Article Text

Abstract
Background: Randomised controlled trials have shown that treatment with anti-tumour necrosis factor (anti-TNF) agents is effective in refractory rheumatoid arthritis (RA).
Objective: To determine the effectiveness of anti-TNF in a general unselected group of patients with refractory RA.
Methods: 68 patients with active RA despite treatment with disease modifying antirheumatic drugs were studied during 12 infliximab infusions. Infliximab (3 mg/kg/infusion) was given every 8 or 6 weeks. Clinical efficacy was assessed by the Disease Activity Score (DAS) index (44 joints). Dose adjustments were based on residual disease activity (DAS score >2.4). The primary end points were the percentage of patients achieving good or moderate response by the EULAR response criteria and the proportion of patients requiring dose adjustment.
Results: 20 (29%) patients discontinued treatment owing to side effects, early inefficacy, or other considerations. Among the patients who continued treatment, 27 (56%) and 32 (67%) were responders on the 6th and 12th infliximab infusion, respectively. In the same patients, disease activity gradually improved without modifications in the initial dosing in 10 (21%), whereas in 38 (79%) the dose of infliximab and/or methotrexate was increased. Intensification of treatment led to a significant decrease in the mean DAS score in this group (from 5.27 just before dose modification to 4.54 before the 12th infusion, p<0.002). The EULAR response category improved in only 10/38 (26%), however.
Conclusions: In this initial observational study of patients with RA treated with recommended doses of infliximab, adjustments in treatment were common but not always sufficient to maintain adequate disease control. Longitudinal controlled trials are needed to define the optimal dose escalation in patients with suboptimal response.
- rheumatoid arthritis
- infliximab
- Disease Activity Score
- EULAR response criteria
- ACR, American College of Rheumatology
- CRP, C reactive protein
- DAS, Disease Activity Score
- DMARD, disease modifying antirheumatic drug
- ESR, erythrocyte sedimentation rate
- HAQ, Health Assessment Questionnaire
- PPD, purified protein derivative
- RA, rheumatoid arthritis
- RCT, randomised controlled trial
- TB, tuberculosis
- TNFα, tumour necrosis factor α
- VAS, visual analogue scale
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- CRP, C reactive protein
- DAS, Disease Activity Score
- DMARD, disease modifying antirheumatic drug
- ESR, erythrocyte sedimentation rate
- HAQ, Health Assessment Questionnaire
- PPD, purified protein derivative
- RA, rheumatoid arthritis
- RCT, randomised controlled trial
- TB, tuberculosis
- TNFα, tumour necrosis factor α
- VAS, visual analogue scale
Rheumatoid arthritis (RA) is a chronic inflammatory arthropathy of substantial social and financial cost, and may reduce survival.1 Treatment of RA has changed following the clinical use of biologic therapies. Strategies that selectively target tumour necrosis factor α (TNFα) have shown efficacy when tested in patients with considerable disease activity despite treatment with disease modifying antirheumatic drugs (DMARDs).2–4
Infliximab is a chimeric monoclonal antibody that specifically binds both soluble and membrane bound TNFα. It was the first anti-TNFα antibody that was clinically assessed for patients with RA. Several well designed randomised clinical trials (RCTs) have shown that infliximab has adequate clinical efficacy and an acceptable side effect profile.5–8 Although the recommended dosing schedule for infliximab is at the lower end of doses that were evaluated in clinical studies, in the same studies higher doses and/or more frequent dosing suggested a potential for additional improvement.2 Based on these results and clinical experience, in May of 2002 a consensus statement on biological agents for treatment of RA stated that “in patients with an incomplete response, observations suggest that increasing the dose or reducing the dosing intervals may provide additional benefit, as may the addition or substitution of other DMARDs or other biological agents”.9 Although this is a sensible approach, its usefulness and the optimal escalation of treatment are not known.
Data from an RCT are of paramount importance to determine clinical efficacy of new treatments, but they have limitations related to their applicability in a general, unselected population.10 Observational studies and clinical protocols provide useful additional information about long term outcomes and side effects. Herein, we report our experience with the use of infliximab in patients with RA. More specifically, we report the long term efficacy, treatment failures, toxicity, and the application of validated tools for assessment of disease activity to modify treatment and the effect of treatment modification.
METHODS
Patients and treatment
Patients followed up by two rheumatology referral clinics (one in northern and the other in southern Greece) were included in this uncontrolled, open label study. They were recruited over a period of about 20 months and received infliximab because of considerable disease activity (Disease Activity Score (DAS) >3.7). Neither an upper limit for the steroid dose nor any limit for the current DMARDs was applied. Patients received infliximab in the recommended dose of 3 mg/kg during weeks 0, 2, 6, and thereafter every 8 or 6 weeks depending on individual response (see below) and were subsequently followed up for 12 infliximab infusions.
Patient evaluation
Patients were evaluated clinically at baseline and before each infusion. Routine laboratory tests such as complete blood count, erythrocyte sedimentation rate (ESR), C reactive protein (CRP), blood urea nitrogen, creatinine, liver function tests, and urine analysis were performed. A chest radiograph was performed on study enrolment. Patients recruited after November 2000 also had a skin test with purified protein derivative (PPD).
Assessment of disease activity
Disease activity was evaluated at study enrolment and before each of the 3rd to the 12th infliximab infusion using the following indexes: Ritchie articular index for tender joints, swollen joint count (44), visual analogue scale (VAS) for pain (0–10), VAS for patient’s global assessment, doctor’s global assessment on a Likert scale (1–5), and Health Assessment Questionnaire (HAQ). We applied the original DAS based on four variables (the Ritchie index, the 44 swollen joint count, the patient’s assessment of disease activity, and the ESR) to assess disease activity on each visit. Response to treatment was assessed by the EULAR response criteria. According to these criteria patients were characterised as good, moderate, or non-responders based on both the DAS level attained and the change in DAS.11 Good response was defined as >1.2 improvement in the DAS from baseline and a DAS attained during follow up of ⩽2.4. Non-responders were patients with an improvement of ⩽0.6 or patients with an improvement of >0.6 but ⩽1.2 and a DAS attained during follow up of >3.7. The remaining patients were classified as moderate responders.
Primary end points
The primary end points included the proportion of patients who achieved good and moderate response after 12 infliximab infusions as well as the proportion of patients requiring dose adjustment.
Adjustment in treatment
Treatment modification (increase in the methotrexate dose or shortening the interval between infliximab infusions) to control disease activity was based predominantly on DAS at every visit (cut off point for low disease activity DAS ⩽2.4) and, in rare cases, on practical considerations, such as difficult access to the hospital or lack of insurance coverage. When adequate disease control was achieved corticosteroids were tapered. Treatment withdrawals were classified as withdrawals due to inefficacy, adverse reaction, or other cause.
Statistical analysis
Statistical evaluation within group was done by the use of paired Student’s t test. Rate differences between groups were analysed by the χ2 test, while comparison between groups was done by the Mann-Whitney test. A p value <0.05 (two tailed) was considered as significant.
RESULTS
Patients’ demographics and disease characteristics
A total of 68 patients received infliximab. Most had longstanding RA (mean disease duration 10.7 years; table 1), failed multiple DMARDs, and had functional status ranging from I to III according to the revised American College of Rheumatology (ACR) criteria.12 At study entry all but five patients (93%) had a high level of disease activity (DAS >3.7). Consistent with that was the high number of swollen joints (mean (SD) 19.7 (11.3)) as well as the high Ritchie articular index score (mean (SD) 28.1 (14.3)).
Baseline characteristics of patients (n = 68)
Most patients received methotrexate before infliximab treatment either as monotherapy or in combination with different DMARDs. The majority of the patients (55/68, 81%) continued methotrexate upon study enrolment but discontinued other DMARDs. Six patients had contraindication to the use of methotrexate and received another DMARD (hydroxychloroquine (four), cyclosporin A (one), and hydroxychloroquine in combination with sulfasalazine (one)), while seven received monotherapy with infliximab. The majority of patients (41/68, 60%) on study enrolment received corticosteroids, with a mean (SD) dose of 9.1 (4.5) mg/day. Patients were followed up for up to 12 infliximab infusions. Because of modifications in the infliximab scheme the mean treatment duration was 72.6 weeks (range 54–78).
Withdrawals
Overall, 20 (29%) patients discontinued treatment (table 2). All but two discontinuations (90%) occurred during the first six infliximab infusions. The single late discontinuation was at the 10th infusion because of marked lympocytosis. All patients who discontinued treatment because of inefficacy had considerable disease activity with a DAS score of at least 3.7 and no improvement in any of the patient oriented or physician measures. All five patients who discontinued treatment because of inefficacy received no modification to the dose or scheme of treatment before discontinuation. This was because experience with infliximab treatment was limited during the first months of its clinical application. An additional four patients discontinued because of concurrent infection. Two of them had tuberculosis (TB), one lethal miliary TB and the other extrapulmonary TB with cervical lymph node involvement. Another patient after 60 weeks of treatment was diagnosed as having possible TB arteritis of the subclavian artery. The fourth patient had a severe pneumonia of possibly infectious aetiology. Two patients, both receiving monotherapy with infliximab, discontinued because of serious allergic reactions, one on the 5th and the other on the 6th infliximab infusion. All subsequent data analysis for efficacy and treatment modification are for the 48 patients who completed 12 infliximab infusions.
Withdrawals from the infliximab treatment
Efficacy
Efficacy was maintained through the treatment period with no statistically significant differences between the 6th and 12th infusion for the three categories of response (good, moderate, and no response). The percentage of responders (good plus moderate) at the 6th and 12th infusion was 56% and 67% respectively (fig 1). All clinical parameters were significantly improved for those patients who completed the study (fig 2). However, only nine (19%) patients could satisfy the remission cut off criterion (DAS <1.6) at least once during the treatment period and only three patients at the 12th infusion. Moreover, only 23% of the patients had DAS scores <2.4 (low disease activity cut off limit) at the12th infusion.
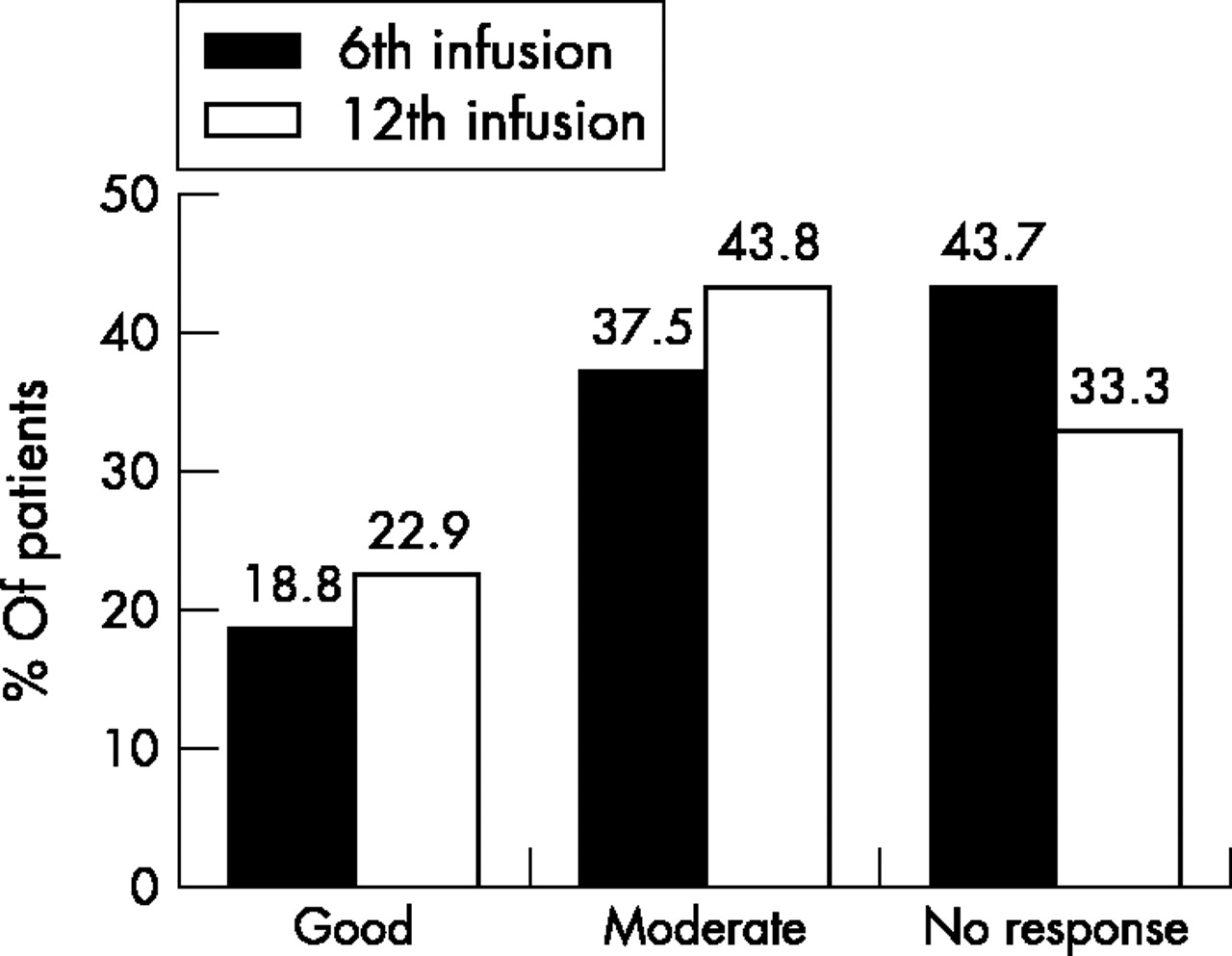
Response rates at the 6th and 12th infusions of infliximab according to EULAR response criteria (% of patients).

Improvement in clinical parameters (n = 48). *p<0.001; **p<0.002.
The mean corticosteroid dose for those patients who completed 12 infusions decreased from 8.6 mg/day at study entry to 7.1 and 6.0 mg/day at the 6th and 12th infusion, respectively (p<0.05 between study entry and both the 6th and 12th infusions), while 30% (9/30) were able to discontinue steroids (table 3).
Dose adjustment during treatment for those patients who completed 12 infliximab infusions
Dose adjustments
Adjustment in the infliximab scheme or methotrexate was done in the majority of the patients as outlined in “Methods”. Among the patients receiving methotrexate, the dose of methotrexate was increased in 20%; the mean dose increased from 13.2 to 14.2 mg/wk between the 1st and 12th infusion, respectively (table 3). The frequency of infliximab infusions was increased to at least every 6 weeks in 73% of patients. The mean time point of infliximab dosing adjustment was the 8th infusion (4th to 11th; fig 3). In contrast, in 10 (21%) patients adequate clinical response was achieved and in this group neither methotrexate nor infliximab doses were increased. When differences at baseline characteristics between the stable treatment group (21%) and the dose adjustment group were assessed, it was shown that the mean DAS in the latter was significantly higher than in the first group (6.05 v 4.57, p<0.01; fig 3). No differences were detected in age, disease duration, sex, methotrexate, or corticosteroid dosages between these two groups.

Mean DAS over time for each group of patients: the first with stable treatment (n = 10) and the second with treatment modification (n = 38).
Response to dose adjustment
In total, either methotrexate or infliximab dosing were modified in 38/48 (79%) patients. The mean DAS for this group of patients significantly improved after treatment modification from 5.27 just before dose modification to 4.54 before the 12th infusion (p<0.002; fig 3). After either treatment modification the EULAR response category was improved in 10 (26%) of these 38 patients, remained the same in 23 (61%), and worsened in 5 (13%) (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in EULAR response categories after treatment adjustments (n = 38).
DISCUSSION
RCTs are the “gold standard” for assessing clinical efficacy of a therapeutic intervention. However, application of these types of study to a chronic disease like RA has several limitations10 as a significant number of patients seen in routine care do not meet the criteria for inclusion, thus limiting the applicability of results in a limited number of patients. Long term observational studies and clinical protocols are of great value for obtaining data about effectiveness and long term prognosis of patients with RA.13 We consider that data presented as in this study are useful for a better and more reliable assessment of clinical results of recently developed therapeutic interventions for RA.
Although the size of the cohort was modest, we believe this is a group representative of a “real life” clinical practice. Thus, most of the patients had longstanding RA (mean disease duration 10.7 years) with multiple DMARD failure (mean 2.6) and considerable disease activity (mean DAS 5.4, with 93% of the patients having a DAS >3.7). Their high disease activity is indicated by the fact that the majority of them received corticosteroids at a mean dose of 9.1 mg/day, which is more than the accepted dose for long term use in patients with RA. Two patients developed TB with an additional possible TB arteritis. A baseline PPD skin test was not available in these three patients. After recognition of the potential for reactivation of TB, a PPD skin test was performed in all patients subsequently enrolled.
The ACR response criteria were originally developed to discriminate between active treatment and placebo and are used mainly in RCTs.14 We applied the DAS because we were also interested in actual disease activity status, an important consideration in clinical practice. Applying the EULAR response criteria we found that treatment effectiveness was sustained throughout the treatment period. The percentage of patients who were responders (good or moderate) was not significantly different between the 6th and 12th infusions (56% and 67% at the 6th and 12th infusion, respectively; fig 1). In agreement with previous experience, significant residual disease activity remained, even for responders (mean DAS of good and moderate responders at the 12th infusion 3.01). Moreover, only nine (19%) patients entered remission (DAS <1.6) at some time during treatment and three (6%) of them just before the 12th infliximab infusion.
Because the ACR20 response criteria correspond roughly with the sum of good and moderate responders, response rates for our patients are comparable with response rates from clinical trials and with a registry reported recently from Sweden.15 Moreover, our treatment survival was around 70%, which is also similar to that reported recently from the Swedish registry. However, the data on efficacy in this study have to be interpreted with caution. Because this was an open label study, we cannot completely rule out the possibility that a placebo effect or regression to the mean might have influenced the response rates. However, the long duration of the study makes it unlikely that either of these had a substantial effect on the analysis (because the placebo effect usually declines with time), and regression to the mean would have a similar effect on both groups.
Two groups of patients can be distinguished based on treatment efficacy and subsequent need for an increase of either methotrexate or infliximab (fig 3). About 20% of the patients improved gradually and there was no need for modification in treatment schedule. This group of patients had significantly lower disease activity at the beginning than the second group (DAS 4.57 v 6.05, p<0.05), while no significant differences in either methotrexate or corticosteroid doses were detected between them. However, the majority of patients required dose modification at some point (4th to 11th, mean 8th infliximab infusion) to control disease activity. Although DAS in this group improved significantly between baseline and the 12th infusion (from 6.05 to 4.54, p<0.001), they had more active disease than the first group at all times during the treatment period (6th, 8th, and 12th infliximab infusion, p<0.01 between groups).
Comparison of response rates just before treatment adjustment and before the 12th infliximab infusion showed that the majority of the patients remained at the same response category and only 26% improved response status (fig 4). It might be argued that the modifications of infliximab and/or methotrexate were not aggressive enough to improve optimally the disease activity level as assessed by the DAS index, or that disease in these patients is not strictly ΤΝFα dependent.
The immunogenicity of infliximab has been recently assessed in patients with Crohn’s disease treated with infliximab.16 The authors concluded that concomitant immunosuppression prevents the formation of antibodies against infliximab, reducing the incidence of allergic reactions and increasing the duration of response. Thus, in patients with RA methotrexate acts both as a DMARD and by reducing infliximab immunogenicity. The finding in the present cohort that treatment modification is needed in the majority of the patients can be attributed to either a “low dose” infliximab scheme (3 mg/kg) or to an inadequate suppression of infliximab immunogenicity by methotrexate “low dosing” regimen (mean dose 13.2 mg/week, lower than the 15 mg/week in the aforementioned study).
Den Broeder et al recently published their successful experience of dose titration with adalimumab, a human monoclonal anti-TNFα antibody, applying DAS28 to monitor disease activity.17 Our data support this approach of close monitoring of disease activity and subsequent dose adjustment, especially when recently developed and expensive agents like biological agents are used. To this end, efforts to develop a “physician friendly” Simple Disease Activity Index (SDAI) that retains the sensitivity assessment characteristics of the DAS and ACR response criteria, but is at the same time an easy way to assess disease activity in daily practice, are certainly useful.18
The goal of treatment of RA is to control inflammation, and regular disease activity monitoring is needed for clinical decision making. TNFα antagonists are potent and expensive drugs and their use in clinical practice requires close monitoring and application of validated tools such as the EULAR response criteria, which assesses both functional capacity and progression of joint damage,19 may facilitate this task.20
Acknowledgments
This work was supported—in part—by an unrestricted grant from Schering Plough of Greece.
The authors thank Dr Marinela Mamoulaki, Panagiota Siaka, Giasna Kakavouli, Maria Kasapaki, RN, Sofia Sfakianaki, RN, and the nursing staff of the rheumatology clinics for patient care, and Dr Gabor Illei for critical review of the manuscript.