Article Text

Abstract
Objectives To investigate whether baseline disease activity levels and responses in patients with rheumatoid arthritis (RA) changed during the period 2000–2010.
Methods Data were provided by the Norwegian disease-modifying antirheumatic drug (NOR-DMARD) study. Patients with inflammatory joint diseases starting new treatment with disease-modifying antirheumatic drugs (DMARDs) were consecutively included and followed longitudinally. Time trend analyses were performed in methotrexate (MTX)-naïve RA patients starting MTX monotherapy (MTX mono) and biologic DMARD (bDMARD)-naïve RA patients starting tumour necrosis factor inhibitors+MTX (TNFi+MTX).
Results A total of 2573 patients were included in the analyses: MTX mono n=1866 (69.9% female, 62.0% RF+, mean (SD) age 56.0 (13.7) years, median (25–75 percentile) time from diagnosis 0.2 (0.01–2.8) years); TNFi+MTX n=707 (70.3% female, 75.0% RF+, mean (SD) age 52.1 (13.2) years, median (25–75 percentile) time from diagnosis 5.7 (2.0–13.7) years). Significant time trends towards lower baseline disease activity score 28 (DAS28) as well as other disease activity measures were found in both groups (DAS28 from 5.17 to 4.75 in MTX mono and from 5.88 to 4.64 in TNFi+MTX), and disease duration became shorter. Six-month DAS28 remission rates increased significantly over the years (from 17.8 to 37.6 in MTX mono and from 16.9 to 46.3 in TNFi+MTX).
Conclusions During the last decade, baseline RA disease activity level at the time of starting MTX as well as TNFi+MTX decreased from high to moderate. A more than twofold increase in 6-month remission rates was observed in both groups. Our findings indicate that clinicians have implemented modern, more aggressive treatment strategies, which hopefully will lead to better long-term disease outcomes.
- Rheumatoid Arthritis
- Methotrexate
- TNF-alpha
Statistics from Altmetric.com
Introduction
During the past decade, there has been increasing focus on early, aggressive treatment of rheumatoid arthritis (RA) to prevent joint damage, loss of function and decreased quality of life.1–4 It has been widely accepted that treatment with disease-modifying antirheumatic drugs (DMARDs), particularly methotrexate (MTX), should be started as soon as the diagnosis of RA has been made.1 ,3 Furthermore, the introduction of tumour necrosis factor inhibitors (TNFi) and other biologic DMARDs (bDMARDs) has constituted a major advance in the treatment of patients not responsive to treatment with conventional, synthetic DMARDs (sDMARDs)-like MTX.4
An increasing number of available bDMARDs and new treatment strategies, including the concept of ‘window of opportunity’, contribute to earlier start of sDMARDs and have also made it possible for the clinician to add bDMARDs earlier in the disease and at a lower level of disease activity.5–7 Modern treatment strategy of RA includes early diagnosis, early start with MTX, setting a treatment target (remission or low-disease activity), tight monitoring and switching of therapy if the target is not achieved within 3–6 months.1 ,3 ,7–11
The guidelines for prescribing TNFi in Norway are relatively liberal: patients with RA only need to have failed one sDMARD—MTX if not contraindicated—before starting a bDMARD, and such a treatment can be instituted in patients with moderate and not only high disease activity.12 The recommendations for initiating TNFi treatment in RA elsewhere in Europe vary, and in many other countries failure of two or more sDMARDs and/or a high-disease activity level are required.13–15
Efficacy of new treatment strategies and drugs is usually established through randomised controlled trials (RCTs). However, observational studies reflect everyday clinical practice and can provide information that is complementary to results from RCTs. Whether the implementation of more aggressive treatment strategies has led to improved outcomes in patients with RA in clinical practice in the last decade is not yet well documented. The aim of this study of real-life data from a drug register was to investigate possible time trends and changes in baseline disease activity levels, response and remission rates in patients with RA starting MTX monotherapy or TNFi+MTX during the period 2000–2010.
Methods
The Norwegian disease-modifying antirheumatic drug (NOR-DMARD) study
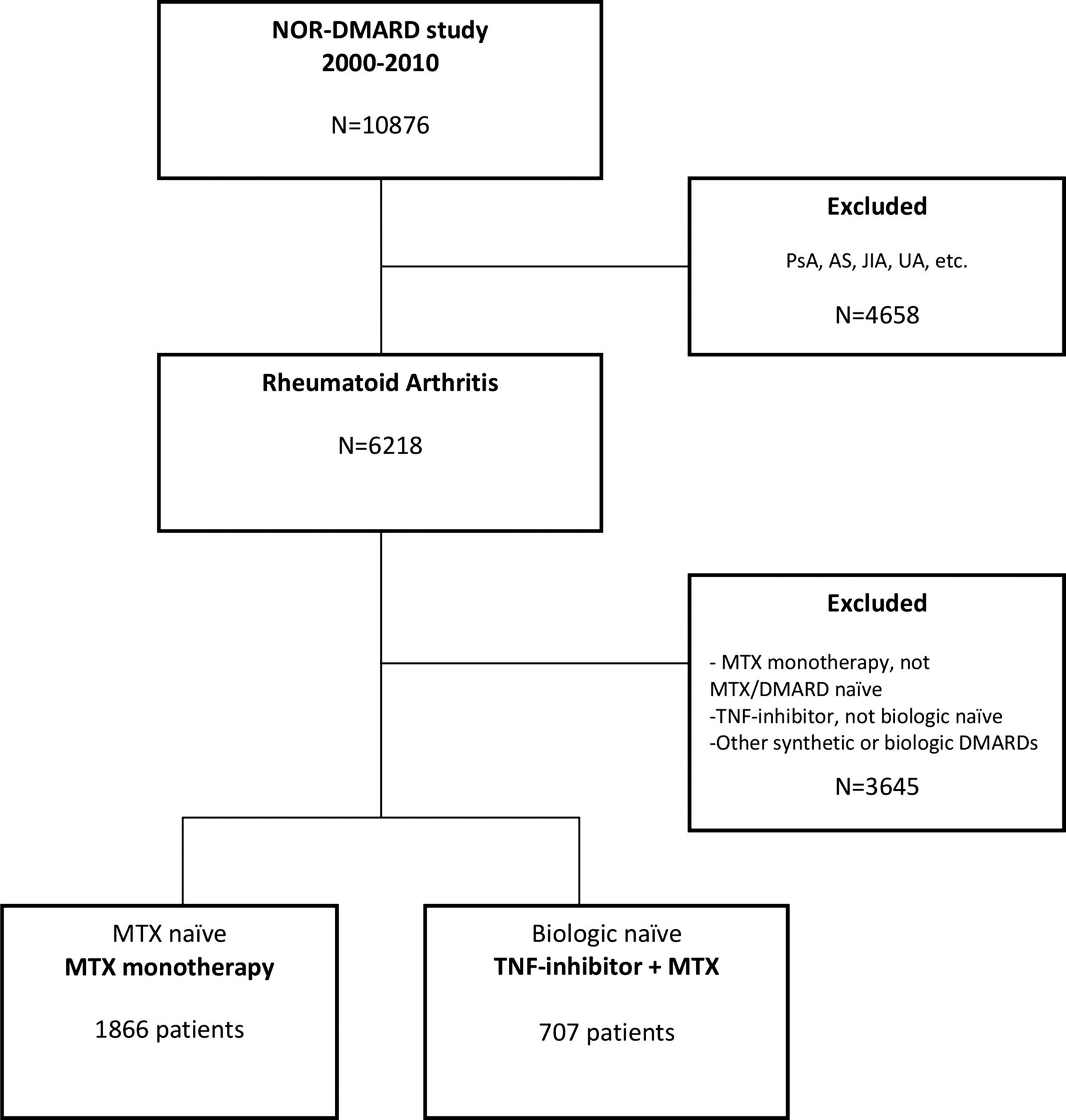
From 2000 to 2010, adult patients (>18 years of age) with inflammatory joint diseases in five Norwegian rheumatology departments starting treatment with sDMARDs or bDMARDs were included in the NOR-DMARD study. The five centres together cover more than 1.5 million inhabitants, nearly 30% of the Norwegian population. The study design was a prospective multicentre longitudinal observational study with assessments at baseline, after 3, 6 and 12 months and then yearly. The completeness of the register has been approximately 85%; the remaining 15% were either missed for inclusion, refused enrolment or were excluded due to language barriers or inclusion in ongoing randomised controlled trials. A total of 10 876 treatment courses in more than 7300 individual patients had been included in the NOR-DMARD study per December 2010. An overview of the study is presented in figure 1.

Overview of the Norwegian disease-modifying antirheumatic drug (NOR-DMARD) study. Included patients were methotrexate (MTX)-naїve RA patients starting MTX monotherapy (MTX mono) or biologic-naїve RA patients starting TNF-inhibitor+MTX (TNFi+MTX). RA, rheumatoid arthritis; PsA, psoriasis arthritis; AS, ankylosing spondylitis; JIA, juvenile idiopathic arthritis; UA, undifferentiated arthritis; DMARDS, disease-modifying antirheumatic drugs; TNF, tumour necrosis factor.
Patient selection
For the current analyses, we selected patients with RA who were included in the NOR-DMARD study from December 2000 to December 2010 and who were MTX-naïve starting MTX monotherapy (MTX mono) and biologic-naïve starting their first TNFi combined with MTX (TNFi+MTX). Diagnoses are based on the clinical judgement of the treating rheumatologist (ICD-10 codes M05.8, M05.9 and M06.0).
Assessments
Baseline and 6-month assessments were included in the main analyses, while the drug survival analysis was based on 2-year follow-up data. Assessments included 28-swollen joint counts (SJC) and 28-tender joint counts (TJC) performed by rheumatologists or trained research nurses, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), 0–100-mm visual analogue scales (VAS) for physician's assessment of global disease activity and patient's assessment of joint pain, fatigue and global disease activity, and the modified health assessment questionnaire (MHAQ).16 The short form-6 dimensions (SF-6D) was calculated from the medical outcomes study short form health survey (SF-36) and presented as a utility measure (1.0 perfect health).17
The disease activity score 28 (DAS28) with ESR,18 the simplified disease activity index (SDAI)19 and the clinical disease activity index (CDAI)20 were calculated. For each group, we calculated proportions achieving a European League Against Rheumatism (EULAR) good response,21 as well as DAS28 remission (DAS28 <2.6),22 SDAI remission (SDAI ≤3.3),23 CDAI remission (CDAI ≤2.8)24 and the Boolean-based American College of Rheumatology (ACR)/EULAR remission.25
Statistical analysis
For the descriptive analyses, each treatment group was stratified into 2-year intervals according to the date of the baseline visit. Continuous variables are presented as means (SD) if normally and medians (IQR) if non-normally distributed.
Time trends in several baseline variables were assessed by linear regression analysis with year at onset of treatment as the independent variable (continuous 1–10) and the respective baseline variables as dependent variables. CRP, ESR, joint counts and MHAQ were normalised for the linear regression analyses.
Completers at 6 months were included in the analyses of EULAR good response, DAS28 remission, SDAI remission, CDAI remission and ACR/EULAR remission, and time trends of these response rates were analysed by logistic regression analyses with the dichotomised responses as the dependent variables. Response and remission rates were also compared between first and last time periods by χ2 test, and the presented results are limited to this comparison when no linear effects of time were found.
To account for differences in retention to therapy, we calculated LUNDEX values for each response and remission category by the following formula: LUNDEX value=[fraction of starters still in study at time T]×[fraction responding at time T].26 We used the estimated survival rates from the Kaplan–Meier analysis for the calculation of LUNDEX values, and those patients who were lost to follow-up or had missing 6-month visit or outcome data (eg, due to logistical reasons) did not contribute to reduced LUNDEX values.
Mean prednisolone doses and proportions of patients who used prednisolone at baseline and at 6 months were assessed and compared statistically between first versus last time period by using two-sample t test and χ2 test. Possible linear effects of time on prednisolone usage were also assessed by linear and logistic regression with year of treatment start as a continuous variable. Mean doses of MTX were assessed and compared statistically in the same way.
Two-year retention to therapy (drug survival) of MTX (in MTX-naïve patients) and first TNFi+MTX was assessed by the Kaplan–Meier analysis and possible time trends assessed by Cox regression analysis with year as a continuous (1–10) covariate.
Statistical tests were two-sided with level of significance set at 0.05, without correction for multiple comparisons. Statistical analyses were performed using the Predictive Analytics Software program, V.19.0 (SPSS, Chicago, Illinois, USA).
Results
Patient characteristics
From 2000 to 2010, 1866 MTX-naïve RA patients started MTX monotherapy (figure 1). Mean (SD) age was 56.0 (13.7) years, 69.9% were female and 62.0% rheumatoid factor positive. In the same time period, 707 RA patients started their first TNFi+MTX (figure 1). During the decade, an increasing fraction of patients started treatment with etanercept and adalimumab rather than infliximab (data not shown). The mean (SD) age was 52.1 (13.2) years, 70.3% were female and 75.0% rheumatoid factor positive in the TNFi+MTX group. These patient characteristics remained stable during the study years in both groups.
Baseline disease activity
Several measures of disease activity and inflammation in both groups decreased significantly over time. Average baseline DAS28 decreased from high to moderate level of disease activity from 2000 to 2010; in the MTX mono group, from mean (SD) 5.17 (1.26) to 4.75 (1.30); and in the TNFi+MTX group, from mean (SD) 5.88 (1.23) to 4.65 (1.41). SDAI, CDAI, MHAQ, 28-SJC, CRP and ESR were all lower for more recent treatment initiations as compared with in the earlier years (tables 1 and 2). A similar decline was also observed for more subjective markers of disease severity, including pain and patient and physician global assessments, but similar changes over time were not observed for fatigue VAS and SF-6D.
Time trends in demographics and baseline characteristics at start of MTX monotherapy
Time trends in demographics and baseline characteristics at start of first TNFi+MTX
Disease duration
We observed a significant time trend towards initiation of both MTX mono and TNFi+MTX earlier in the disease course (tables 1 and 2). In 2000–2001, the time from diagnosis to initiation of MTX mono was median (25–75 percentile) 10.0 (3.0–96.0) months—and in 2009–2010, the median was 10 days; 0.3 (0–12.8) months. Time from diagnosis to initiation of the first TNFi also decreased significantly during the decade, from median 8.0 (4.0–15.0) years in 2000–2001 to 3.8 (1.3–10.6) years in 2009–2010.
MTX doses
MTX doses increased significantly in both treatment groups during the decade. The mean dose of MTX 6 months after initiation of treatment increased from mean (SD) 12.1 (4.9) to 15.7 (6.5) mg/week (p<0.001) in MTX mono. In the TNFi+MTX group, the mean dose of MTX at initiation of TNFi increased from 9.7 (4.5) to 16.3 (5.7) mg/week (p<0.001) during the decade.
Prednisolone and folic acid
The proportion of patients using co-medication with prednisolone at initiation of MTX monotherapy increased over the years (49.0% in 2000–2002 vs 60.7% in 2009–2010), while the proportion still using prednisolone after 6 months decreased (32.5% in 2000–2002 vs 21.7% in 2009–2010). The differences between the first and the last period were statistically significant, but the effect of time was not linear (table 3). In the TNFi+MTX group, the proportion of patients using prednisolone at baseline was stable during the decade, but the proportion of prednisolone users at 6 months was significantly lower in the last versus the first time period (35.3% vs 14.8%). The mean prednisolone doses at baseline and 6 months among patients who used prednisolone were stable throughout the decade in both groups (table 3). An increasing proportion of patients used folic acid both in the MTX mono and the TNFi+MTX group over the decade (see online supplementary table S3).
Time trends in proportion of patients on prednisolone at baseline and after 6 months and prednisolone dose mg/day
Response and remission rates
A twofold increase in 6-month remission rates was observed in both groups during the decade (figure 2A,B). The 6-month DAS28 remission rate increased in MTX mono from 17.8% in 2000–2001 to 37.6% in 2009–2010 (p<0.001 for both time trend and for first vs last period). An even larger increase from 16.9 to 46.3% was observed in the TNFi+MTX group (p<0.001 for time trend and p=0.001 for first vs last period). There was also a significant time trend showing increasing SDAI, CDAI and ACR/EULAR remission rates at 6 months in both groups, whereas increasing rates of the less stringent outcome EULAR good response were only observed in the MTX mono group (p=0.013 for first vs last period) without any linear effect of time. Time trends and pairwise comparisons of first versus last period are shown in figure 2A,B. Results for response and remission rates were consistent after LUNDEX adjustment (see online supplementary tables S1 and S2).

(A) Time trends 2000–2010 in response and remission rates after 6 months, MTX monotherapy.(B) Time trends 2000–2010 in response and remission rates after 6 months, TNFi+MTX. MTX, methotrexate; TNFi, tumour necrosis factor inhibitor; EULAR, European League Against Rheumatism; ACR, American College of Rheumatology; DAS28, disease activity score 28; SDAI, simplified disease activity index; CDAI, clinical disease activity index.
Drug survival
Two-year drug survival for MTX mono improved over the decade. The highest drug survival rates were observed among those patients initiating treatment in the second part of the decade (figure 3A). The overall time trend (p<0.001) of the HR for treatment discontinuation was statistically significant (figure 3B). Conversely, for the TNFi+MTX group, there was no significant trend for change in drug survival at 2 years during the decade (figure 3C), and difference in 2-year drug survival between the three most frequently prescribed TNFi (infliximab, etanercept and adalimumab) was not statistically significant (data not shown).

{kind=link}
{kind=link}
{kind=link}
(A) Two-year drug survival of MTX monotherapy. Kaplan–Meier plots over 2-year retention to MTX monotherapy, according to year of treatment start. Log-rank test for 2-year drug survival; p<0.001. (B) HR discontinuation of MTX monotherapy within 2 years. Overall time trend p<0.001. Dots represent the HR, and error bars represent the 95% CI of HR. 2001 was used as the reference year (HR=1). The 10 years are divided into three groups of approximately same number of patients to present the overall time trend (p<0.001) for HR of treatment discontinuation. (C) Two-year survival of TNFi+MTX. Kaplan–Meier plots over 2-year retention to first TNFi+MTX therapy, according to year of treatment start. Log-rank test for 2-year drug survival: p=0.268 (not significant). HR, hazard ratio; MTX, methotrexate; TNFi, tumour necrosis factor inhibitor.
Discussion
In this longitudinal observational study, we found a twofold increase in remission rates as well as a consistent improvement in other disease activity measures over the period 2000 to 2010. Importantly, this increase in remission rates was present both for MTX mono and the more expensive combination with TNFi. This improvement over time with a higher proportion of patients achieving accepted targets1 for treatment coincided with a more aggressive treatment approach reflected by lower disease activity levels and shorter disease duration when therapies were initiated.
Some previous register studies have also indicated that lower disease activity at initiation of sDMARD and bDMARD will result in improved remission rates. Hetland et al27 showed that baseline disease activity in the DANBIO register decreased and treatment responses improved in RA patients treated with their first bDMARD in the period 2000 to 2005. Similarly, in a study from the British Society for Rheumatology Biologic Register (BSRBR), Hyrich et al28 showed a time trend towards less severe disease at baseline and improved outcomes in RA patients starting their first TNFi during the period 2001–2008. However, in both these observational studies, the baseline disease activity remained high in contrast to the current study in which the baseline disease activity decreased from high to moderate during the 10-year study period.
In the NOR-DMARD study, the time from diagnosis to initiation of TNFi treatment decreased significantly from 2000 to 2010. In the above-mentioned study from DANBIO, the disease duration remained unchanged in the study period, while in the BSRBR register a significant trend towards use of TNFi in patients with shorter disease duration was also observed, although mean disease duration remained as long as 11.4 years in 2008.28 We found that time from diagnosis to initiation of MTX monotherapy decreased significantly from median 10 months to median 10 days during the decade. Several studies have shown that all therapies—sDMARD monotherapy, sDMARD combinations and bDMARDs—seem to work better in early disease than in established RA.29–31 Results from meta-analysis support that disease duration at the time of DMARD initiation was the main negative predictor of response to DMARD treatment.32 Timing the ‘window of opportunity’ is important,33 and it has been shown that ACPA-positive RA patients with symptoms <12 weeks have less progressive disease than patients with a longer symptom duration.34 Initiation of sDMARD treatment as soon as the diagnosis of RA is made is in concordance with both the EULAR and the ACR treatment recommendations.1 ,3
In this study, the diagnosis of RA was based on the clinical judgement of the treating rheumatologists, which may result in initiation of DMARD before the patients fulfilled the 1987 criteria of RA. During this study period, the recent ACR/EULAR 2010 criteria for RA were not in use, and it has been shown that the new criteria can support earlier classification of RA and even earlier initiation of sDMARDs in RA.35
Sokka et al36 showed increasing use of MTX in several countries since the 1980s. A similar evolution has also occurred in Norway and was observed in the NOR-DMARD from 2000 to 2009 (data not shown). We also found a significant increase in doses of MTX during the 10-year study period in both the MTX mono and the TNFi+MTX groups. Recent recommendations have also advocated that MTX should be used in higher doses than was previously practiced.37 An increase in the dose of MTX was also found by Hetland et al27 with an increase to higher MTX doses than was observed in our study. It is well documented that higher weekly doses (20–30 mg) are more effective than lower doses (7.5–15 mg).1 ,37 ,38 Interestingly, we also found a significant time trend for better drug survival of MTX monotherapy during the decade despite increased availability of TNFi treatment, which probably reflects a real improved efficacy of MTX with higher doses and earlier initiation, as well as fewer discontinuations due to non-serious adverse events (see online supplementary figure S1A–C). Clinicians and patients have become increasingly aware of the importance of MTX as an anchor drug in early RA.39 However, the efficacy of combinations of MTX and other sDMARDs versus MTX mono is still under debate and investigation.40–42 However, in the 2013 updated EULAR recommendations for management of RA, MTX monotherapy and MTX combined with other sDMARD are equal as initial treatment in DMARD-naïve patients.15
In our study, a higher proportion of RA patients used prednisolone when starting MTX in the recent years, and an increasing proportion of patients tapered and discontinued prednisolone. This practice is in accordance with EULAR recommendations on the use of glucocorticosteroids in RA.43 More aggressive use of glucocorticosteroids is advantageous, especially for bridging the interval between initiation of DMARDs and onset of their therapeutic effect.44 Available evidence also supports that low-dose or step-down glucocorticosteroids given in addition to standard DMARD treatment can slow radiographic progression significantly in early RA.45 ,46
A higher proportion of RA patients used folic acid when starting MTX and TNFi+MTX in the latter part of the study period. Hoekstra et al47 have previously found folic acid supplementation and, to a lesser extent, prednisolone to be associated with better drug survival for MTX.
Drug survival for the first TNFi+MTX was largely unaffected by the year of treatment initiation, as also observed by Hetland et al27 in DANBIO. This finding, despite the observed increase in response and remission rates, is probably due to an increasing number of available bDMARDs during the recent years, which allow patients to change to an alternative bDMARD when they have a partial response to their ongoing regimen. This increased switching practice also seems to be reflected in our data as we found an increased frequency of discontinuations due to lack of efficacy during the period 2007–2010 compared with earlier periods (data not shown). The access to switching to other bDMARDs in situations with inadequate response or adverse events is currently not restricted in Norway. However, tight control and ‘treat to target’ strategies were not fully implemented in the study period, but the focus on earlier switching has increased during recent years if the predefined treatment target is not achieved within 3–6 months.2
Radiographic data are not systematically assessed in the NOR-DMARD study, but the proportion of patients with erosive disease at baseline is recorded, and during the study period this proportion decreased in the TNFi+MTX group but not in the MTX group. Radiographic damage is associated to level of physical function, particularly in established disease,48 and baseline MHAQ score also improved during the decade.
The main response and remission data are presented for completers (figure 2A,B); however, results were consistent after LUNDEX correction (see online supplementary tables S1 and S2). The opportunity for liberal access and application of bDMARDs in Norway may reduce the generalisability of our findings to other countries with stricter criteria for initiating bDMARDs. However, the twofold increase in remission rates for MTX mono illustrates that good treatment results also can be achieved with cheap drugs if they are used early according to updated treatment recommendations.
The limitations of this study include lack of systematically assessed radiographic data, incomplete information about fulfilment of individual items in the 1987 RA classification criteria and missing information about symptom duration (first symptom attributed to RA or first reported joint swelling). However, universal agreement on how to define disease onset and therefore disease duration does not exist.33 The strength of our observational study is related to its real-life setting. When treatment is initiated at moderate rather than high disease activity, it is likely that remission is more frequently achieved. However, regardless of this circularity, our results support that earlier and more aggressive treatment will lead to more frequent achievement of remission, the agreed treatment target for RA.1 ,3 Further, our data were robust as better results with time were consistent across a variety of endpoints.
These real-life data from the NOR-DMARD study showed that during the period 2000–2010 rheumatologists adopted a more aggressive treatment approach with earlier use of both sDMARD and bDMARD and with treatment initiation at lower levels of disease activity. Remission was more frequently achieved with this more aggressive approach. These observations should be considered by payers and decision makers involved in issuing recommendations for use of DMARDs in RA. In summary, modern early and aggressive treatment approaches seem to have led to better short-term outcomes and will hopefully also lead to better long-term outcomes for patients with RA.
Acknowledgments
The authors thank the patients for participating in this study and the local rheumatology staff for data collection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
- Data supplement 2 - Online tables
Footnotes
-
Handling editor Hans WJ Bijlsma
-
Contributors TKK, EL and EAH were responsible for study design.AW, SK, ER, KM and A-BA were responsible for data acquisition. A-BA, EL and ICO were responsible for data analysis. A-BA, EL, TU, TKK and EAH were responsible for manuscript preparation. All authors approved the final manuscript.
-
Funding This work was supported by the Norwegian Women's Public Health Association by a PhD grant to the first author. The NOR-DMARD study has previously received grant support from AbbVie, Amgen, Wyeth/Pfizer, Aventis, MSD, Schering-Plough/Centocor, Bristol-Myers Squibb, UCB, Roche and the Norwegian Directorate for Health and Social Affairs.
-
Competing interests A-BA has received honoraria as speaker and/or consultant from AbbVie, MSD/Schering-Plough and UCB. EL has received honoraria as speaker and/or consultant from AbbVie, Bristol-Myers Squibb, Hospira, Pfizer, Roche and UCB. TU has received has received consulting and/or speaker honoraria from AbbVie, Bristol-Myers Squibb, MSD, Pfizer, Roche and UCB. ICO, AW, SK, ER and KM: none declared. TKK has received honoraria as speaker and/or consultant from AbbVie, Bristol-Myers Squibb, MSD/Schering-Plough, Pfizer/Wyeth, Roche, UCB, Celltrion, Orion Pharma and Hospira. EAH has received honoraria as speaker and/or consultant and/or investigator research grants from AbbVie, Pfizer/Wyeth, MSD/Schering-Plough, Roche, Bristol-Myers Squibb and UCB.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the regional ethics committee and by the Data Inspectorate. Patients gave written consent before participation.
-
Provenance and peer review Not commissioned; externally peer reviewed.