Article Text

Abstract
Objective To investigate the incidence and risk of ischaemic heart disease (IHD) and acute myocardial infarction (AMI), including the role of non-steroidal anti-inflammatory drugs (NSAID), in patients with ankylosing spondylitis (AS) compared with population controls.
Methods All patients with newly diagnosed AS (n=3809) from the British Clinical Practice Research Datalink (1987–2012) were matched with up to seven persons without AS by year of birth, gender and practice (n=26 197). Incidence rate ratios (IRR) and HRs for development of IHD and AMI were calculated. Stepwise analyses were performed adjusting for age, gender, comorbidity and drug use, including NSAIDs.
Results At baseline, 4.3% of the patients had IHD and 1.8% had AMI compared with 3.4% and 1.4% of the controls, respectively. After exclusion of pre-existing IHD or AMI, the IRRs were 1.18 (95% CI 0.96 to 1.46) and 0.91 (95% CI 0.65 to 1.27) for IHD and AMI, respectively. Compared with controls, the age-gender adjusted HR for developing IHD was 1.20 (95% CI 0.97 to 1.48), and for AMI 0.91 (95% CI 0.65 to 1.28). In female patients, the risk of developing IHD was increased (HR 1.88, 95% CI 1.22 to 2.90), but after adjustment for all possible risk factors only a non-significant trend was found (HR 1.31, 95% CI 0.83 to 2.08). In particular, NSAID use explained this change (HR IHD adjusted for age-gender-NSAID use 1.57, 95% CI 0.99 to 2.48).
Conclusions Female patients with AS had an increased age-adjusted risk of developing IHD, but after adjustment for NSAID use only a non-significant trend towards increased risk was found.
Statistics from Altmetric.com
Introduction
Ischaemic heart disease (IHD) is one of the leading causes of death and loss of quality of life worldwide.1 In the last few decades, an excess in cardiovascular (CV) morbidity and mortality in patients with chronic inflammatory rheumatic disease, such as rheumatoid arthritis (RA) has been demonstrated.2 ,3 This led to additional recommendations for CV risk assessment4 and treatment guidelines to manage the CV risk in RA.5 In ankylosing spondylitis (AS) conflicting results on the risk of CV disease have been reported.6 An increased risk of IHD in AS was found in three studies.7–9 Also, a statistically significantly increased risk for acute myocardial infarction (AMI) in AS was reported in some studies,10–12 whereas, others failed to demonstrate this.7 ,13 ,14 Differences in selection of populations or a flawed study design may have contributed to the contradictory results.15
Several aetiological mechanisms could be associated with the increased CV risk in AS. First, the systemic inflammation, which is a part of the pathophysiology of AS, may play an independent role in the onset of atherosclerosis.6 Second, several studies have shown an increased prevalence of conventional risk factors in AS, including the metabolic syndrome and decreased levels of high density lipoprotein cholesterol.6 ,11 Third, the long-term use of non-steroidal anti-inflammatory drugs (NSAID) may accelerate the atherosclerotic process.6 ,16 NSAIDs are the cornerstone of the treatment of AS and are often prescribed on a long-term basis. According to a recent evaluation of all available evidence by the European Medicines Agency, NSAIDs, as a class, are associated with a small increased risk of atherosclerosis or atherothrombotic events, particularly in patients with underlying heart or circulatory conditions, or with certain CV risk factors.17 Moreover, high-dose or long-term NSAID use may increase this risk.18 Differences among the several types of NSAIDs with respect to the CV risk have been reported.17 ,19
To date, there are still some unsolved epidemiological issues on the CV risk of patients with AS. Studies comparing the CV risk in patients with AS with population-based controls are limited or had a flawed study design. Also, studies including adjustments for other potential risk factors besides age and gender when analysing the risk of CV disease in AS, are scarce. Furthermore, the role of NSAID use in the aetiology of AS-associated IHD has, to our knowledge, never been assessed. Therefore, the objective of the present study was to investigate the risk of a first event of IHD, including AMI, in patients with AS compared with population-based controls, and the role of NSAID use in this.
Methods
Design and data source
A retrospective cohort study was conducted using data from the Clinical Practice Research Datalink GOLD (CPRD), formerly known as the General Practice Research Database. CPRD contains computerised medical records of over 10 million patients under care of general practitioners (GP) in the UK. Since 1987, data are prospectively recorded, and include patient demographics, prescription details, clinical events, preventive care provided, specialist referrals, hospital admissions and their major outcomes. Read codes classify diseases and symptoms. Practices only contribute to CPRD when their data quality is up to research standards. CPRD has been extensively validated.20
Study population
The study population consisted of all patients aged 16 years or older with at least one recording of AS during the period of CPRD data collection, which started for the present study in January 1987 and ended in December 2012. The start of valid data collection of each patient was defined as the date at which the practice was included into CPRD, the GP's dataset was approved as ‘up-to-standard’, and the patient moved into the practice. Patients with a first-ever diagnosis of AS were matched by year of birth, gender, calendar time and practice to up to seven control subjects without a diagnosis of AS at any time during their registration period. The date of the first record of AS defined the index date. Control patients were assigned the same index date as their matched case. The subjects in the study population were followed from their index date to the outcome of interest, the end of data collection, the date of transfer out of the practice area or death, whichever came first. Patients and controls with a record for another inflammatory rheumatic disease (RA, psoriatic arthritis, systemic lupus erythematous or vasculitis) any time during the enrolment were excluded from the current analysis.
Study outcome and risk factors
Outcomes of interest were a first event of IHD or AMI, specified by read codes. IHD was defined as all types of IHD, and included, for example, AMI, coronary artery bypass surgery and percutaneous coronary intervention. The total follow-up time was divided into 30-day intervals in order to adjust the analyses for the influence of potential confounders in a time-varying way. The computerised medical records before the start of each interval were reviewed for the occurrence of potential confounders. Baseline confounders considered included gender, body mass index (BMI), smoking status and alcohol use (the later three as dummy variables). The following time-varying confounders were considered: age, hypercholesterolaemia (including familial hypercholesterolaemia), a history of acute or chronic renal failure, as well as a prescription of antihypertensives, antidiabetics, antiplatelet agents, statins and asthma medication 6 months before the start of an interval. Exposure to NSAIDs was determined as the average defined daily doses (DDD) equivalent to 100 mg of diclofenac, based on WHO norms prior to the start of an interval.21 NSAIDs were further categorised into cyclo-oxygenase-2 (COX-2) inhibitors, naproxen or other traditional NSAIDs 3 months prior the start of an interval (binary), because of the possible different impact on the risk of IHD or AMI.17
Statistical analysis
Dichotomous baseline characteristics (excluding gender and age) of patients and controls were compared using χ2 tests. Stratified analyses for gender were done with respect to a history of IHD and AMI before the index date. After excluding patients with pre-existing IHD or AMI, incidence rates (IR) for IHD and AMI were calculated for patients (and their controls), respectively, and were estimated as the number of subjects with the event per 1000 person-years (pys). pys Were computed by adding all person-time from the index date to either the date of the first event or to the date of censoring if the event did not occur. Incidence rate ratios (IRR) were calculated by dividing the IR for patients by the IR for controls. IRRs were stratified based on gender and age categories (16–39, 40–49, 50–59, 60–69, 70–79 and ≥80 years). The overall prevalence of IHD and AMI was estimated using Kaplan–Meier methods, and also included patients (and controls, respectively) with an event at baseline. Furthermore, the attributable risk per 1000 pys was calculated for IHD and AMI.
The risk of developing a first IHD or AMI after the index date was estimated by HRs using time-dependent Cox proportional hazard models for those patients (and controls) without the outcome of interest before the index date. Three step-wise models were created with adjustment for potential confounders: (1) adjustment for age and gender, (2) adjustment for age, gender and the DDD of NSAID use, (3) adjustment for age, gender, DDD of NSAID use, and all confounders that changed the β coefficient of the HR more than 1% in the age-gender adjusted analysis. Stratified analyses were done for gender.
In a separate analysis, the role of NSAIDs in the risk of IHD was evaluated. For this, all patients were stratified according to the recent use of any NSAIDs, naproxen, COX-2 inhibitors or other traditional NSAIDs. HRs were calculated, in which patients were compared with controls, irrespective of their NSAID use. Additionally, patients with a history of NSAID use were compared with patients without a history of the same class of NSAIDs, using the Wald test. This analysis was also stratified for gender. All statistical analyses were conducted using SAS V.9.1.
Results
Baseline results
Baseline characteristics of patients with AS (n=3809) and their matched controls (n=26197, 92% had seven controls) are presented in table 1. The mean duration of follow-up for patients and controls was 6.6 years. At baseline, patients were more likely to have been diagnosed with IHD (4.3% vs 3.4%) or AMI (1.8% vs 1.4%) compared with controls (table 1). In the stratified analyses, male patients were more likely to have been diagnosed with IHD (3.4% vs 2.8%, p=0.04) and AMI (1.7% vs 1.2%, p=0.01) compared with male controls, and female patients were more likely to have been diagnosed with IHD (0.9% vs 0.6%, p=0.04), but not with AMI (0.1% vs 0.1%, p=0.06) compared with female controls. Within the AS population, male patients had, more often, a history of IHD (p=0.01) and AMI (p<0.01) compared with female patients.
Baseline characteristics of patients with ankylosing spondylitis (AS) and controls
Incidence and overall prevalence of IHD and AMI
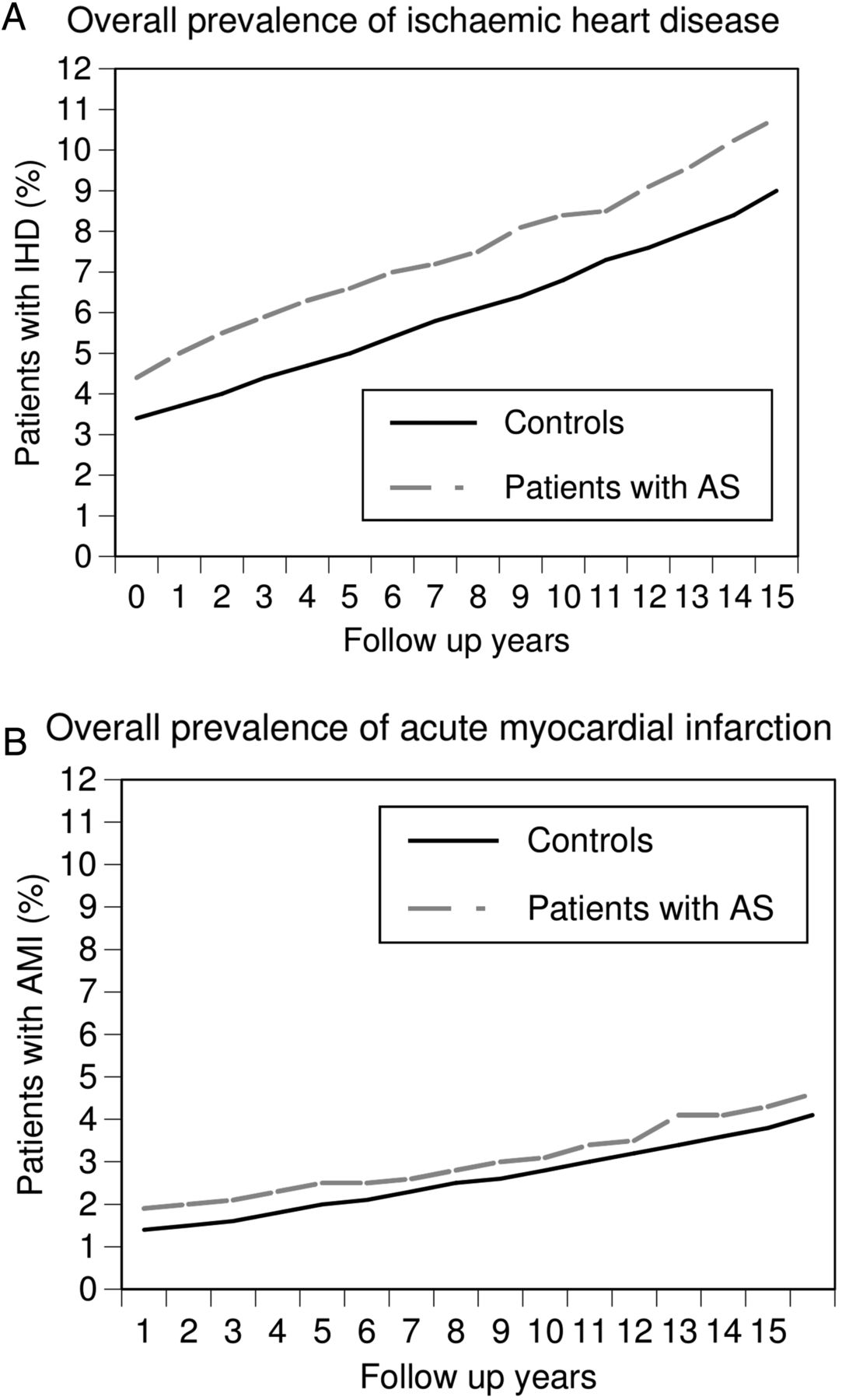
In table 2, a trend towards a higher incidence of developing a first IHD event in patients compared with controls (IRR 1.18, 95% CI 0.96 to 1.46) is shown. In particular, the IRR of IHD was increased among female patients versus female controls (IRR 1.72, 95% CI 1.12 to 2.64), whereas, male patients were not at increased risk of IHD (IRR 1.07, 95% CI 0.84 to 1.37). The IRR of developing a first AMI event was not increased in patients versus controls (IRR 0.91, 95% CI 0.65 to 1.27). Figure 1 visualises the overall prevalence of IHD and AMI over time compared with controls, including events prior to baseline. At baseline, differences in the prevalence of IHD and AMI between patients and controls were found, which remained unchanged during follow-up. The overall prevalence of IHD was 10.8% in patients and 9.0% in controls, after 15 years of follow-up. The overall prevalence of AMI was 4.6% in patients and 4.1% in controls, after 15 years of follow-up. The attributable risk of AS for developing IHD was 0.7 per 1000 pys and for developing an AMI −0.2 per 1000 pys.
Incidence rates of ischaemic heart disease and acute myocardial infarction in patients with ankylosing spondylitis (AS) and controls
{kind=link}
Visualisation of the overall prevalence over time, including baseline values, of IHD and AMI in patients with AS and controls. (A) IHD; (B) AMI. For the calculation of the overall prevalence over time, also the patients (controls) are included with an event at baseline. AMI, acute myocardial infarction; IHD, ischaemic heart disease; AS, ankylosing spondylitis.
Risk of developing a first event of IHD or AMI
Table 3 shows that the risk of IHD or AMI was similar among patients with AS and controls. Female patients with AS had a 1.9-fold age-gender adjusted risk of IHD (HR 1.88, 95% CI 1.22 to 2.90), but it was no longer significantly increased after adjustment for the DDD of NSAIDs use (age-gender adjusted HR1.57, 95% CI 0.99 to 2.48). Additionally, table 4 shows that the risk of IHD in patients with AS was 1.4-fold increased with recent use of NSAIDs (fully adjusted HR 1.36, 95% CI 1.00 to 1.85), and 3.0-fold increased with recent use of COX-2 inhibitors (fully adjusted HR 3.03, 95% CI 1.61 to 5.69) compared with all controls irrespective of their NSAID use. Moreover, patients with AS using COX-2 inhibitors had an increased risk of IHD compared with patients who did not use this drug (data not shown).
Risk of ischaemic heart disease and acute myocardial infarction in patients with AS compared with controls
Risk of ischaemic heart disease stratified by NSAID exposure in patients with AS compared with controls
Discussion
The present study investigated the incidence and risk of IHD and AMI, including the role of NSAIDs, in patients with AS compared with population-based matched controls. While the incidence of IHD was not increased in male patients, a significant increase was found in female patients compared with controls. After adjustment for NSAIDs use, however, only a non-significant trend towards increased risk of IHD in female patients was found. Recent use of NSAIDs and, in particular COX-2 inhibitors, resulted in a 1.4-fold and 3.0-fold fully adjusted overall risk of IHD in patients with AS compared with controls. An increased risk of AMI could not be demonstrated, and no gender differences were found.
In the literature, an increased risk of IHD in patients with AS has been reported earlier. Claims data from the Canadian province, Quebec, showed increased IHD risks in 4836 male patients of all age categories (prevalence ratio ranging from 1.17 to 1.75) and in 3169 female patients younger than 60 years of age (prevalence ratio ranging from 1.54 to 1.97), but not in 701 female patients older than 60 years (prevalence ratio 1.08, 95% CI 0.99 to 1.17) compared with a general population cohort.9 Two other population-based studies, not stratified for gender, reported an increased risk of IHD in patients with AS after adjustment for age and gender (n=935, standardised morbidity ratio 2.20, 95% CI 1.27 to 2.707), and after adjustment for hypertension and hyperlipidaemia only (n=4794, HR 1.47 95% CI 1.13 to 1.92).16 Various explanations can be found for the differences between reported risks and our results. Although sample sizes were large and comparable, our study included only newly diagnosed patients with AS, whereas, other studies included both prevalent and incident patients. At baseline, we found a higher prevalence of IHD in patients with AS compared with controls, which is in line with a cross-sectional study, which also found a 1.5 higher relative risk (95% CI 1.0 to 1.5) of IHD in patients with AS compared with matched controls.8 Furthermore, in contrast with other studies, we were able to statistically adjust for a wide range of confounders, including the use of NSAIDs. In this study, we demonstrated that use of NSAIDs explained a substantial proportion of the association between AS and risk of IHD. Our results are in line with the growing evidence that also COX-2 inhibitors may increase the risk of IHD.6 ,22 In general, NSAIDs inhibit the activity of both COX-1 (thromboxane; thrombogenic and arthrogenic) and COX-2 activity (prostacyclin; opposes thromboxane). A COX-2 inhibitor-associated disruption of this balance might increase the risk of atherosclerosis, thrombogenesis and CV complications.22
A broad definition of IHD was used in this study and consisted of several of ischaemic heart conditions and symptoms, among which is angina pectoris. It is possible that misdiagnosis has occurred, because chest pain may also be caused by other conditions. Therefore, a more ‘reliable’ measure for IHD, that is, AMI, which was diagnosed on objective findings on electrocardiogram and blood abnormalities, was investigated. Earlier studies reported conflicting results with respect to the risk of AMI in AS. Two population-based studies with, respectively, 935 and 1686 patients with AS, failed to demonstrate an increased risk of developing AMI,7 ,14 which is similar to our results. By contrast, a cross-sectional survey from The Netherlands among 383 patients with AS (age 50–75 years) under the care of a rheumatologist reported a 3.1-fold increased risk of AMI (95% CI 1.89 to 5.09) compared with patients selected from a general practitioner database.12 The association in this cross-sectional survey is probably largely explained by information bias due to differential recording of exposure and outcome between both cohorts: the quality of AS recording has not been validated, and there is clear evidence that AMI is substantially under-recorded.15
Interestingly, we found a difference in the IHD risk between female and male patients, but we could not show this difference for the AMI risk. A possible explanation might be that female patients suffer more from enthesitis23 and widespread (‘fibromyalgia-like’) pain24 compared with male patients, which might be misdiagnosed as IHD.
Some limitations of the present study need to be addressed. First, an association between AS and IHD or AMI may have been masked by non-differential misclassification of exposure (AS, NSAID use) or outcome (IHD, AMI). Linkage of a different regional UK GP dataset with a rheumatology registry showed that 24% of the patients with an AS diagnoses were not captured by the GP.14 We do not have information on this within CPRD. Additionally, a recent study showed a 25% under-recording rate of AMI in CPRD.25 Furthermore, information on over-the-counter use of NSAIDs was lacking, which could have resulted in misclassification of NSAID exposure, however, it is difficult to quantify the degree of misclassification. The second limitation is our operational definition of ‘incident’ patients with AS. A proportion of the patients may have suffered from AS for a longer time, either because of a delay in diagnosis, or because the first diagnostic code for AS in CPRD did not correspond with the actual diagnostic date of AS. Third, the positive associations that we have reported may also be explained by diagnostic bias. Patients with AS may have visited their healthcare provider more regularly because of their disease, and as such, IHD and AMI may have been earlier or more frequently diagnosed compared with controls. Furthermore, as described above, chest pain is a feature of AS, and may therefore be misclassified as IHD, which can also explain the different findings with the lack of association between AS and AMI. Fourth, we did not have information on patient disease characteristics including HLA-B27 status, physical activity, disease activity and prescriptions of biologicals. Inflammation might accelerate the progress of atherosclerosis, and it is uncertain whether biologicals have a beneficial effect on subclinical atherosclerosis in AS.26 Moreover, NSAID use might be a surrogate for disease activity, because patients with a higher disease activity are more likely to use NSAIDs.
The strengths of this study are the large sample size and substantial duration of follow-up. CPRD is representative for the total UK population. By contrast with most previous studies, we had a population-based comparison group which was randomly selected from CPRD. Additionally, we were the first study that could statistically adjust for a wide range of potential confounders, including smoking status, BMI, comorbidities and the use of comedications, including NSAIDs.
In conclusion, this study showed that female patients with AS seemed to be at an increased risk of developing IHD compared with female population-based controls in an age-adjusted analysis, but after adjustment for recent NSAID use there was only a trend towards increased risk. There was no increased risk of AMI in patients with AS compared with controls. Although it cannot be excluded that NSAID use is (partly) a reflection of disease activity, rheumatologists should carefully balance the beneficial effects of NSAIDs and the increased risk of IHD in patients with AS.
Acknowledgments
This study protocol (No 12_163) has been approved by the Independent Scientific Advisory Committee of the Medicine and Healthcare products Regulatory Agency.
References
Footnotes
Handling editor Tore K Kvien
Contributors IE, CS, AvT, AB and FdV were involved in the design of the study, the analysis and interpretation of data and drafting of the manuscript. MTB was involved in the analysis of the data and revising it critically for important intellectual content. MLDB was involved in revising the manuscript critically for important intellectual content. All authors read and approved the final manuscript.
Competing interests The Division of Pharmacoepidemiology & Clinical Pharmacology has received unrestricted funding from the Netherlands Organisation for Health Research and Development (ZonMW), the Dutch Health Care Insurance Board (CVZ), the Royal Dutch Pharmacists Association (KNMP), the private-public funded Top Institute Pharma (http://www.tipharma.nl), includes cofunding from universities, government and industry, the EU Innovative Medicines Initiative (IMI), the EU 7th Framework Program (FP7), the Dutch Ministry of Health and industry (including GlaxoSmithKline, Pfizer and others). AB received research grants from Amgen, Abbvie, Merck and Pfizer and occasionally honoraria from Pharma funded (UCB, Pfizer) speakers bureaus. AvT: Speaker's and consultancy fees from Abbott, MSD, UCB, Pfizer.
Patient consent Obtained.
Ethics approval Independent Scientific Advisory Committee of the Medicine and Healthcare products Regulatory Agency.
Provenance and peer review Not commissioned; externally peer reviewed.