Article Text

Abstract
Treating to target is becoming the standard of care in many medical specialities, including rheumatology. The Tight Control of Psoriatic Arthritis (TICOPA) trial has recently provided evidence of the benefit of treating to target in psoriatic arthritis (PsA), and the revised European League Against Rheumatism (EULAR) recommendations on the management of PsA suggest this approach. However, the question of the optimal measure to use and the practicalities of incorporating this into routine clinical practice remain problematic.
- Psoriatic Arthritis
- Treatment
- Outcomes research
Statistics from Altmetric.com
Treating to target (T2T) has become prevalent in many specialities across medicine including rheumatology where it has become the standard of care for patients with newly diagnosed rheumatoid arthritis (RA).1 A large international task force published recommendations on T2T in spondyloarthritides (SpA) in 2014,2 which followed an extensive literature review assessing the evidence base.3 There were no trials directly assessing T2T in SpA at that time. Despite this, the recommendations still supported the concept of T2T in SpA, based on expert opinion only.2
The T2T recommendations were concerned with SpA as a group, although specific recommendations were made for axial, peripheral and psoriatic arthritis (PsA). The overarching principles stated that the target should be based on a shared decision between patient and rheumatologist, but the recommendations did not give any specific targets which could be used.2 Clearly, the targets may vary depending on the subtype of SpA to ensure appropriate assessment of disease domains. At the EULAR annual meeting 2015 in Rome, Italy, an update to the 2012 EULAR recommendations for the treatment of PsA was presented. Given the updated literature review, and building on the previous recommendations, these recommend the use of a T2T approach in PsA,4 with new evidence from the Tight Control of Psoriatic Arthritis (TICOPA) trial.5
The TICOPA trial is the first trial to assess T2T in any of the spondyloarthropathies. This trial recruited 206 patients with early (<2 years’ symptom duration), disease modifying anti-rheumatic drug (DMARD) naïve PsA and randomised them to receive either standard care or tight control. The tight control group was reviewed every 4 weeks and treated using a step-up conventional and biologic DMARD algorithm using minimal disease activity (MDA) as the target for treatment. The standard care group was reviewed by National Health Service (NHS) rheumatologists every 12 weeks with no restrictions or guidance on their therapeutic choices. The study confirmed the benefit of this treatment approach using the MDA criteria for PsA6 as the treatment target. The trial showed a significant benefit in articular and skin outcomes (ACR20, 50, 70 and PASI75) as well as improvements in multiple patient-reported outcomes.5 Tight control was associated with an increase in adverse events, which may represent the impact of rapid escalation and higher rate of combinations of DMARDs in this arm. Of course there are limitations to the TICOPA trial, and more studies are needed to look at the different treatment strategies and the response of different subgroups, as well as to examine the impact of such strategies early in the disease course on long-term structural damage in the worst prognostic groups.
There are multiple potential targets for treatment that could be used in PsA. Clearly, remission would be the absence of tender and swollen joints, no skin disease, no dactylitis and enthesitis, and no axial activity. This definition of remission was used by Cantini et al, but is hard to achieve.7 The MDA criteria were developed by consensus and allowed some minor disease activity in the target. The MDA criteria require assessment of articular disease (a 68/66 joint count), enthesitis, skin disease (psoriasis activity and severity index (PASI) or body surface area (BSA)) and patient-reported measures (visual analogue scale (VAS) for pain and global disease activity and the health assessment questionnaire (HAQ) for function). To achieve MDA, five of the seven criteria must be met, and in the TICOPA trial roughly 30% of people were classified as being in MDA by meeting 5/7 criteria, a third by meeting 6/7 and a third by meeting all seven criteria. Of the seven criteria, the skin and tender joint count targets were missed most often (Helliwell and Coates: unpublished data). Given the TICOPA trial data, the MDA criteria clearly have the most significant evidence base with direct benefit in a trial assessing the T2T strategy. The patient-reported outcomes fit onto two sides of paper and are simple to measure. In clinical practice, these can be done in the waiting-room prior to an appointment. They take 5–10 min for the patient to complete. With regular use, the assessment of articular, entheseal and skin involvement also takes 5–10 min. Indeed, while we would advocate a full evaluation of these domains, for the purposes of MDA the individual cut points can be assessed quickly. For example, a quick appraisal of skin disease will reveal whether there is more than 3% body surface area and an exact BSA or PASI need not be recorded. The criteria are therefore relatively quick and feasible to perform but do not give a level of disease activity or response.
The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) have developed and tested a number of composite measures, which answer these limitations (table 1).8 ,9 The composite psoriatic disease activity index (CPDAI) was developed by FitzGerald based on the GRAPPA grid10 and it assesses disease activity and impact in five domains.8 It provides a composite score of 0–15 and also allows easy identification of domains that are active. This was not data driven but was designed to include all of the principal domains of PsA to ensure full assessment. Both the Psoriatic Arthritis Disease Activity Score (PASDAS) and GRAPPA Composite Exercise (GRACE) index were developed as part of an international GRAPPA exercise. Both measures include physician and patient-reported outcome measures combined into a composite index. The calculation of both is more complex than other measures but can be performed using a computer spreadsheet. These were developed from patient data (over 500 cases worldwide) identifying, in the case of the PASDAS, key outcome measures that predicted the decision to escalate treatment. They therefore reflect clinical decision-making, as well as include key domains of disease. However, they are more complex to perform and calculate and have thus far been used only in clinical trials.
Composite measures available for assessing psoriatic disease
All three of these (CPDAI, PASDAS and GRACE) are composite disease activity measures and have proposed response levels and cut-offs for disease activity based on physician and patient opinion.11 The proposed cut-offs now give a combined response measure assessing change from baseline and absolute final score, analogous to the EULAR responses in RA. These measures are derived from patient data, provide an overall assessment of disease activity across the domains and provide both a measure of disease activity at one time point and response over time. However, they do take significantly longer to perform in clinic than the MDA criteria and require a more complex calculation. This limits their feasibility in time-pressed clinics.
The other measure proposed in PsA is the Disease Activity in Psoriatic Arthritis (DAPSA).12 This includes a 68/66 joint count, patient pain and patient global disease activity VAS and a C reactive protein. They are simply added up allowing easy calculation. This measure represents a significant advantage over the DAS28 as it includes a full 68/66 joint count, which is necessary in PsA to accurately identify arthritis activity.13 Potential response measures for the DAPSA were developed in the GRAPPA paper above, and there has also been a recent publication looking at separate cut-offs for disease activity levels and response.14 Unfortunately, while this measure is feasible to perform and easy to calculate in clinic, it only assesses articular disease and thus provides a limited assessment of psoriatic disease manifestations. This could be used as a target for treatment for articular involvement specifically but ideally should be combined with measures of other domains (enthesitis, skin disease and axial involvement) to ensure that all aspects of the disease are well treated. The time advantage offered may be lost when these additional measures of skin, enthesitis, dactylitis and axial involvement are added.
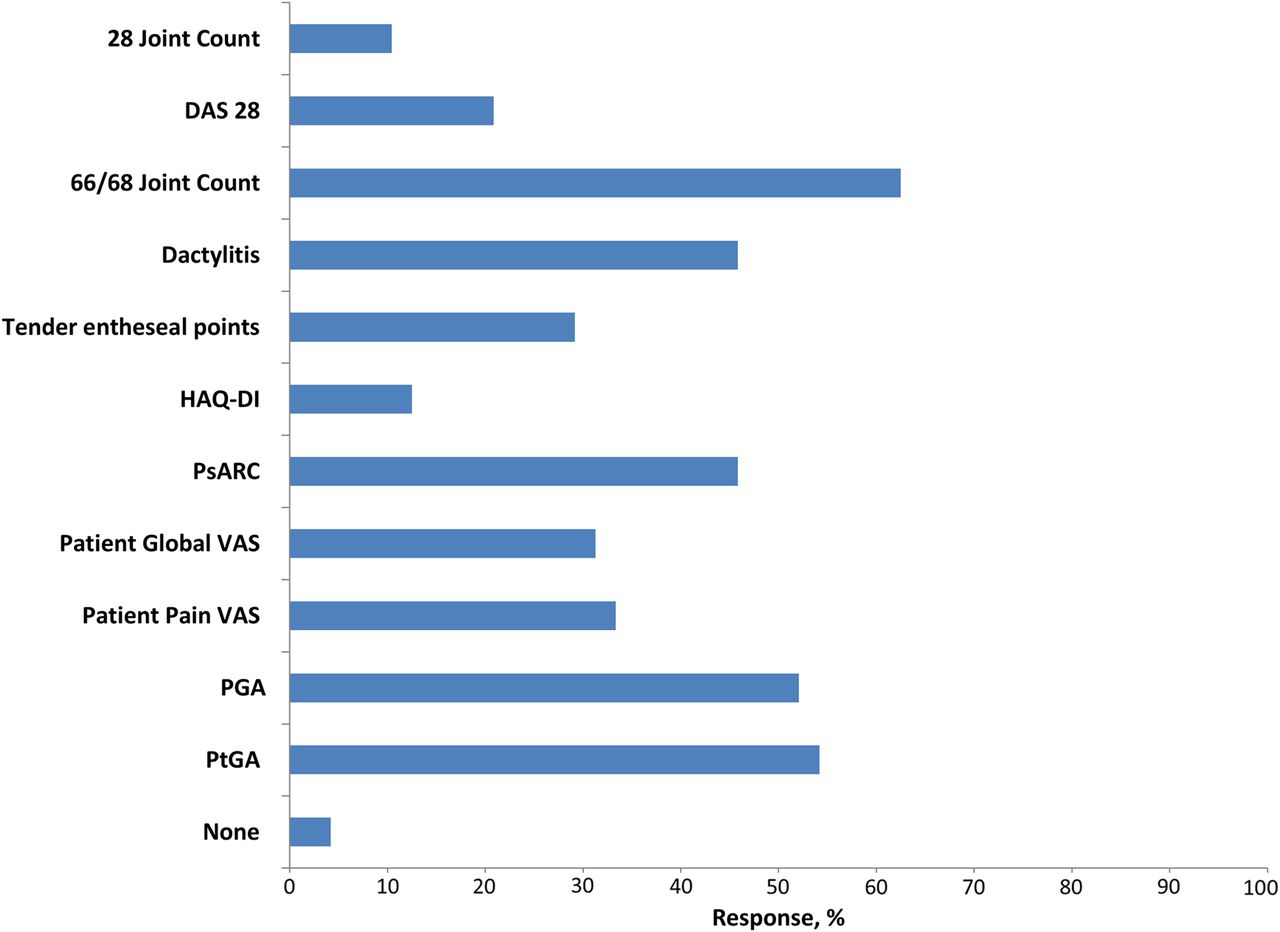
Despite the proliferation of new PsA-specific outcome measures and the push for a T2T approach in the EULAR recommendations, we know anecdotally that this is not routinely performed. Despite the relative simplicity and brevity of the MDA criteria, many people regard this as a research tool and impractical to use in a normal clinic setting. How far are we at the moment from measuring multiple outcomes and adopting a T2T strategy? A recent survey in the UK has provided a glimpse of the current practice (figure 1) (Helliwell and Kirkham, unpublished data). Fifty-six respondents (mainly consultant rheumatologists) participated. The majority (82%) used a 66/68 swollen joint count, and over 60% usually made some form of global assessment of skin disease. Only 14% of respondents currently adopted a T2T philosophy.15

{kind=link}
Disease activity and response measures performed routinely in clinic in the UK. (DAS, disease activity score; HAQ-DI, health assessment questionnaire disability index; PGA, physician global assessment; PsARC, psoriatic arthritis response criteria; PtGA, patient global assessment; VAS, visual analogue scale).
Given the consensus for moving toward a T2T strategy in PsA, how can this be implemented into routine practice? The first important step in clinics is to ensure that all PsA domains are considered and assessed using validated instruments. While the DAS28 is routinely used for assessment and T2T in patients with RA, it is not appropriate in PsA. Articular disease should be assessed using a 68/66 joint count as reduced joint counts designed for RA miss significant disease activity.13 It is also important to note that the cut-offs for remission and low disease activity for the DAS28 were developed and validated in patients with RA and are not validated for use in PsA. Physicians should also consider assessing dactylitis, enthesitis and axial involvement. The skin is also important to rheumatologists as important systemic treatment decisions will require at least a considered opinion of this domain. We are not suggesting that every rheumatologist should make a detailed assessment of the skin but that the skin should be examined for extent and severity.
If rheumatologists can implement a simple assessment of these key domains in their clinic routinely, this should facilitate a move towards using a feasible composite measure, such as MDA, or the GRAPPA indices. Currently, the MDA criteria represent the best compromise between a comprehensive measure of psoriatic disease and feasibility for inclusion in clinical practice. Achievement of the criteria has already been shown to predict less short-term clinical and radiographic progression16,17 and have also recently been shown to be associated with better 5-year outcomes in terms of radiographic damage and functional ability.18 They are the only measure used to date in a study of a T2T approach (in the TICOPA trial), and this study confirmed a significant improvement in articular, skin and patient-reported outcomes. They should be achievable within a consultation taking around 5–10 min for the physician assessment. Once these measures are recorded, it is a relatively small step to use them in a T2T approach.
In terms of the research agenda, further work is required to select the optimal measure for use as a treatment target in PsA. Further strategy trials are required in subgroups of PsA to confirm the performance of existing outcome measures across different presentations and critically which therapies should be used within the T2T approach. As T2T becomes a reality in daily practice, it will be important to evaluate a real-life clinic implementation of a T2T strategy to assess cost-effectiveness.
Acknowledgments
The authors wish to thank the following people for their contribution in acquiring the data for the figure: E Korendowych, N McHugh, S Abraham, P Ho, W Tillett.
References
Footnotes
Handling editor Tore K Kvien
Contributors LCC and PSH conceived the article, drafted it and approved the final version.
Funding Institute for Health Research (Clinical Lecturer funding).
Competing interests LCC has received consultancies, speaking fees and honoraria <US$10 000 from Abbvie, UCB, Pfizer, Boehringer Ingelheim, MSD, Celgene, Janssen, Novartis, Lilly and SunPharma. PSH has received consultancies, speaking fees and honoraria <US$10 000 from Abbvie, Pfizer, Amgen, Novartis, Janssen.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Unpublished data are available on request from the corresponding author.