Article Text

Abstract
Objectives To examine whether MRI features predict radiographic progression including erosive evolution in patients from the Oslo hand osteoarthritis (OA) cohort, which is the first longitudinal hand OA study with available MRI.
Methods We included 74 patients (91% female, mean (SD) age of 67.9 (5.3) years) with MRI of the dominant hand and conventional radiographs taken at baseline and 5-year follow-up. Baseline MRIs were read according to the Oslo hand OA MRI score. We used three definitions of radiographic progression: Progression of joint space narrowing (JSN, grades 0–3), increased Kellgren–Lawrence score (grades 0–4) or incident erosions (absent/present). For each definition, we examined whether MRI features predicted radiographic progression in the same joint using Generalised Estimating Equations. We adjusted for age, sex, Body Mass Index, follow-up time and other erosive joints (the latter for analyses on incident erosions only).
Results MRI-defined moderate/severe synovitis (OR=3.52, 95% CI 1.29 to 9.59), bone marrow lesions (BML) (OR=2.73, 95% CI 1.29 to 5.78) and JSN (severe JSN: OR=11.05, 95% CI 3.22 to 37.90) at baseline predicted progression of radiographic JSN. Similar results were found for increasing Kellgren–Lawrence score, except for weaker association for JSN. Baseline synovitis, BMLs, JSN, bone damage, osteophytes and malalignment were significantly associated with development of radiographic erosions, of which malalignment showed the strongest association (OR=10.18, 95% CI 2.01 to 51.64).
Conclusions BMLs, synovitis and JSN were the strongest predictors for radiographic progression. Malalignment was associated with incident erosions only. Future studies should explore whether reducing BMLs and inflammation can decrease the risk of structural progression.
- Hand Osteoarthritis
- Magnetic Resonance Imaging
- Outcomes research
Statistics from Altmetric.com
Introduction
Hand osteoarthritis (OA) is usually a slowly progressing disease, whereas some patients show more rapid progression leading to severe joint damage.1 A subset of patients develops erosive hand OA, which is often associated with more inflammatory findings.2 Hence, erosive hand OA is often called ‘inflammatory OA’.3 Currently, we have limited knowledge about factors that predict development of severe structural disease or erosive hand OA.
A recent hand OA study by Kortekaas et al4 showed that ultrasound-detected synovitis predicted radiographic progression, suggesting that inflammation also plays an important role in the pathogenesis of non-erosive disease. Bijsterbosch et al5 found that radiographic joint space narrowing (JSN) was the major predictor for erosive evolution of the same joint. However, joint tenderness, as a possible marker of inflammation, was also significantly associated with development of erosions.
Traditionally, measurement of OA structures has relied upon conventional radiography, which demonstrates destruction of cartilage visualised as reduced joint space and bone damage as destructive (erosions) or osteoproliferative (osteophytes) changes. During the recent years, ultrasonography has gained a more important role both in clinical and research settings as a good supplement for demonstration of joint inflammation. MRI is a sensitive tool with the advantage of a whole-joint demonstration.6 Previous cross-sectional MRI studies in hand OA have indicated that MRI is more sensitive than conventional radiography to detect structural OA features, probably due to the multiplanar joint demonstration.7 ,8 Furthermore, MRI demonstrates joint inflammation, which is not visualised by conventional radiographs,9 and is the only imaging modality that demonstrates diffuse marginated bone marrow lesions (BML). Despite these advantages, more data is needed to clarify the clinical relevance of MRI, such as associations between MRI features and future disease progression.10 Due to the lack of longitudinal hand OA studies in which MRI is obtained, it is unknown whether MRI-defined synovitis or other MRI features such as BMLs predict radiographic progression including erosive evolution. This knowledge may also provide further insight into the pathophysiology of hand OA.
Hence, our aim was to examine whether MRI features can predict hand OA radiographic progression including development of erosions 5 years later.
Methods
Patients
Participants of the Oslo hand OA cohort have attended three scheduled examinations (figure 1). In 2001–2003 (examination 1), 209 patients with hand OA were examined with joint assessments, conventional radiography and questionnaires. Details of the patient recruitment have been published elsewhere.11 The same examinations were performed in 2008–2009 (examination 2) and 2013 (examination 3). At examination 2, the participants also underwent MRI of the dominant hand. The Regional Ethical Committee approved the study, and all participants signed informed consent.
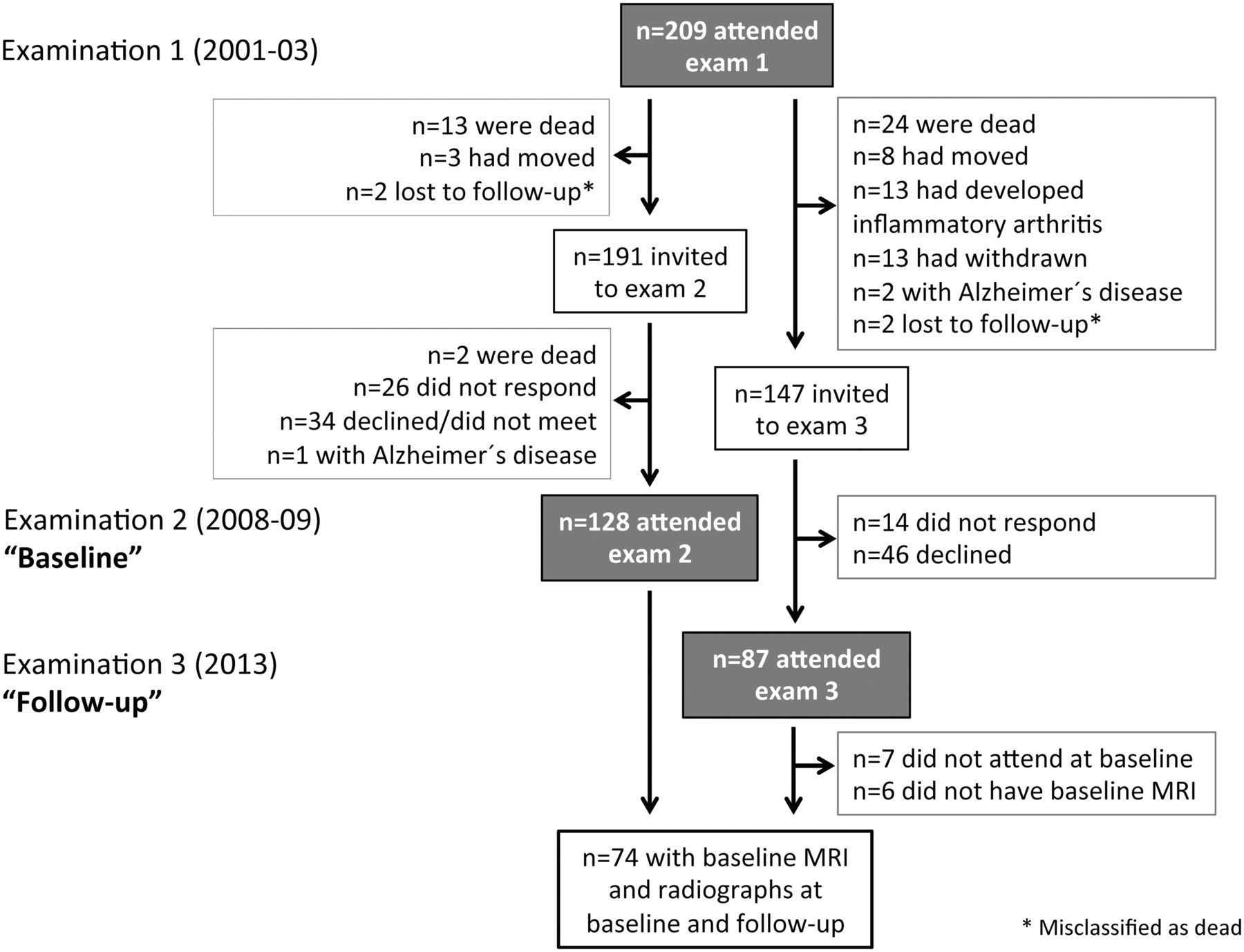
{kind=link}
Flowchart showing the number of participants who have been followed in the Oslo hand osteoarthritis cohort.
In the current analyses, we included 74 participants with available MRI of the dominant hand at examination 2 (hereafter referred to as ‘baseline’) and conventional radiography at both examination 2 (baseline) and examination 3 (hereafter referred to as ‘follow-up’). Among the 87 participants who attended the follow-up examination in 2013, there were no significant differences in sex distribution (p=0.25), mean age (p=0.40) or mean amount of radiographic OA at follow-up (p=0.71) between those who were included (n=74) and not included (n=13) in the analyses.
Imaging
MRI of the dominant hand was performed at baseline (2008–2009). The 2nd–5th distal and proximal interphalangeal joints were imaged using a high-field extremity 1.0 T MRI unit (ONI, GE Healthcare, Waukesha, Wisconsin, USA) and a cylindrical coil (diameter 10 cm). Coronal, sagittal and axial T1-weighted fat-suppressed preintravenous and postintravenous Gadolinium (0.1 mmol Gadolinium/kg body weight; Magnevist, Bayer Schering Pharma AG, Leverkusen, Germany) images were acquired from a three-dimensional dual-echo Dixon technique (repetition time (TR) 20 ms, echo time (TE) 5 ms, 1 mm slice thickness), in addition to coronal and axial Short Tau Inversion Recovery images (TR 2850 and 3150 ms, TE 16.3 and 21 ms, 2 and 3 mm slice thickness, respectively). One reader (IKH) scored the baseline MRIs according to the Oslo hand OA MRI score for presence of synovitis (grades 0–3), flexor tenosynovitis (grades 0–3), focal erosions (grades 0–3), subchondral bone attrition (absent/present), cysts (absent/present), osteophytes (grades 0–3), JSN (grades 0–3), BMLs (grades 0–3), malalignment (absent/present), collateral ligament discontinuity (absent/present). Detailed description of the scoring system and its reliability has been published.12 Focal erosions (sharply marginated bone lesions with cortical break) and subchondral bone collapse (central erosions with typical ‘seagull wing’ configuration) were scored separately as opposed to the proposed scoring system.
Bilateral hand radiographs (posteroanterior view) were obtained at baseline (2008–2009) and follow-up (2013). One reader (IKH) scored the paired hand radiographs with known time sequence according to the Osteoarthritis Research Society International atlas for JSN (grades 0–3) and erosions (absent/present) and according to a modified Kellgren–Lawrence scale (grades 0–4): KL grade (KLG) 0=no hand OA; 1=minimal hand OA, that is, questionable osteophyte and/or JSN; 2=mild hand OA, that is, small osteophyte(s) and/or mild JSN, sclerosis may be present; 3=moderate hand OA, that is, moderate osteophyte(s) and/or moderate JSN, sclerosis and erosions may be present; 4=severe hand OA, that is, large osteophyte(s) and/or severe JSN, sclerosis and erosions may be present.1 ,13 The reader has shown moderate to good intrareader reliability (KLG: weighted κ=0.82, JSN: weighted κ: 0.61, erosions: κ=0.81).14
Readings of MRIs and conventional radiographs were performed blinded for clinical information and other imaging features.
Statistics
We used three definitions of radiographic progression: (1) progression of JSN (JSN change ≥1 in joints with baseline JSN=0–2); (2) increasing global OA severity (KLG change ≥1 in joints with baseline KLG=0–3) and (3) incident radiographic erosions in joints without erosions at baseline.
At joint level, we calculated the OR (95% CI) of radiographic progression (dependent variables) for the various baseline MRI features (independent variables) using Generalised Estimating Equations (modelled as a logistic regression model with binary responses). Separate analyses were performed for each MRI feature and each definition of radiographic progression. Joints with no potential for progression (JSN=3, KLG=4 and erosions at baseline) were excluded from the respective analyses. For joints that were scored for MRI features in the distal and proximal part of the joint separately (ie, focal erosions, attrition, cysts, osteophytes and BMLs), we used the maximum score. A possible dose–response relationship was explored for MRI features that were scored on 0–3 scales. In case of no significant dose–response relationship, we present the odds of progression in joints with the MRI feature compared with those without. Joints without the current MRI features served as reference if not stated otherwise. Due to few joints without osteophytes, joints with no or small osteophytes served as reference. For erosive evolution, joints with no or mild JSN served as reference, as all joints with erosive evolution had JSN at baseline.
We adjusted for sex, age and Body Mass Index (BMI) at baseline and follow-up time. Analyses on erosive development were additionally adjusted for absence/presence of other erosive joints at baseline. Analyses on erosive development were hampered by colinearity between sex and erosive development, and we therefore excluded seven eligible men from the analyses. For radiographic progression, we used an unstructured correlation matrix, whereas we used an exchangeable matrix for erosive evolution due to less observations and need for a less complex matrix.
Analyses were performed using IBM SPSS Statistics V.21, and p values <0.05 were considered statistically significant.
Results
Baseline characteristics are shown in table 1. Most participants had severe radiographic hand OA. Erosive disease was present in 42 persons (56.8%), of whom 39 were women. MRI-defined synovitis, osteophytes, JSN and collateral ligament discontinuity were frequently present, whereas flexor tenosynovitis, BMLs, erosions, attrition, cysts and malalignment were less common (table 1).
Baseline demographics and clinical characteristics
MRI findings as predictors for progression of radiographic JSN
The mean (SD) follow-up time was 4.6 (0.4) years. The 74 patients had 507 eligible joints with baseline JSN ≤2 (n=85 joints with baseline JSN=3 were excluded), of which 86 (17.0%) showed radiographic progression during follow-up. The majority of joints with progression had one grade increase of JSN score (table 2).
The number (%) of joints with radiographic progression
In the crude regression analyses, moderate/severe synovitis, JSN and BMLs at baseline could predict progression of JSN during follow-up. In the adjusted analyses, the observed associations remained statistically significant. Statistically significant association was also demonstrated for cysts in the adjusted analyses (table 3). A dose–response relationship was found for synovitis and JSN. For synovitis, only moderate/severe synovitis was associated with increasing JSN score. Few joints had moderate (n=5) and severe BMLs (n=9), and a dose–response relationship could, therefore, not be explored (table 3).
Baseline MRI findings as predictors for progression of radiographic JSN in the same joint
The association between moderate/severe synovitis (OR=3.35, 95% CI 1.01 to 10.30; p=0.03) and radiographic progression was independent of BMLs (OR=3.52, 95% CI 1.28 to 9.68; p=0.01), when both features were included in the same model. We chose to not adjust for structural features as synovitis and BMLs may be intermediate variables between structural features and OA progression.15
MRI findings as predictors for radiographic progression of structural OA (Kellgren–Lawrence)
The 74 patients had 498 eligible joints with baseline KLG ≤3 (n=94 joints with KLG=4 were excluded), of which 120 (24.1%) showed radiographic progression during follow-up. The majority of joints with progression had one grade increase of KLG (table 2).
In the crude regression analyses, synovitis, JSN and BMLs could significantly predict increasing KLG (table 4). In the adjusted analyses, the associations remained statistically significant for synovitis, moderate JSN and BMLs. Both mild and moderate/severe synovitis were associated with increasing KLG, but no clear dose–response relationship was observed. When analysing moderate and severe synovitis separately, a dose–response relationship was found (data not shown). However, only eight joints had severe synovitis. A less clear-cut dose–response relationship was observed for baseline JSN, of which only moderate JSN was significantly associated with increasing KLG. Few joints had moderate (n=5) and severe BMLs (n=9), and a dose–response relationship could, therefore, not be explored (table 4).
Baseline MRI findings as predictors for radiographic progression according to the Kellgren–Lawrence scale in the same joint
Mild (OR=2.67, 95% CI 1.55 to 4.61; p<0.001) and moderate/severe synovitis (OR=2.34, 95% CI 1.05 to 5.24; p=0.04) were significant predictors of radiographic progression independent of BMLs (OR=2.55, 95% CI 1.24 to 5.26; p=0.01).
MRI findings as predictors for development of radiographic erosions
Among the 67 women included in the analyses, erosive evolution appeared in 40 of 438 (9.1%) joints that were non-erosive at baseline.
In the crude regression analyses, the majority of MRI features predicted development of erosions. In the adjusted analyses, statistically significant associations were found for moderate/severe synovitis, BMLs and JSN (table 5). Compared with the associations to progression of JSN (table 3), stronger associations were observed for synovitis and BMLs (table 5). Furthermore, features of bone damage (ie, erosions and attrition) as well as osteophytes, could significantly predict erosive development. Malalignment, which was not associated with progression of JSN or KLG, was the strongest risk factor for erosive evolution (table 5).
Baseline MRI findings as predictors for development of radiographic erosions in the same joint
The association between moderate/severe synovitis (OR=3.99, 95% CI 0.99 to 16.14, p=0.05) and development of erosions was independent of BMLs (OR=4.76, 95% CI 1.68 to 13.48; p=0.003).
Development of radiographic erosions occurred in 25 different participants (1–3 incident erosions per patient), of whom 22 already had radiographic erosions in other finger joints at baseline. Having other joints with radiographic erosions was a strong risk factor for erosive development in previously radiographic non-erosive joints (OR=12.99, 95% CI 4.00 to 42.20; p<0.001 in a model adjusted for age, BMI and follow-up time). In the same model, neither age nor BMI could predict erosive development (data not shown).
Discussion
This is the first study to explore the predictive value of MRI in hand OA. We found that MRI-defined synovitis, BMLs and JSN at baseline predicted radiographic progression including development of erosions in the same joint. Furthermore, MRI-defined bone damage, osteophytes and malalignment were associated with incident erosions, of which malalignment was the strongest predictor. These findings suggest that radiographic progression is affected by inflammation as well as biomechanical factors. Being able to detect patients who are more likely to progress is crucial both in clinical settings as well as clinical trials.
Synovitis was a significant predictor for all measures of radiographic progression including development of erosions. OA is no longer seen as a non-inflammatory wear-and-tear disease, but a disease in which the synovium also plays a pivotal role.16 According to the traditional view of synovitis, cartilage matrix macromolecules are released into the joint fluid during degradation, triggering a secondary inflammation reaction.16 The inflammatory mediators produced by the synovial cells have a catabolic effect on the cartilage, creating a viscous circle.16 This study confirms with MRI that synovitis is a risk factor for OA progression and erosive evolution, assessed by conventional radiographs.
A recent hand OA study by Kortekaas et al4 found that inflammatory features shown by ultrasonography, especially when persistently present, were independently associated with radiographic progression after 2.3 years. Using a different imaging modality, our results are in line with these findings. Synovitis as a risk factor for knee OA progression has been studied with inconsistent results. Longitudinal studies using arthroscopy demonstrated a positive correlation between the severity of synovitis and the progression of cartilage lesions over time.17 ,18 Later MRI studies in knee OA have shown inconsistent results.19–22 Whether inflammation is a more important risk factor for OA progression in hands compared with knees should be further explored.
To our knowledge, this study is the first to demonstrate an association between synovitis and incident erosions. In line with our results, Bijsterbosch et al5 found that painful joints, as a possible marker of local inflammation, were a risk factor for development of erosions. Systemic inflammation (ie, levels of high sensitivity C-reactive protein) was, on the other hand, not related to development of erosions.5
BMLs predicted radiographic OA progression, and we found a strong association between BMLs and erosive development. Cysts were also associated with radiographic progression, although no significant associations were found. One knee OA study has suggested that these features represent the same process, and that BMLs may develop into cysts.23 Our results are in line with previous knee OA studies, which have demonstrated strong evidence for an association between BMLs and the risk of total knee replacement24–28 as well as MRI-defined cartilage loss.20 ,27 ,29–32 In knee OA, BMLs are considered as the structural equivalent of malalignment, which is a major determinant for knee OA progression.33 Due to increased loading in malaligned knees, bone trauma with remodelling is occurring in the subchondral bone, representing BMLs. The histological content of BMLs in hand OA is currently unknown. However, assuming that BMLs in hand OA represents areas of bone trauma and remodelling, our results may suggest that erosions occur at least partly due to bone remodelling in joints with increased loading of the subchondral bone. This hypothetical sequence of events needs to be confirmed in longitudinal studies.
Previous studies have shown that synovitis and BMLs can be modified by pharmacological treatment.34 ,35 Currently, we have no evidence that curbing the inflammation and BMLs in hand OA will lead to less disease progression, and future studies are needed. No studies in humans have explored the effect of steroids on structural OA progression. A study on dogs with induced OA found no effect of continuous treatment with steroids on the long-term structural progression.36 Anti-tumour necrosis factor (anti-TNF) treatment has been tested in hand OA. Verbruggen et al37 found that TNF-blockade could prevent development of erosions in joints with clinical soft tissue swelling, suggesting that halting the inflammation reduces the risk of erosions. Furthermore, TNF-blockade may reduce the development of secondary OA in patients with rheumatoid arthritis.38 On the other hand, no association was found between anti-TNF therapy and reduced pain in a placebo-controlled trial.39 Bisphosphonates target bone remodelling and can therefore reduce BMLs.35 Animal studies have shown conflicting evidence on whether bisphosphonates are preventing cartilage damage,40 ,41 and there is a lack of long-term data on OA joint structure modification postbisphosphonate therapy.42 The effect of bisphosphonates on structural progression in humans has been explored in one observational study only, showing a trend towards a beneficial effect that was not statistically significant.43 Furthermore, a randomised trial on strontium ranelate, another medication traditionally used for osteoporosis, suggested that reduction in BMLs may protect against cartilage loss.44 ,45
Higher JSN at baseline was a strong risk factor for further narrowing of the joint space. These results are in line with previous studies in knee OA.46 The strong association between severe MRI-defined JSN and development of erosions was of similar magnitude as previously shown for radiographic JSN.5 Unexpectedly, we found no association between malalignment and OA progression, defined as increasing JSN or KLG. On the other hand, malalignment was the strongest risk factors for incident erosions, which is in line with a study in knee OA showing an association between malaligment and incident MRI-defined subchondral bone attrition.47 These results support that biomechanical factors are strongly involved in the pathogenesis of erosive hand OA.
Bone damage and osteophytes were associated with development of erosions, but not increasing JSN or KLG. Hence, MRI visualises focal erosions and subchondral bone attrition before they are visible on conventional radiographs. Furthermore, erosive disease may be associated with more bone remodelling compared with non-erosive disease (ie, strong association between BMLs and erosions), which may also lead to bone formation seen as osteophytes.
In addition to the MRI features, we found that having other erosive joints at baseline was a strong risk factor for developing more erosive joints, as previously shown by Bijsterbosch et al.5 In the Framingham study, knee bone attrition and hand erosions were significantly associated. However, the association was no longer significant when we adjusted for the burden of OA. These results suggest that the association was best explained by a heightened burden of disease in certain patients.48
The analyses are limited by MRI at only one time point and only one reader. Furthermore, frontal hand radiographs may underestimate the degree of OA progression. JSN posteriorly and anteriorly can be more optimally evaluated using lateral view or other imaging modalities such as MRI. Future studies should explore whether MRI is more sensitive to change and whether persistent inflammation and BMLs are associated with a higher risk of progression than fluctuating features.
In conclusion, the current 5-year longitudinal hand OA study is the first to demonstrate that MRI-detected JSN, synovitis and BMLs at baseline can predict radiographic progression including development of erosions in the same joint. Furthermore, malalignment was the strongest risk factor for development of erosions. These results suggest that both inflammation and mechanical load are of importance in the pathogenesis of hand OA progression.
Acknowledgments
We thank the patients of the Oslo hand OA cohort for participating in this study, study nurses and technicians in the department of radiology for helping us to collect the data.
References
Footnotes
Handling editor Hans WJ Bijlsma
Contributors IKH was involved in study design, data collection, drafting and final approval of the manuscript. BS-C, PB and SS were involved in study design, data collection, critical appraisal and final approval of the manuscript. DvdH and TKK were involved in study design, critical appraisal and final approval of the manuscript.
Funding The study is supported by grants from ‘Extrastiftelsen’/’the Norwegian Rheumatology Organization’, ‘Grethe Harbitz’ legacy for combating rheumatic diseases’ and ‘Dr Trygve Gythfeldt og wife's research fund’.
Competing interests None.
Patient consent Obtained.
Ethics approval Regional Ethical Committee.
Provenance and peer review Not commissioned; externally peer reviewed.