online supplementary figure S2). Although RA persistence is more frequent in ACPA-positive RA, the present data suggest that treatment affects RA persistence in both ACPA-negative and ACPA-positive RA. More detailed studies on these subgroups are needed.
Presumably the mechanisms that promote the development of DMARD-free sustained remission, and thus the loss of RA persistence, are different from the mechanisms mediating treatment response. In this light it is interesting to note that the predictors of DMARD-free sustained remission (ACPA, symptom duration) are different from previously reported predictors for DAS response (male gender, older age, lower body mass index, lower baseline disease activity).20–22
The major limitation of our study is that a proportion of patients with DMARD-free sustained remission declined their research visits during remission (they were seen by rheumatologists only). ‘Feeling well’ might be causative for this. If this would have introduced bias, the results obtained are likely derived from the worst selection of patients with DMARD-free sustained remission because the patients who had the best physical function or the least symptoms in particular refused further study participation. We did not observe large differences in baseline characteristics between DMARD-free remission patients with and without data at the time of remission.
In conclusion, RA can no longer be considered as an inevitably chronic disease. The results of the present study indicate that DMARD-free sustained remission is increasingly achievable in the recent years of early and intensified antirheumatic therapy. Therefore, DMARD-free sustained remission is an advantageous long-term disease outcome that is relevant to pursue.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
Contributors SA, HWvS, TWJH and AHMvdH-vM contributed to the study concept. SA and HWvS performed the data analyses. SA drafted the manuscript. JABvN and LEB were responsible for selection of patients and the data collection. All authors contributed to revising and adjusting the manuscript and approved the final manuscript.
Funding This work was supported by the Dutch Arthritis Foundation and a Vidi-grant of the Netherlands Organization for Scientific Research, the Swedish Rheumatism Association, the regional agreement on medical training and clinical research (ALF) between Stockholm County Council and Karolinska Institutet and King Gustav V 80 year's Foundation.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Local Medical Ethical Committee, Leiden University Medical Center, the Netherlands.
Provenance and peer review Not commissioned; externally peer reviewed.