Article Text

Abstract
Objectives In agreement with other autoimmune diseases, systemic sclerosis (SSc) is associated with a strong sex bias. However, unlike lupus, the effects of sex on disease phenotype and prognosis are poorly known. Therefore, we aimed to determine sex effects on outcomes.
Method We performed a prospective observational study using the latest 2013 data extract from the EULAR scleroderma trials and research (EUSTAR) cohort. We looked at (i) sex influence on disease characteristics at baseline and (ii) then focused on patients with at least 2 years of follow-up to estimate the effects of sex on disease progression and survival.
Results 9182 patients with SSc were available (1321 men) for the baseline analyses. In multivariate analysis, male sex was independently associated with a higher risk of diffuse cutaneous subtype (OR: 1.68, (1.45 to 1.94); p<0.001), a higher frequency of digital ulcers (OR: 1.28 (1.11 to 1.47); p<0.001) and pulmonary hypertension (OR: 3.01 (1.47 to 6.20); p<0.003). In the longitudinal analysis (n=4499), after a mean follow-up of 4.9 (±2.7) years, male sex was predictive of new onset of pulmonary hypertension (HR: 2.66 (1.32 to 5.36); p=0.006) and heart failure (HR: 2.22 (1.06 to 4.63); p=0.035). 908 deaths were recorded, male sex predicted deaths of all origins (HR: 1.48 (1.19 to 1.84); p<0.001), but did not significantly account for SSc-related deaths.
Conclusions Although more common in women, SSc appears as strikingly more severe in men. Our results obtained through the largest worldwide database demonstrate a higher risk of severe cardiovascular involvement in men. These results raise the point of including sex in the management and the decision-making process.
- Autoimmune Diseases
- Epidemiology
- Systemic Sclerosis
Statistics from Altmetric.com
Introduction
Autoimmune diseases include more than 70 different disorders, affecting over 5% of the population of the Western countries. They are a well-known cause of morbidity and mortality.1 One of the major shared features among most autoimmune diseases is the predominance of women, with >80% of affected individuals being women.1 Even though the female predisposition has been known for a long time, the mechanisms by which sex influences disease expression remain unknown. A better understanding of such effects could help towards a better stratification of the factors leading to a wide range of clinical manifestations, particularly identifying cases more likely to progress or to present severe damages and to develop novel targeted therapies and ultimately personalised medicine.1–3
Systemic sclerosis (SSc) is a complex multiorgan disease affecting the immune system, the microvascular system and the connective tissue.4 ,5 In agreement with other autoimmune diseases, SSc is associated with a strong sex bias.6 The various available worldwide cohorts usually report a female predominance with between four and nine affected women for one man.7–11 However, data about the effects of sex on disease characteristics and outcomes are scarce. The very few published data were mainly obtained in non-European patients (North American or Japanese) and revealed conflicting results regarding the impact of sex on disease severity and survival.12–17 So far, large epidemiological studies are missing, particularly in European populations. Two independent studies, each based on about 1000 European patients, suggested that male gender could be a risk factor for mortality,8 ,18 but data were provided on distinct disease manifestations. In another autoimmune disease, systemic lupus erythematosus (SLE), large prospective data have well documented that male patients have more often a severe disease and greater organ progression than female patients.19–22 Whether a similar effect occurs in SSc remains unknown. Therefore, we aimed (i) to clarify the impact of sex on SSc phenotype: time of occurrence, autoantibodies and organ involvements and (ii) to investigate the impact of sex on disease outcomes including severe damages and mortality, in a large European population. This is now made possible by the implementation of the systematic longitudinal follow-up of patients with SSc included in the EULAR scleroderma trials and research (EUSTAR) registry. Based on annual visits, on a prospective manner, this large database provides a powerful tool to investigate prognostic factors.
Methods
All data for patients registered in the EUSTAR database as of November 2013 were exported.
In all, 9182 patients, fulfilling the 2013 American College of Rheumatology/ European League Against Rheumatism (ACR/EULAR) criteria for SSc, were available for baseline analyses. We analysed the baseline and follow-up visit data using the predefined annual data collection protocol. We also looked at difference in sex bias according to age at disease onset by dividing the cohort in decades (disease onset <30 years, between 30 and 40, 40–50, 50–60 and >60 years).
Impact of sex on phenotype at baseline
We looked at sex influence on age at disease onset, disease subtype and disease phenotype at baseline. We also compared nailfold capillaroscopic patterns (ie, early, active and late pattern) between men and women.23
Impact of sex on disease outcomes
For the patients with follow-up, we focused on those having at least 2 years of follow-up after baseline to estimate the predictive value of sex on disease outcomes including mortality and disease progression. For mortality, analysis was based on the whole cohort (n=9182). Causes of death were separated in SSc related and SSc unrelated.
For disease progression, we focused on severe organ involvement (new digital ulcers (DU)), new onset of pre-capillary pulmonary hypertension (PH) on right heart catheterisation, new onset of reduction of the left ventricular ejection fraction (LVEF) to below 50% as assessed by echocardiography, new occurrence of scleroderma renal crisis (SRC), new onset or worsening of pulmonary fibrosis on X-rays and/or high-resolution CT (HRCT) and deterioration of lung volume (≥10% of forced vital capacity (FVC) during follow-up).
Statistical analysis
A multivariate stepwise logistic regression analysis was performed with calculation of OR estimates and 95% CIs. We applied Bonferroni correction for multiple comparisons (adjusted probability value=0.003) at baseline.
Predictors of disease progression were evaluated by univariate and multivariate Cox proportional hazards models and summarised as HRs and 95% CI. A p value <0.05 was considered statistically significant in the multivariate Cox models.
Further details are provided in online supplementary materials.
Results
The study began at entry to EUSTAR database. In all, 1321/9182 (14.4%) patients with SSc were men and 4756/5260 (90.4%) were white patients. The sex ratio was six women affected for one man. There were 3359/9149 (36.7%) diffuse cutaneous forms. In diffuse cutaneous forms, the sex ratio women/men was 4:1, whereas it was 9:1 in limited cutaneous subtypes. Sex bias was similar whatever age at disease onset, with a sex ratio women/men respectively equal to 8:1 before 30 years, 6:1 between 30 and 60 years and 5:1 after 60 years (figure 1).

Sex bias according to age at disease onset. In abscissa, there are different ages at disease onset, whereas in ordinate, we can find incidence of disease in per cent. The percentage of women was 89 in the group with disease onset below 30 years, 86 in both 30–40 years and 40–50 years, 85 in the group with disease onset between 50 and 60 years and 83 in the group with disease onset after 60 years.
Disease characteristics at baseline
At baseline, mean age (±SD) was 54.3 (13.9) years, whereas mean disease duration (±SD) was 8.5 (9.0) years. Lung fibrosis was detected in 3507/8574 patients, with a diagnosis based on HRCT in 2659 patients (1190 patients had lung fibrosis on HRCT) and on X-rays for the remaining 2915 patients (2317 with lung fibrosis). Right heart catheterisation had been performed in 195 patients (2% of the cohort), revealing pre-capillary PH in 54 patients. However, as right heart catheterisation was only performed in patients with a suspicion of PH, we considered the entire cohort to estimate prevalence of PH.
In univariate analysis, a large number of characteristics were associated with male sex. There was no high association between variables (Cramer's V <0.6).
In multivariate analysis, only variables with >70% of the data available were included. In the multivariate model, adjusted on age, disease duration and anti-Scl70 antibodies, male sex was independently associated with a more severe phenotype as reflected by a higher risk of diffuse cutaneous form (OR: 1.68; 95% CI (1.45 to 1.94), p<0.001), a more active disease (Valentini score ≥3) (OR: 1.39 (1.13 to 1.70), p<0.003) and a higher risk of creatine kinase elevation (OR: 1.93 (1.58 to 2.36), p<0.001). Men were also characterised by a more severe vascular phenotype with an independent association with DU (OR: 1.28 (1.11 to 1.47), p<0.001) and PH (OR: 3.01 (1.47 to 6.20), p<0.003). Women had higher frequencies of anticentromere antibodies (ACA) positivity and of gastrointestinal involvement. Further details are provided in table 1.
Results of the univariate and multivariate analyses (adjusted on age, disease duration and anti-Scl70 antibodies) comparing men and women with SSc at baseline (n=9182 patients)
Concerning nailfold capillaroscopy results (information available for 20% of the cohort), 264/305 (86.6%) men and 1411/1559 (90.5%) women had a scleroderma pattern (p<0.05). Women displayed more frequently an early pattern (279/1085 (25.7%) vs 40/210 (90.5%); p<0.05), whereas men were characterised by an active pattern (103/210 (49.0%) vs 458/1085 (42.2%); p<0.05). There was no significant difference regarding the late pattern (67/210 (31.9%) vs 348/1085 (32.1%); p=NS) (information missing in 54 men and 326 women). After adjusting for disease duration, sex was not associated with a capillaroscopic pattern.
Impact of sex on disease outcomes
Follow-up data
In all, 4499/9182 (49.0%) patients with SSc had a recorded follow-up visit at least 2 years after inclusion. Among them, there were 652 men (14.5%) and 3847 women, resulting in a sex ratio of six women affected for one man. There were 1658/4485 (40.0%) diffuse cutaneous forms. After a mean follow-up of 4.9 (2.7) years, mean age was 58.9 (13.5) years and mean disease duration was 12.7 (8.0) years.
The sample had sufficient power for detecting impact on studied outcomes (see online supplementary table S1). Variables tested in univariate Cox proportional models were those with more than 70% of the data available in the follow-up cohort, resulting in 25 variables tested and four excluded (ie, C-reactive protein elevation, modified Rodnan skin score, LVEF below 50% and FVC below 70%). There was no significant association (Cramer's V<0.60) between all the variables tested.
Organ involvements
In univariate Cox proportional models, male sex was not predictive of either occurrence of new DU or lung progression during the follow-up.
For new onset of PH, we excluded patients with PH at baseline (ie, 22 patients). New occurrence of PH during the follow-up was recorded in 71/4477 (1.6% of the cohort) (right heart catheterisation was performed in 96 patients). In the multivariate analysis, male sex appeared as a predictor of new onset of PH during the follow-up (HR: 2.66 (1.32 to 5.36); p=0.006) together with carbon monoxide diffusing capacity test (DLCO) below 60% predicted (table 2).
Results of the multivariate Cox proportional model for predictors of new onset of pulmonary hypertension during the follow-up (adjusted on age, disease duration, diffuse cutaneous subtype and positivity of anti-Scl70 antibodies)
For cardiac progression, we excluded patients with previous reduction of the LVEF to below 50%, that is, 126 patients. New onset of reduction of LVEF was observed in 41/2784 (1.5%) (data available in 63.7% of the cohort). In the multivariate model, male sex was independently predictive of heart dysfunction (HR: 2.22 (1.06 to 4.63); p=0.035) (table 3).
Results of the multivariate Cox proportional model for predictors of new occurrence heart dysfunction during the follow-up (adjusted on age, disease duration, diffuse cutaneous subtype and anti-Scl70 antibodies)
In univariate Cox proportional model, male sex was predictive of new onset of SRC, but not in multivariate Cox proportional model. Further information is provided in online supplementary information.
Mortality
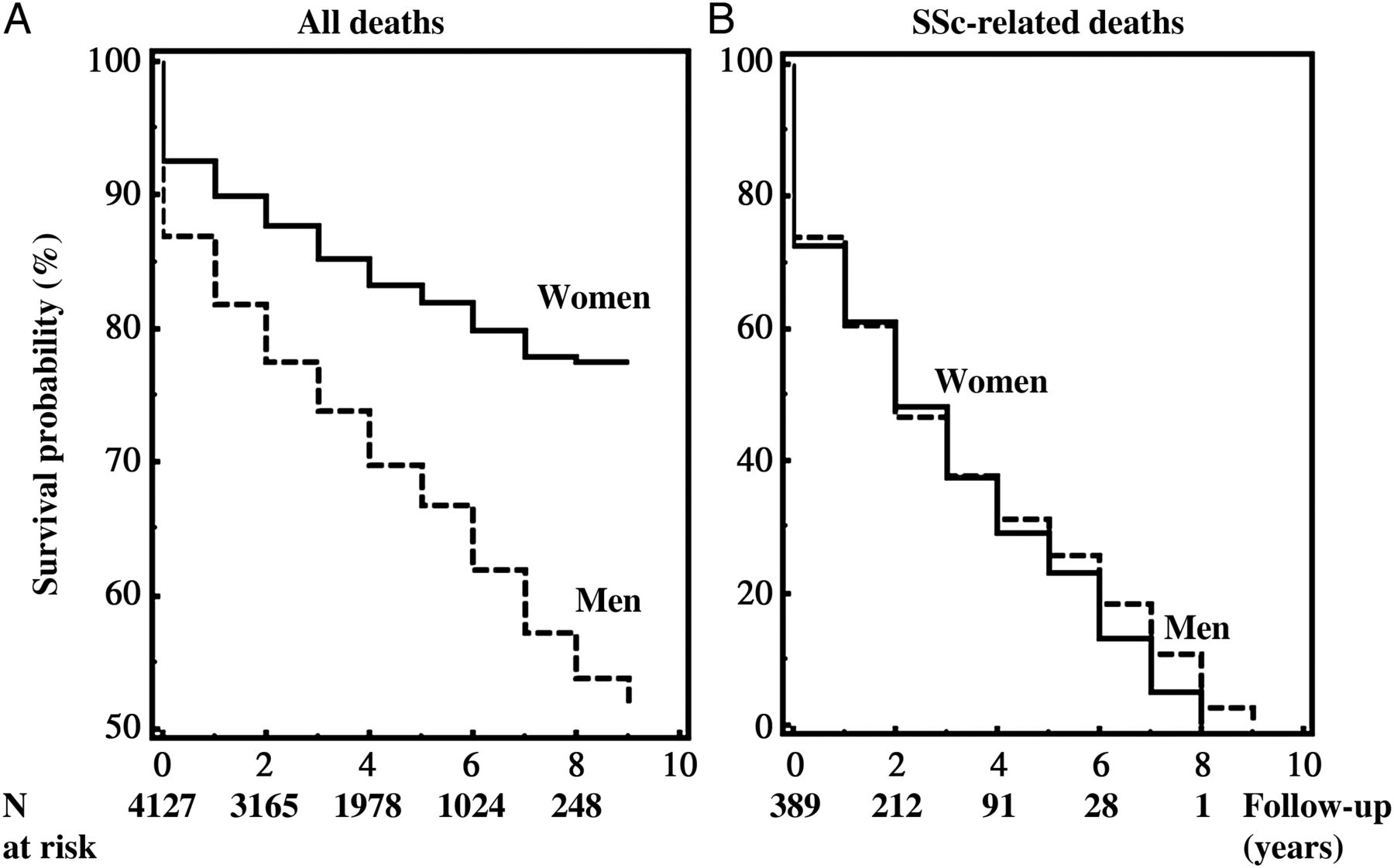
Overall, 908 deaths were recorded (217 (33.1%) men vs 691 (18.0%) women; p<0.001). Men died younger than women (60.4 (13.1) years vs 63.9 (13.6) years; p<0.001) and their disease duration was shorter at death (8.6 (7.9) vs 12.3 (9.3) years; p<0.001) (information available respectively for 908 and 816 dead patients). Death was considered to be SSc-related in 445/665 cases (cause of the death not provided in 243 patients): 115/165 (69.7%) men and 330/500 (66.0%) women; p=0.44. The mean time to death after study inclusion was 2.5±2.2 years. The Kaplan–Meier survival curve displayed a higher survival probability in women compared with men (figure 2A). In multivariate Cox proportional hazard model adjusted on age, disease duration, diffuse cutaneous subtype and positivity of anti-Scl70 antibodies, male sex was identified as an independent predictor of death (HR: 1.48 (1.19 to 1.84); p<0.001). Other independent predictors were musculoskeletal involvement and severe organ involvements (ie, DU, PH and lung fibrosis) (table 4).
{kind=link}
{kind=link}
Kaplan–Meier survival for all deaths (A) and systemic sclerosis (SSc)-related (B) deaths according to sex during the follow-up period. The dotted line represents survival probability in men, whereas the solid line represents survival probability in women. In the bottom, the number of patients with SSc at risk can be noticed.
Results of the multivariate Cox proportional model for predictors of all causes of death (adjusted on age, disease duration, diffuse cutaneous subtype and anti-Scl70 antibodies)
We then focused on SSc-related deaths and observed no significant difference between men and women (figure 2B). Independent predictors for SSc-related mortality were an active disease, muscle weakness, DLCO below 60% and proteinuria at baseline (see online supplementary table S2).
Discussion
In this study, we analysed the impact of sex on SSc, taking advantage of the largest series of (European) patients with SSc ever reported. Our main results are: (i) sex ratio (women/men) in SSc is about 6:1 whatever age at disease onset; (ii) men with SSc have a more severe phenotype and (iii) the prognosis of SSc is worse in men with an increased risk of occurrence of cardiovascular disease (PH and heart dysfunction).
It was already well documented that SSc was associated with a strong female predominance. Our results were concordant with literature data with a sex ratio equal to six affected women for one man.7–11 It has been suggested that the sex ratio in SSc could be higher in the childbearing years and decreased during the postmenopausal years.25 This was also demonstrated in other autoimmune diseases, such as SLE and rheumatoid arthritis.26–28 We did not observe any difference in sex bias according to age at disease onset, suggesting that the female hormonal milieu and the pregnancy-related events were not responsible for this difference in disease susceptibility.29 Other hypotheses have been proposed to explain this sex imbalance in autoimmune diseases, such as sex-specific environmental exposure, foetal microchimerism, skewing in X-chromosome inactivation patterns and X-linked genetic susceptibility risk factors.6 ,30 ,31 This latter factor is supported by a reproducible association between a sex chromosome gene IRAK1 and SSc in two independent studies.31 ,32
In this study, we showed that the disease was strikingly more severe in men, as reflected by an independent association with the diffuse cutaneous subtype, an active disease assessed by Valentini score and with creatine kinase elevation. Conversely, women were characterised by ACA antibodies positivity and a more frequent gastrointestinal involvement. Our results confirm and extent previous studies, reporting a higher frequency of ACA antibodies in women and a higher risk of diffuse cutaneous forms in men.12 ,15 ,33
Our group previously reported that women with SSc were characterised by polyautoimmunity, ACA positivity and limited cutaneous subtype.34 ,35 However, prevalence of polyautoimmunity could not be assessed in the present study because this information was available only in a small proportion of patients.
Our study was the first to rigorously demonstrate that men have a more severe vasculopathy. Indeed, male sex was independently associated with both DU and PH at baseline.
A previous study suggested a higher frequency of DU in men in line with our results.16 However, the sample size and the lack of multivariate analysis in this report could not allow firm conclusions. Herein, we could confirm that male patients have more frequently DU at baseline using multivariate analysis (OR: 1.28 (1.11 to 1.47), p<0.001). However, our prospective analysis failed to demonstrate any association between new occurrence of DU and sex during the follow-up.
Strengthening the relationships between male sex and vasculopathy, male sex was identified as an independent predictor of new occurrence of PH and heart dysfunction during the follow-up, with HR equal to 2.66 and 2.22, respectively. In a previous study, male sex was independently associated with PH assessed by echocardiography.33 However, this study was biased because PH was not confirmed by right heart catheterisation, which is the gold standard for the diagnosis. Our study is the first to demonstrate that male sex is independently associated with PH, but is also predictive of new occurrence of PH during the follow-up, with a stringent definition of PH. It is of interest to notice that usually idiopathic pulmonary arterial hypertension occurs more frequently in women.36 This underlines the specificity of SSc-PH characterised by higher prevalence and incidence in men.
Men were characterised by an active pattern at nailfold capillaroscopy and women by the early one. Some studies suggest that the active pattern is at higher risk of severe peripheral vascular involvement than the early one, which is in accordance with our results.37 However, we did not succeed to demonstrate any association after adjusting for disease duration, probably because of the small size of the sample.
A previous study in EUSTAR cohort reported that male sex was independently associated with left ventricular dysfunction.38 Herein, male sex was identified as an independent predictor of new occurrence of heart dysfunction during the follow-up. These results are of major interest since PH and heart dysfunction are the leading causes of death in SSc39 and herein we show, for the first time, in a prospective study, that male sex is predictive of these two life-threatening outcomes. Note that we could not assess the association of heart dysfunction and outcome during the follow-up or male sex at baseline because LVEF was available for <70% of the cohort. Another critical issue is survival in SSc.40 We herein observed that male sex was independently predictive of death. This is concordant with few previous cohort studies reporting a better survival for female patients.8 ,12 ,14 ,16 ,41 In a preliminary EUSTAR study, male sex appeared as a risk factor to predict mortality.18 Our results obtained through the largest worldwide database confirmed these data by showing a higher mortality in affected men with 1.8-fold more deaths in men compared with women. However, when we stratified on SSc-related mortality, there was no significant difference between men and women. Several hypotheses might be driven to explain this discrepancy. First, this difference might be related to the inherent difference between men and women regarding SSc-unrelated mortality.42 This underlines the bias of considering all deaths instead of SSc-related deaths to estimate the impact of sex on mortality. In the same way, observational studies, which used the standardised mortality ratio, adjusted on sex and age, did not find any difference between men and women or suggested an increased risk of death among women.9 ,43–45 However, the mean follow-up (5 years) might be too short to allow an accurate detection of predictive factors of death and SSc-related deaths. With this follow-up, we observed that severe organ involvements were more prevalent in men, but deaths related to these organ involvements might occur several years later.
Our study should be interpreted within some limitations: first, the exact cause of death could not be analysed because these data were not available. Furthermore, we could not perform adjustment for comorbidities, except arterial hypertension, which was as prevalent in men and women (table 1). Moreover, despite all the efforts made by EUSTAR to homogenise the care of patients with SSc, the participation of several centres might have introduced some heterogeneity in their assessment and some factors could not be included in the analysis because of missing values. Finally, our findings appear as robust in white Europeans but might not be applied generally to other ethnicities.
However, our study has several strengths: data were derived from a large, multicentre cohort, with an extensive list of clinical, laboratory and diagnostic parameters. Furthermore, unlike previous retrospective and cross-sectional clinical studies, our data collection was prospective to identify the impact of sex on disease progression and outcomes. In addition, most of the variables were available for more than 80%–90% of the cohort and thus analysed in our different multivariate models, which confirm the robustness of our study (table 1). Finally, in contrast to previous studies, we used the new ACR/EULAR classification allowing increasing the number of patients included and the representativeness of our cohort.
Novelty in our analysis lies on the identification of a more severe vasculopathy in men. The mechanisms that explain these discrepancies are still unknown and very challenging.
Our results suggest taking sex into account (i) for the patient management with a particular attention to vascular manifestations in men, (ii) for the analysis of drug effects in clinical trials and (iii) may open new avenues for SSc research, which needs to evaluate both genetic and environmental influences according to sex. Stratification or adjustment according to sex should allow identifying which therapeutic strategy has the greatest benefit for men and women, leading to the development of sex-tailored treatment regimens, as it has been recently demonstrated in depression and hepatitis C.46 ,47
Acknowledgments
EUSTAR acknowledges the unconditioned support that EULAR has provided in the past for the maintenance of the EUSTAR database.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
Collaborators Serena Guiducci; Alan Tyndall; Giovanni Lapadula; Florenzo Iannone; Radim Becvar; Stanislaw Sierakowsky; Otylia Kowal Bielecka; Maurizio Cutolo; Alberto Sulli; Giovanna Cuomo; Serena Vettori; Simona Rednic; Ileana Nicoara; P. Vlachoyiannopoulos; C. Montecucco; Roberto Caporali; Srdan Novak; László Czirják; Cecilia Varju; Carlo Chizzolini; Eugene J. Kucharz; Anna Kotulska; Magdalena Kopec-Medrek; Malgorzata Widuchowska; Blaz Rozman; Carmel Mallia; Bernard Coleiro; Armando Gabrielli; Dominique Farge; Adrian Hij; Roger Hesselstrand; Agneta Scheja; Frank Wollheim; Duska Martinovic; M. Govoni; Andrea Lo Monaco; Nicolas Hunzelmann; Raffaele Pellerito; Lisa Maria Bambara; Paola Caramaschi; Carol Black; Christopher Denton; Jörg Henes; Vera Ortiz Santamaria; Stefan Heitmann; Dorota Krasowska; Matthias Seidel; Mara Oleszowsky; Harald Burkhardt; Andrea Himsel; Maria J. Salvador; Bojana Stamenkovic; Aleksandra Stankovic; Mohammed Tikly; Maya N. Starovoytova; Merete Engelhart; Gitte Strauss; Henrik Nielsen; Kirsten Damgaard; Gabriella Szücs; Antonio Zea Mendoza; Carlos de la Puente Buijdos; Walter A. Sifuentes Giraldo; Øyvind Midtvedt; Torhild Garen; David Launay; Guido Valesini; Valeria Riccieri; Ruxandra Maria Ionescu; Daniela Opris; Laura Groseanu; Fredrick M. Wigley; Carmen M. Mihai; Roxana Sfrent Cornateanu; Razvan Ionitescu; Ana Maria Gherghe; Marilena Gorga; Rucsandra Dobrota; Mihai Bojinca; Georg Schett; Jörg HW Distler; Pierluigi Meroni; Silvana Zeni; Luc Mouthon; Filip De Keyser; Vanessa Smith; Francesco P. Cantatore; Ada Corrado; Susanne Ullman; Line Iversen; Maria R. Pozzi; Kilian Eyerich; Rüdiger Hein; Elisabeth Knott; Jacek Szechinski; Piotr Wiland; Magdalena Szmyrka-Kaczmarek; Renata Sokolik; Ewa Morgiel; Brigitte Krummel-Lorenz; Petra Saar; Martin Aringer; Claudia Günther; Branimir Anic; Marko Baresic; Miroslav Mayer; Sebastião C. Radominski; Carolina de Souza Müller; Valderílio F. Azevedo; Svetlana Agachi; Liliana Groppa; Lealea Chiaburu; Eugen Russu; Thierry Zenone; Simon Stebbings; John Highton; Lisa Stamp; Peter Chapman; Murray Baron; John O'Donnell; Kamal Solanki; Alan Doube; Douglas Veale; Marie O'Rourke; Esthela Loyo; Edoardo Rosato; Simonetta Pisarri; Cristina-Mihaela Tanaseanu; Monica Popescu; Alina Dumitrascu; Isabela Tiglea; Rodica Chirieac; Codrina Ancuta; Daniel E. Furst; Suzanne Kafaja; Paloma García de la Peña Lefebvre; Silvia Rodriguez Rubio; Marta Valero Exposito; Jean Sibilia; Emmanuel Chatelus; Jacques Eric Gottenberg; Hélène Chifflot; Ira Litinsky; Algirdas Venalis; Irena Butrimiene; Paulius Venalis; Rita Rugiene; Diana Karpec; Eduardo Kerzberg; Fabiana Montoya; Vanesa Cosentino.
Contributors Study conception and design: ME, JA, OD and YA. Acquisition of data: ME, JA, UAW, MM-C. GR. PA. EH. GV. PEC. FC. ABG. YB-M. ND. LPA. RS. SJ. JB. ML. UM-L. AK. OD and YA. Analysis and interpretation of data: ME, JA, UAW, MM-C, GR, PA, EH, GV, PEC, FC, ABG, YB-M, ND, LPA, RS, SJ, JB, ML, UM-L, AK, OD and YA All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published.
Competing interests OD has/had consultancy relationship and/or has received research funding in the area of systemic sclerosis and related conditions from Actelion, Pfizer, Ergonex, BMS, Sanofi-Aventis, United BioSource Corporation, Roche/Genentech, Medac, Biovitrium, Boehringer Ingelheim Pharma, Novartis, 4 D Science, Active Biotec, Bayer-Schering, Sinoxa, Serodapharm, EpiPharm and Biogen.
Patient consent Obtained.
Ethics approval Paris CPP Ile de France 3.
Provenance and peer review Not commissioned; externally peer reviewed.