Article Text

Abstract
Objective Type 2 innate lymphoid cells (ILC2s), a recently identified population of lymphoid cells lacking lineage-specific receptors, promote type 2 immunity and tissue remodelling. However, the contributive role of ILC2s in the pathogenesis of systemic sclerosis (SSc) is unknown. We aimed to evaluate the levels and correlations with fibrotic manifestations in SSc.
Methods 69 patients with SSc and 47 healthy controls were included. Blood samples and skin sections were analysed by flow cytometry and immunohistochemically by staining two complementary panels of markers.
Results Dermal and circulating ILC2s were significantly elevated in patients with SSc compared with controls. Dermal, but not circulating ILC2s were activated. Stratification of the SSc population in patients with limited cutaneous SSc (lcSSc) and diffuse cutaneous SSc (dcSSc) demonstrated increased levels of ILC2s in both subgroups with significantly higher frequencies in dcSSc compared with lcSSc. Moreover, dermal and circulating ILC2 counts correlated closely with the modified Rodnan skin score and with the presence of pulmonary fibrosis.
Conclusions ILC2 counts are elevated in patients with SSc and correlate with the extent of skin fibrosis and the presence of interstitial lung disease providing compelling evidence for profibrotic effect of ILC2s in SSc.
- Systemic Sclerosis
- Pulmonary Fibrosis
- Autoimmune Diseases
- Fibroblasts
Statistics from Altmetric.com
Introduction
Tissue fibrosis affecting the skin, but also internal organs such as the lungs, is the major hallmark of systemic sclerosis (SSc).1 ,2 The accumulation of extracellular matrix components disrupts the physiological tissue structure and leads to organ dysfunction, high morbidity and increased mortality of affected patients. However, the mechanisms in this fundamentally important process of tissue injury are incompletely understood. A growing body of evidence suggests that overproduction of extracellular matrix components results from complex interactions between various cells, including leucocytes and fibroblasts.3 ,4 More recently, locally accumulating innate-like lymphoid cells (ILCs) are emerging as an important cellular source of cytokines triggering fibrotic tissue remodelling independently of the adaptive immune system.5 ,6
ILCs are characterised by the absence of conventional lineage markers.7 ,8 Similar to T cells, they are categorised into three groups, according to distinct pattern of cytokine production and the requirement of specific transcription factors guiding their development and function.9 ,10
The type 2 cytokines interleukin (IL)-25 and IL-33 are implicated in the generation of IL-13-expressing type 2 innate lymphoid cells (ILC2s). In the mouse model of carbontetrachloride (CCl4)-induced liver fibrosis, ILC2s activated via ST2-dependent signalling are a major source of the profibrotic cytokine IL-13.5 Moreover, inhibition of ILC2 development dampens collagen deposition following injection of Schistosoma mansoni eggs.6 Besides the absence of conventional lineage markers, ILC2s express several characteristic receptors such as the inducible T cell costimulator (ICOS), the coinhibitory receptor killer-cell lectin-like receptor G1 (KLRG1) and the cytokine receptors IL-25 (IL17RB) and IL-33 (T1/ST2).11–15
Here, we identified increased frequencies of ILC2s in skin sections and in the circulation of patients with SSc compared with healthy controls (HC), suggesting that ILC2s may trigger fibroblast activation and tissue fibrosis. Furthermore, ILC2 numbers in the skin and the blood correlated with the extent of fibrosis in patients with SSc.
Materials and methods
Patient characteristics and materials and methods are available in the online supplementary material.
Results
ILC2 numbers are elevated in the skin of patients with SSc
As no single marker can sufficiently distinguish ILC2s from other cell population, we used two established sets of ILC2 markers to quantify ILC2s in the skin of patients with SSc and healthy individuals. Using the definition of ILC2s as ICOS+; ST2+; CD3–; CD11b– cells, we observed a 10-fold increase in ILC2s in skin sections of patients with SSc (median 4.78; IQR 2.03–11.24) compared with HC (median 0.48; IQR 0–1.91; p=0.0003) (figure 1A). Elevated ILC2 counts in the skin of patients with SSc were confirmed using an independent second panel of positive and negative markers of ILC2s. Consistent with the results obtained with the first panel of ILC2 markers, also the characterisation as ST2+; IL-17RB+; KLRG1+; Lin– (CD3, CD14, CD16, CD19, CD20 and CD56) cells showed an increase in ILC2s by 3.8-fold in patients with SSc (median 4.03; IQR 1.91–16.12) compared with HC (median 1.06; IQR 0.32–1.27) (figure 1B). Autofluorescent mast cells and erythrocytes were excluded from analysis by toluidine-blue and nuclear (4′,6-Diamidin-2-phenylindol; DAPI) staining (see online supplementary figure S1A–C).
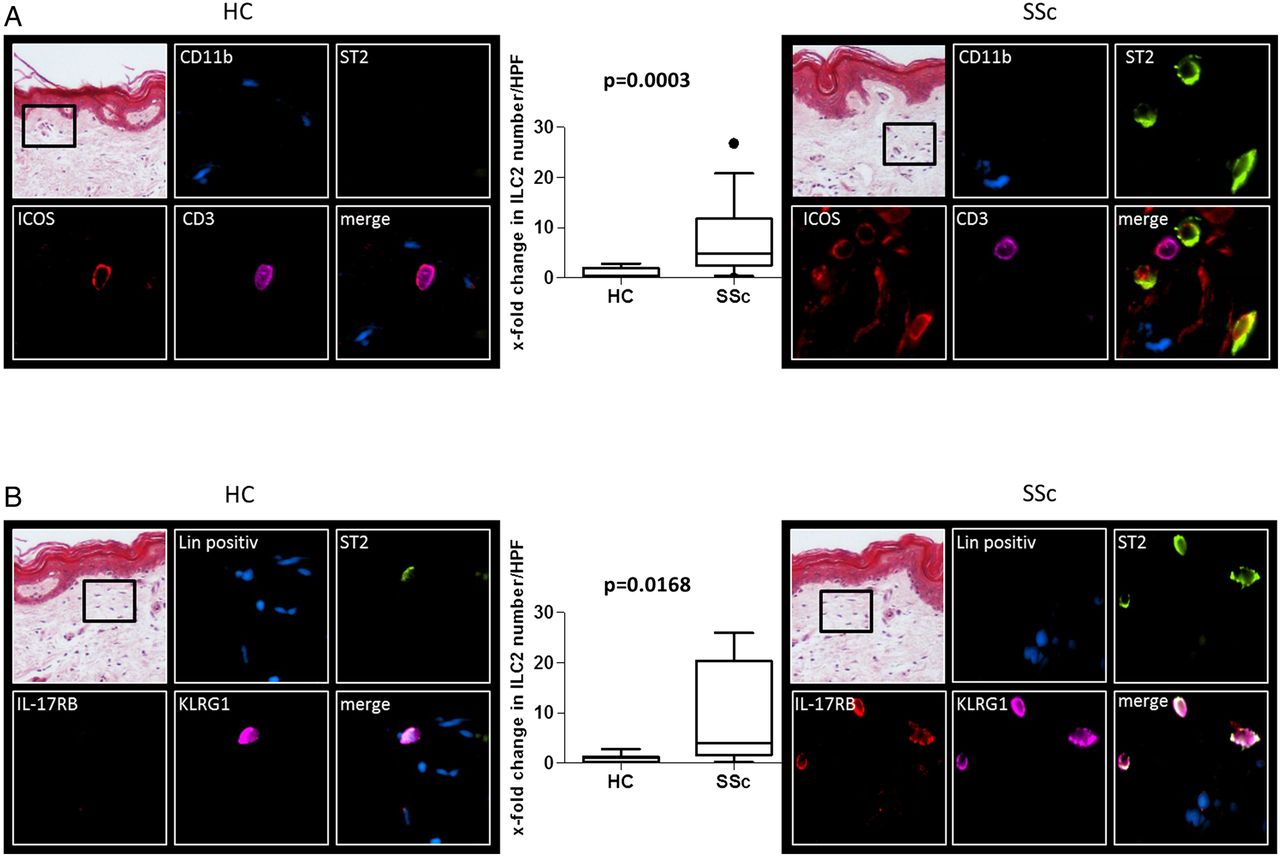
The number of type 2 innate lymphoid cells (ILC2s) is elevated in the skin of patients with systemic sclerosis (SSc) compared with healthy controls (HC). (A) Representative images and quantification of H&E and immunofluorescence staining for ILC2s in the skin of patients with SSc (n=33) and healthy volunteers (n=11) using ST2 and ICOS as positive markers and CD11b and CD3 as negative markers for ILC2s. (B) Representative images (HC: n=7; SSc: n=9) and quantification of H&E and immunofluorescence staining for ILC2s using a complementary panel of markers with ST2, interleukin (IL)-17RB and killer-cell lectin-like receptor G1 (KLRG1) as positive markers and lineage markers consisting of CD3, CD14, CD16, CD19, CD20 and CD56 as negative markers. Representative images are shown at a 100-fold (H&E) or 600-fold (immunofluorescence) magnification. All data are shown as box plots with 5% and 95% centiles. HPF, high power field.
Increased ILC2 numbers in the skin of patients with SSc are associated with fibrotic manifestations
We next analysed potential associations of ILC2 numbers with clinical manifestations in patients with SSc. We stratified the SSc population in patients with limited cutaneous SSc (lcSSc) and diffuse cutaneous SSc (dcSSc). Although the number of ILC2s in the skin was increased in both subgroups of patients with SSc compared with healthy individuals, ILC2 numbers were significantly higher in patients with dcSSc than in patients with lcSSc (figure 2A). We grouped patients with SSc into patients with restricted and extensive skin fibrosis and found that patients with a modified Rodnan skin score (mRSS) >10 have higher ILC2 numbers in the skin compared with patients with SSc with an mRSS ≤10 (figure 2B). Moreover, dermal ILC2 counts correlated with the mRSS (figure 2C). Further characterisation of ILC2s revealed homogeneous expression of thymic stromal lymphopoietin protein (TSLP) receptor and IL-17RB in dermal, but not in circulating ILC2s, suggesting activation of ILC2s in the skin of patients with SSc (figure 2D, see online supplementary figure S4B). The majority of dermal ILC2s also express cutaneous lymphocyte antigen (CLA), suggesting putative skin homing of ILC2s in patients with SSc (see online supplementary figure S4A).

Type 2 innate lymphoid cell (ILC2) counts in the skin correlate with the fibrotic burden in patients with systemic sclerosis (SSc). (A) Numbers of ILC2s in skin sections of healthy controls (HC) and of patients with limited cutaneous SSc (lcSSc) and diffuse cutaneous SSc (dcSSc). (B) ILC2 counts in skin sections of HC and patients with SSc with an modified Rodnan skin score (mRSS) >10 compared with patients with SSc with an mRSS≤10. (C) Correlation between ILC2 numbers in the skin and the mRSS. Data are shown as median and IQR. (D) Representative images of H&E and immunofluorescence staining for ILC2s in the skin of patients with SSc (n=5) using ILC2 activation markers TSLPR, interleukin (IL)-17RB and ST2 as positive markers and Lin (CD3, CD14, CD16, CD19, CD20 and CD56) as negative markers for ILC2s. HPF, high power field. *0.05 > p ≥ 0.01; **0.01 > p ≥ 0.001; ***p<0.001.
The number of circulating ILC2s is increased in patients with SSc and correlates with the extent of skin fibrosis and the presence of interstitial lung disease
As access to skin biopsies in clinical routine is limited, we analysed whether ILC2 counts may also be correlated with fibrotic manifestations in patients with SSc. Indeed, frequencies and absolute numbers of CD45+; ST2+; ICOS+; Lin– (CD3, CD14, CD16, CD19, CD20 and CD56) ILC2s were elevated in the blood of patients with SSc compared with controls (figure 3A, see online supplementary figures S2A and S3C). Consistently, the characterisation as CD45+; CRTH2+; IL-7Rα+; Lin– (CD3, CD14, CD16, CD19, CD20 and CD56) cells also showed significantly elevated circulating ILC2 counts in patients with SSc compared with HC (see online supplementary figures S2B and S3B, D). As for ILC2s in the skin, ILC2 numbers in the blood were higher in patients with dcSSc, and in patients with an mRSS of >10 compared with patients with lcSSc and mRSS of ≤10, respectively (figure. 3B,C). Circulating ILC2 counts also correlated closely with the mRSS (R2=0.44; p<0.0001; online supplementary figure S5A). Moreover, patients with SSc with pulmonary fibrosis had increased ILC2 numbers in peripheral blood compared with patients with SSc without interstitial lung disease (ILD) (figure 3D). Notably, ILC2 counts were highest in patients with extensive lung involvement assessed by CT scan (see online supplementary figure S5B). A comparison of circulating ILC2 frequencies between different cohorts of patients with rheumatoid arthritis,16 systemic lupus erythematosus17 and SSc demonstrated strong upregulation of ILC2s only in patients with SSc (see online supplementary figure S3A). Together, these data demonstrate that not only ILC2 numbers in tissue, but also in the blood are correlated with fibrotic manifestations in SSc.

{kind=link}
{kind=link}
{kind=link}
The number of circulating type 2 innate lymphoid cells (ILC2s) is increased in patients with systemic sclerosis (SSc) and correlates with the extent of skin fibrosis. (A) ILC2 counts in the blood of patients with SSc and healthy controls (HC). (B) Numbers of ILC2s in the blood of patients with limited cutaneous SSc (lcSSc) and diffuse cutaneous SSc (dcSSc). (C) Circulating ILC2 counts of HC and patients with SSc with an modified Rodnan skin score (mRSS) >10 compared with patients with SSc with an mRSS ≤10. (D) Number of circulating ILC2s in HC and patients with SSc with and without pulmonary fibrosis. All data are shown as median and IQR.
Multivariate analysis of clinical parameters and ILC2 numbers in patients with SSc
Next, we calculated a multivariate linear regression model with three associated clinical parameters (lcSSc vs dcSSc; mRSS; the presence of pulmonary fibrosis) of our cross-sectional cohort to predict ILC2 numbers in a stepwise forward model and a stepwise backward model. Sex and age were also incorporated into the regression analysis as possible confounders. The best forward selection method led to a model consisting of the extent of skin fibrosis defined by dcSSc (β=0.704; p<0.001) and the presence of pulmonary fibrosis (β=0.327; p=0.005). The backward selection method led to the same model, thereby demonstrating the robustness of this data set. The correlation coefficient (R=0.885) results in a coefficient of determination (R2) of 0.764. Thus, the results from our cross-sectional cohort demonstrate that in patients with SSc as much as 76% of the variability of the ILC2 numbers can be explained by a combination of the extent of skin fibrosis and the presence of pulmonary fibrosis; however, as skin and lung fibrosis are dynamic variables over time, follow-up studies are necessary to evaluate ILC2s as predictors of fibrotic activity.
Discussion
Herein, we provide first evidence for a role of ILC2s in the pathogenesis of rheumatic diseases by demonstrating increased ILC2 numbers in patients with SSc. Our data are indirectly supported by findings of increased ILC2 counts in animal models of fibrotic diseases such as CCl4-induced liver fibrosis and S. mansoni-induced pulmonary fibrosis.5 ,6 In contrast to sophisticated studies in mice, data on ILC2s in humans are mainly limited to allergic diseases and largely focus on circulating ILC2s.18
Higher numbers of ILC2s in the skin as well as in the blood were both associated with more extensive skin fibrosis as shown by increased ILC2 numbers in patients with SSc with (i) dcSSc versus lcSSc, (ii) patients with high mRSS versus patients with low mRSS and (iii) a highly significant correlation of dermal and circulating ILC2 counts with the mRSS. In addition, patients with SSc with pulmonary fibrosis had significantly increased ILC2 counts in peripheral blood as well as in the skin (data not shown). The coexpression of skin-homing marker CLA and activation markers TSLPR and IL-17RB on skin resident in contrast to circulating ILC2s suggests that ILC2s are activated locally in the skin.15–17 The highly significant correlations of ILC2 counts with the extent and severity of dermal and pulmonary fibrosis encourage follow-up studies to further evaluate the potential of ILC2s as biomarkers for fibrosis in patients with SSc. However, to serve as a biomarker, our findings need to be confirmed in independent, larger cohorts of patients with SSc with sufficient power to detect correlations with other, rarer fibrotic manifestations and the sensitivity of ILC2 counts to change over time needs to be further evaluated. The association of increased numbers of ILC2s in patients with SSc with fibrotic manifestations also warrants mechanistic studies to elucidate the molecular mechanisms by which ILC2s may promote fibrosis and to characterise the potential of targeting ILC2s as an antifibrotic approach in SSc.
Acknowledgments
We thank Regina Kleinlein, Christina Weiss and Monica Pascual for excellent technical assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figures
Footnotes
Handling editor Tore K Kvien
JHWD and AR contributed equally.
Contributors Design of the study: TW, JHWD, AR. Acquisition of data: TW, SU, SW, AR. Interpretation of data: TW, ME, CD, CB, OD, GS, JHWD, AR. Manuscript preparation: TW, ME, CD, OD, GS, JHWD, AR. Provided patient samples: CB, KG, OD, JHWD, AR.
Funding Grants DI 1537/5-1, DI 1537/7-1, DI 1537/8-1, DI 1537/9-1, AK 144/1-1, RA 2506/3-1 and SCHE 1583/7-1 of the Deutsche Forschungsgesellschaft, Else Kröner-Fresenius-Stiftung 2014_A184, grants A57 and J40 of the Interdisciplinary Center for Clinical Research Erlangen (IZKF), the ELAN-Program of the University of Erlangen-Nuremberg and the Career Support Award of Medicine of the Ernst Jung Foundation.
Competing interests OD has consulted for, or has received research funding from, 4D Science, Actelion, Active Biotec, Bayer-Schering, Biogen, Biovitrium, BMS, Boehringer, EpiPharm, Ergonex, GSK, Inventiva, Medac, Novartis, Pfizer, Roche/Genentech, Sanofi/Genzyme, Serodapharm, Sinoxa and United BioSource Corporation; JHWD has consultancy relationships and/or has received research funding from Actelion, BMS, Celgene, Bayer Pharma, Boehringer Ingelheim, JB Therapeutics, Sanofi-Aventis, Novartis, UCB, GSK, Array Biopharma and Active Biotech in the area of potential treatments of SSc and is stock owner of 4D Science GmbH.
Ethics approval University of Erlangen-Nuremberg.
Provenance and peer review Not commissioned; externally peer reviewed.