Article Text

Abstract
Objective To compare the presence of cardiovascular (CV) risk factors and established CV disease in patients with psoriatic arthritis (PsA) and the general population and to compare the 10-year risk of a fatal CV event calculated by the Systematic Coronary Risk Evaluation (SCORE) algorithm.
Methods Patients with PsA (n=338) and controls (n=50 468) were recruited from the Nord-Trøndelag Health Study 3. Age-adjusted and sex-adjusted prevalence rates of CV risk factors and comorbidity were calculated and the SCORE algorithm was applied.
Results There was an increased prevalence of angina pectoris (5.0% vs 3.6%, p=0.01), history of percutaneous coronary intervention (2.4% vs 1.4%, p=0.04), hypertension (45.3% vs 39.3%, p=0.01), obesity (32.0% vs 22.4%) and tobacco smoking (21.3% vs 16.4%, p=0.02) in patients with PsA compared with controls. Patients with PsA had elevated levels of C reactive protein (CRP; p<0.001), body mass index (BMI; p<0.001) and triglycerides (p=0.01). The median calculated CV risk in patients with PsA was low and comparable with controls (0.87 vs 0.83, p=0.24). The distribution across CV risk classes was similar among patients with PsA and controls.
Conclusions Patients with PsA have a higher risk of CV disease than the background population, although there was no difference between groups in 10-year risk of a fatal CV event estimated by SCORE. However, patients with PsA had elevated levels of CV risk factors not included in the SCORE algorithm, such as BMI, triglycerides and CRP.
- Arthritis
- Psoriatic Arthritis
- Cardiovascular Disease
- Epidemiology
Statistics from Altmetric.com
Introduction
Psoriatic arthritis (PsA) is a chronic inflammatory disease characterised by arthritis and/or entheseal inflammation and psoriasis1 with reported prevalence rates ranging from 0.01% to 0.67%.2–5 In recent years, inflammatory rheumatic joint disorders have been recognised as an important risk factor for cardiovascular (CV) disease (CVD). In the latest European Society of Cardiology (ESC) guidelines for CVD prevention, immunological diseases are presented for the first time as a high-risk factor for CVD.6 Novel risk factors for CVD such as inflammation have been studied and documented more extensively in rheumatoid arthritis (RA). An elevated CV risk in patients with PsA compared with the general population has been indicated,7 ,8 and an increased prevalence of both traditional and novel CV risk factors has been reported.9 However, the underlying causes for increased risk of CVD in patients with inflammatory joint diseases are not entirely understood.
The data presented in this study were retrieved from one of the largest and most extensively mapped epidemiological cohorts available, the Nord-Trøndelag Health Study (HUNT) 3.10 ,11 Population-based studies such as the HUNT studies are pivotal for knowledge on prevalence and incidence of CV risk factors and disease.12–14 Moreover, a recent study reported a substantially higher prevalence of PsA in the HUNT3 population compared with other populations.2 The main objective of this study was to explore the prevalence of CV risk factors and established CVD in a population-based cohort of patients with PsA compared with the background population. Furthermore, we aimed to estimate the 10-year risk of a fatal CV event in patients with PsA by applying the European Systematic Coronary Risk Evaluation (SCORE) algorithm.
Materials and methods
Study population
The HUNT studies are total population-based cohorts from the 1980s, covering 125 000 Norwegian participants; HUNT1 (1984–1986), HUNT2 (1995–1997) and HUNT3 (2006–2008).10 Data presented in this study were retrieved from HUNT3. The three HUNT surveys contribute to important knowledge regarding health-related lifestyle, prevalence and incidence of somatic disease and health determinants. Comprehensive non-responder analyses have been performed for the HUNT studies.10 ,11 ,15 The participation rate has declined between consecutive HUNT surveys as in most other population-based studies.16 The geographic, demographic and occupational structure is fairly representative of Norway as a whole.10 A total of 93 680 adults were eligible for participation in HUNT3, and of these, 50 807 participated (54.1%). In all three surveys, more women than men participated, and the highest participation was in the middle aged and the elderly (aged 50–79 years) with lower participation in the oldest (>80 years) and in age groups <40 years.10 In HUNT3, non-participants had lower socioeconomic status, higher mortality and showed higher prevalences of several chronic diseases including CVD and diabetes mellitus, while opposite patterns were found for common problems such as musculoskeletal pain, urine incontinence and headache.11 Participants provided informed consent. HUNT3 was approved by the Regional Committee for Medical Research Ethics and the Norwegian Data Inspectorate Board.
PsA diagnoses validated in HUNT3
Questionnaire 1 in HUNT3 included questions about psoriasis, RA and ankylosing spondylitis (AS). Persons who answered that they had psoriasis received a more detailed questionnaire including a question if they had PsA. In total, 1238 persons reported that they suffered from either PsA, RA and psoriasis or AS and psoriasis. The medical records of these persons were evaluated by a rheumatologist (MH) to validate the PsA diagnosis. The diagnoses were also tested against the Classification of Psoriatic Arthritis (CASPAR) criteria. Controls were all participants in HUNT3 without a diagnosis of PsA. The validation and inclusion of PsA patients have previously been presented in detail.2
CV risk evaluation
Information about CV risk factors and disease was collected by self-administered questionnaires, clinical measurements and blood samples. In the questionnaire patients reported if they ever had experienced angina pectoris, myocardial infarction (MI), diabetes mellitus, cerebral stroke (ischaemic or haemorrhagic) or if they had undergone coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI). Physical activity was recorded as never, less than once a week, once a week, two to three times a week or every day. Current smokers were defined as daily cigarette smokers.
Measurements of height to the nearest 1 cm, weight to the nearest 0.5 kg and waist circumference were recorded. The participants wore lightweight clothing and no shoes during these measurements. Body mass index (BMI) was calculated as weight in kilograms divided by height squared in metres. Blood pressure (BP) was measured three times (Dinamap 845XT Criticon) and the average of the second and third measurement was used in the analysis. In case of missing values on BP, we preferably used the third, and then second or first BP measure. Hypertension was defined as systolic BP ≥140 mm Hg and/or diastolic BP ≥90 mm Hg or ever use of antihypertensive medication.
Non-fasting blood samples were analysed for serum micro C reactive protein (CRP), triglycerides, total cholesterol and high-density lipoprotein cholesterol (HDL-c) at a central laboratory at the Levanger Hospital by standardised methods. Low-density lipoprotein cholesterol (LDL-c) was calculated using the Friedewald formula.17 For the analysis of LDL-c, we excluded those with triglyceride concentrations of ≥4.5 mmol/L.
Systematic coronary risk evaluation
The 10-year risk of a fatal CV event was calculated using the SCORE algorithm which includes age, sex, smoking status, systolic BP and total cholesterol/HDL-c ratio18 and categorised into four groups according to the latest guidelines: low risk <1%, moderate risk 1%–4%, high-risk 5%–9% and very high risk ≥10%.19 Both the ESC and European League against Rheumatism (EULAR) recommend the SCORE algorithm for CV risk assessment in patients with chronic inflammatory joint diseases.6 Norway belongs to low CV risk region and accordingly uses the low risk version of the SCORE algorithm. Patients with a history of MI, stroke, CABG, PCI or diabetes mellitus are in the latest ESC guidelines automatically classified as having a very high risk of CVD, and a SCORE calculation is therefore not necessary.18
Statistics
Statistical analyses were performed using SPSS, V.21.0. Statistical significance level was defined as p<0.05 on the basis of two-sided tests with no adjustments made for multiple comparison. Values are expressed as the mean±SD, non-parametric values as the median with IQR. Student’s t test, χ2 test and logistical regression analyses were performed for group comparison. Multivariable analyses adjusting for age, sex and BMI were performed by logistical regression (dichotomous outcome variables) or linear regression (continuous outcome variables).
Results
Study enrolment is presented in figure 1. Among the 338 patients with PsA who were identified, 323 patients (95.6%) fulfilled the CASPAR criteria for PsA. All patients with PsA had psoriasis and arthritis, but data on serology were unavailable for some, which contributed to their failure to fulfil the CASPAR criteria.
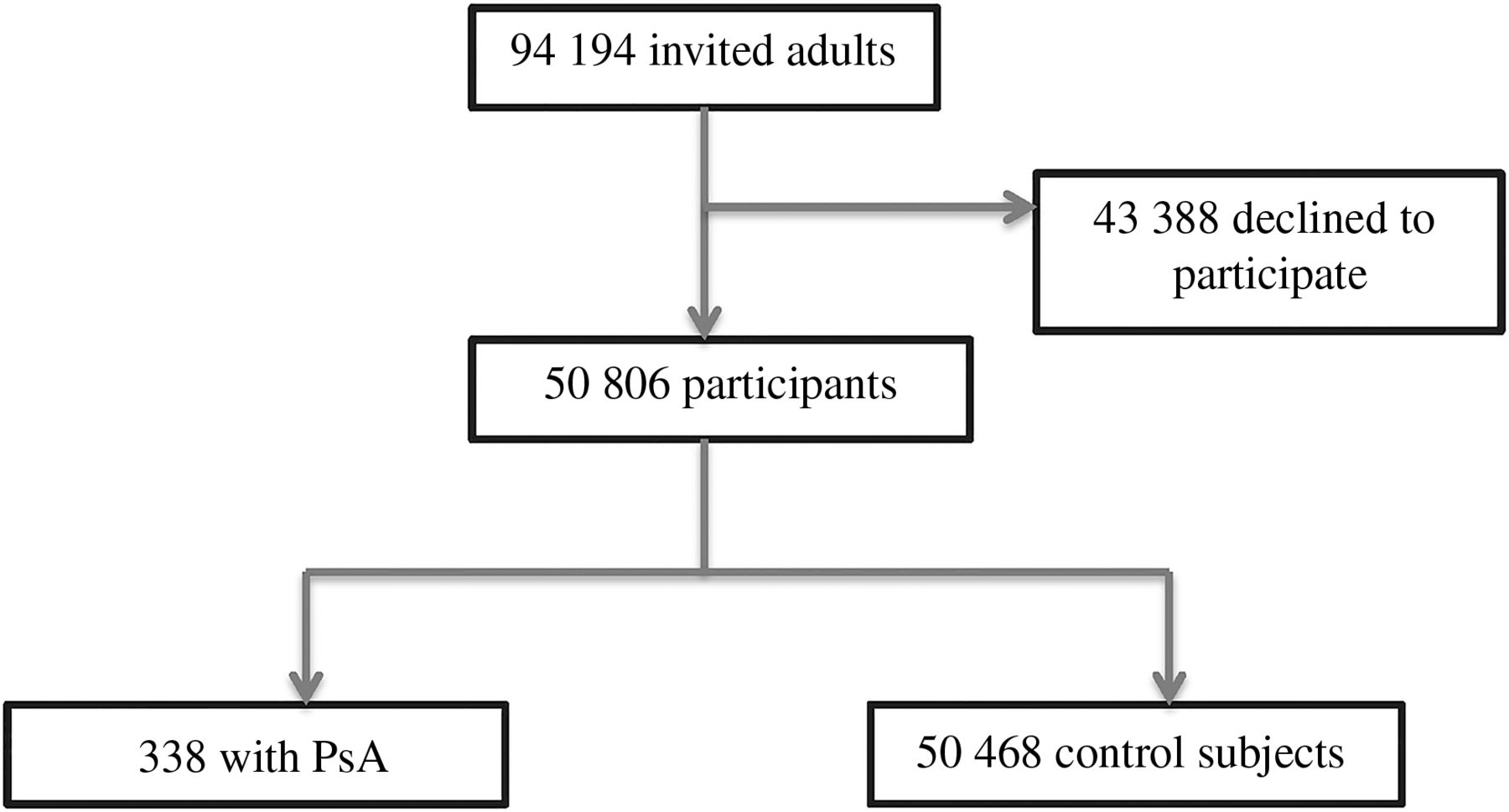
Selection of patients with psoriatic arthritis (PsA) and control subjects from the Nord-Trøndelag Health Study (HUNT) 3 study.
Table 1 shows demographical and disease-related characteristics and CV risk factors of the patients with PsA and control subjects included.
Demographics, clinical characteristics and cardiovascular risk factors for patients with psoriatic arthritis (PsA) and control subjects
Mean±SD age was 54.3±11.9 and 53.9±16.1 years in PsA and controls, respectively (p=0.58) and the sex ratio was equal in both groups (p=0.31). Disease duration among patients with PsA was 9.2±7.6 years. Patients with PsA had significantly higher median CRP than controls (2.1±4.2 vs 1.2±2.1, p<0.001).
Patients with PsA more often had hypertension than controls (45.3% vs 39.3%, p=0.01). The adjusted OR for hypertension was 1.39 (95% CI 1.10 to 1.75). This difference was attenuated after also adjusting for BMI (p=0.09).
Patients with PsA were found to have significantly higher age-adjusted and sex-adjusted mean BMI (28.4±4.6 SD vs 27.2±4.4 SD, p<0.001) and diastolic BP (74.7±11.8 vs 73.4±11.3, p=0.02) than control subjects. There was a significantly higher prevalence of obesity defined as BMI ≥30 kg/m2 in the PsA group (32.0% vs 22.4%, p<0.001). Patients with PsA were also more likely to report daily smoking compared with controls (21.3% vs 16.4%, p=0.02). We found a significantly higher level of triglycerides in patients with PsA compared with controls (1.77±0.94 vs 1.63±1.01, p=0.01) but not a significant difference in other lipids (total cholesterol, HDL-c or LDL-c).
The prevalence of CV comorbidities is presented in table 2.
Prevalence of self-reported cardiovascular risk factors and disease among patients with psoriatic arthritis (PsA) compared with control subjects
After adjusting for age and sex there was a higher prevalence of angina pectoris (5.0% vs 3.6%, p=0.01) and history of PCI (2.4% vs 1.4%, p=0.04) in patients with PsA compared with controls. Total CVD was defined as one or more of angina pectoris, MI, cerebrovascular stroke, CABG or PCI and there was no difference between groups (8.0% in both groups, p=0.20).
CV risk calculated by SCORE
Forty-five (13.4%) patients with PsA and 5719 (11.3%) controls (p=0.25) were allocated in the very high CV risk group due to the presence of established CVD or diabetes mellitus. The median risk calculated by the SCORE (±IQR) was comparable between the two groups (0.87±0.33–2.14 in the PsA group vs 0.83±0.22–2.22 in the control group, p=0.22; table 3).
Cardiovascular risk according to the SCORE in psoriatic arthritis (PsA) patients and control subjects
The similar CV risk among patients with PsA and control subjects was present in all the four CV risk classes (p=0.24; figure 2). There was no association between disease duration and CV risk group (9.5±7.9 years in patients with PsA with low or intermediate risk compared with 9.2±7.6 years in those with high or very high risk).

{kind=link}
{kind=link}
Cardiovascular risk group according to Systematic Coronary Risk Evaluation in patients with psoriatic arthritis (PsA) and controls.
Discussion
This large population-based study shows an increased prevalence of self-reported angina pectoris, hypertension and history of PCI in patients with PsA compared with controls. There were no differences between groups regarding history of MI, CABG, cerebrovascular stroke or diabetes mellitus. However, the number of cases in these categories was very low in the PsA group and patients were rather young with respect to the development of CVD. Patients with PsA were more often smokers, whereas other traditional CV risk factors included in the SCORE (age, sex, systolic BP, total cholesterol/HDL-c ratio) were similar between the two groups. There was no difference between groups in 10-year risk of a fatal CV event estimated by the SCORE algorithm. However, patients with PsA had higher levels of CV risk factor not included in the SCORE algorithm, such as CRP, BMI, diastolic BP and triglycerides.
A large cohort study found slightly increased prevalence ratios in patients with PsA of similar age for hypertension, hyperlipidaemia, ischaemic heart disease, congestive heart failure and total CVD compared with controls.20 Others have also reported patients with PsA to have more hypertension compared with the general population.8 ,20 ,21 In our study as many as 45.3% of patients with PsA had hypertension, which is higher than previously reported.20 The difference between patients with PsA and controls was attenuated when adjusting for BMI, which indicates that obesity is a confounder and contributes to increased BP in patients with PsA. This is in contrast to a study that found a higher prevalence of hypertension in patients with PsA compared with the general population even after adjusting for BMI.21 A potential information bias regarding hypertension may be the use of some antirheumatic medication, such as non-steroidal anti-inflammatory drugs (NSAIDs), cyclo-oxygenase II inhibitors, leflunomide and ciclosporin that may affect BP.22 We did not have the information to control for the use of such drugs in the analyses, and considering that NSAIDs are available without prescription in Norway, complete data on drugs are hard to obtain.
Our data confirm the increased prevalence of obesity in PsA which has been reported previously.9 ,23 It is well known that obesity is associated with CVD, thromboembolic disease, diabetes mellitus and several other comorbidities.24 Whether obesity is a risk factor for PsA or a consequence of the disease remains a matter of debate.25–27 Patients with PsA were more likely to smoke daily and engage less in physical activity in our study. We identified two previous studies on smoking habits among patients with PsA, both of which did not find a higher prevalence of smoking among patients with PsA.21 ,28 To our knowledge, the level of physical exercise in patients with PsA compared with controls has not previously been explored.
PsA patients had an overall low risk of a fatal CV event within10 years estimated by SCORE, and the risk was not different from that in the control subjects. Except for smoking, there were no differences between patients with PsA and controls in the presence of risk factors included in the SCORE algorithm. We are only aware of one other study using the SCORE algorithm in calculating risk of CVD for patients with PsA.29 In persons without established CVD or traditional CV risks, higher SCORE mean values were reported in patients with PsA compared with controls. However, when patients were stratified into high and low CV risk groups based on SCORE, differences between groups were not found.29 Concerns have been raised about the low predictive values of risk equation tools.30–33 However, validation of such tools must be confirmed in studies with strict methodological design with representative patient cohorts. The EULAR expert committee has recommended that the SCORE is multiplied by 1.5 in selected patients with RA to better reflect their increased risk of CVD.6 Future epidemiological studies should explore the prevalence of CV risk and disease in PsA, AS and RA. This might provide information on whether PsA is a CV risk factor of the same order of magnitude as RA and whether a multiplier of the same magnitude as for RA should be applied to risk equations for PsA.
Our study reports a higher triglyceride level in patients with PsA compared with controls, but this finding was not significant when adjusting for BMI. Patients with PsA and controls had similar levels of HDL-c, LDL-c and total cholesterol. Lipid abnormalities in PsA have been reported earlier with conflicting results.7 A higher prevalence of combined dyslipidaemia (low HDL-c and high triglyceride level) in patients with PsA compared with RA and AS has previously been reported.9 Others have found lower levels of total cholesterol and LDL-c and higher levels of HDL-c in patients with PsA.21 Evidence suggests that both fasting and non-fasting triglyceride levels predict CV events,34 but in our study lipids were only measured in non-fasting blood samples. In RA it is shown that the lipids may be altered by inflammation.35–37 However, despite that patients with PsA had a higher CRP level compared with controls, the total cholesterol level did not differ between the groups.
The association between psoriasis, arthritis and CVD is complex and still not fully understood. It has been suggested that the increased risk of CVD in PsA reflects an increased prevalence of conventional CV risk factors.8 ,9 ,20 Our study of 338 patients with PsA supports these findings, as we found a significantly higher prevalence of obesity, smoking and hypertension in addition to higher triglyceride levels in patients with PsA. Interestingly, a higher prevalence of macrovascular disease defined as increased carotid artery intima media thickness has been demonstrated in patients with PsA without clinically evident CVD.38 In RA, it is shown that atherosclerosis cannot solely be explained by the presence of traditional CV risk factors, and chronic inflammation has also been proposed as being responsible for the enhanced development of atherosclerosis in these patients.39 ,40 This may also be the case for patients with PsA. Interestingly, a recent study from the HUNT survey has shown that a history of CVD is associated with increased risk of future development of RA.41 The EULAR recommendations for CVD management in patients with inflammatory arthritis emphasise the need to address both the classic and novel risk factors for CVD.6
Strengths and limitations
Strengths of this study include the population-based study design and use of objective criteria for PsA. Since this is a cross-sectional comparative study, causal association between PsA and CVD cannot be established. For this purpose, prospective long-term follow-up studies are needed. There was a relatively small number of patients with PsA (n=338), which may reduce statistical power and introduce false-negative findings (type II statistical error). Furthermore, we have not explored the relationship between clinical disease activity of PsA and the occurrence of CV risk factors and disease. The diagnoses of CVD were self-reported and not validated, representing a possible source of misclassification. This is a challenge faced by all population-based research using patient-reported disease. However, self-reported disease has been shown to be a reliable source for chronic diseases in the HUNT population.42 Others have also reported accurate recall of medical history in well-defined chronic conditions.43 Validation of CVD would require linking data from several sources (ie, hospitals, general practitioners and health registers), and ethical and legal approval procedures for such studies are very complicated.10 Combining data from different sources provides the opportunity for future sensitivity analyses of CVD prevalence, incidence and association studies. Furthermore, there was a lack of information on documented CVD by invasive or non-invasive testing, chronic renal disease, reduced glomerular filtration rate and peripheral vascular disease, which are all classified as very high CV risk factors. Patients with diabetes mellitus were excluded from the SCORE calculations, but we had no information about end-organ damage and were not able to distinguish between type I and II diabetes. One also has to keep in mind that the PsA group in our study was relatively young with respect to established CVD.
Conclusion
In this large population-based study, the prevalence of hypertension, angina pectoris, PCI, obesity and tobacco smoking was increased in patients with PsA compared with controls. Patients with PsA had an overall low risk of CV disease estimated by SCORE, which was comparable with controls. This finding is probably related to low levels of traditional CV risk factors included in the SCORE algorithm. Patients with PsA had elevated levels of CV risk factors not included in the SCORE risk algorithm such as CRP, BMI and triglycerides.
Acknowledgments
The authors would like to thank Inge Christoffer Olsen PhD and Øyvind Salvesen PhD for help with the statistical analyses. We thank the HUNT Research Centre for providing the data. The HUNT study is a collaboration between the HUNT Research Centre (Faculty of Medicine, Norwegian University of Science and Technology NTNU), Nord-Trøndelag County Council, Central Norway Health Authority and the Norwegian Institute of Public Health.
References
Footnotes
Handling editor Francis Berenbaum
Contributors AMG: Planning, statistical analyses and interpretation of the data and writing. AGS: Conception, planning, interpretation of the data, and writing. SR: Statistical analyses, interpretation of the data and writing. PRR: Statistical analyses and writing. AK: Planning and writing. SG: Statistical analyses and writing. GH: Conception, planning, interpretation of the data, and writing. MH: Conception, planning, collection of data, statistical analyses, interpretation of the data, and writing. All authors contributed with critical review of the paper, read and approved the final manuscript.
Funding AMG has received financial support from Revmafondet i Trondheim. GH has received financial support from Pfizer. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests None.
Patient consent Obtained.
Ethics approval The study was approved by the Regional Committee for Medical Research Ethics in South-Eastern Norway.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All available data are included in the manuscript.