Article Text

Abstract
Objective: To investigate whether coronary flow reserve (CFR), measured by a new non-invasive method, is impaired early in patients with systemic sclerosis (SSc) and whether CFR impairment correlates with clinical or functional measures, or both.
Methods: 27 patients with SSc without clinical evidence of ischaemic heart disease and 23 control group subjects matched for age and sex were studied. CFR was evaluated in the left anterior descending coronary artery (LAD) with a new non-invasive method: contrast (Levovist) enhanced transthoracic Doppler during adenosine infusion. The pulsed wave Doppler examination of blood flow velocity was recorded in the LAD at rest and after maximum vasodilatation by adenosine infusion.
Results: In patients with SSc, without clinical evidence of ischaemic heart disease, CFR was impaired (p=0.0001). 14/27 patients with SSc had severe reduction of the CFR (⩽2.5) compared with controls (p=0.002). A non-significant trend between mean CFR and the severity and duration of the disease was also seen.
Conclusions: CFR is often reduced in patients with SSc, suggesting early preclinical cardiac involvement in SSc. This impairment in coronary microvasculature is detectable by a non-invasive echocardiographic method and in this study was more common in the diffuse form of SSc.
- coronary flow reserve
- echo contrast
- systemic sclerosis
- CAD, coronary artery disease
- CFR, coronary flow reserve
- dcSSc, diffuse cutaneous systemic sclerosis
- LAD, left anterior descending coronary artery
- lcSSc, limited cutaneous systemic sclerosis
- SSc, systemic sclerosis
Statistics from Altmetric.com
- CAD, coronary artery disease
- CFR, coronary flow reserve
- dcSSc, diffuse cutaneous systemic sclerosis
- LAD, left anterior descending coronary artery
- lcSSc, limited cutaneous systemic sclerosis
- SSc, systemic sclerosis
Cardiac disease is a common finding in systemic sclerosis (SSc) but often clinically occult: clinical evidence of myocardial disease may be found in 20–25% of patients with SSc,1 while at postmortem examination the heart is affected in up to 80% of patients.2 Cardiac lesions of patients with SSc range from focal myocardial involvement to diffuse fibrotic replacement of both ventricles, without coronary artery disease (CAD).3 The pathogenesis of the cardiac lesions in SSc is controversial, but the primary disorder of microvasculature with diffuse arteriolar and capillary lesions seems to precede the fibrosis. Manifestations of myocardial involvement in SSc are usually those of congestive heart failure and arrhythmias; angina, myocardial infarction, and sudden death in the absence of epicardial CAD have also been described.4 Cardiac involvement in SSc, when clinically evident, is associated with a poor prognosis, with a two year mortality rate of about 60% and a five year mortality rate of 75%.5 Therefore, early and accurate identification of cardiac involvement is of paramount clinical importance.
Coronary flow reserve (CFR) assessment is commonly used to evaluate the effects of epicardial coronary stenosis6 on coronary microvasculature and myocardial perfusion. CFR, however, may be impaired, not only in patients with angiographically documented CAD but also in patients with microvasculature dysfunction of different origin. In these patients without significant stenosis, CFR reflects the functional capacity of the microcirculation to adapt to the blood demand during increased cardiac work.7
CFR is usually measured with different diagnostic techniques which are either invasive or very expensive and not serially repeatable.8,9 Some of us have recently developed and validated a new non-invasive method that allows serial evaluation of the CFR.10,11 This method involves advanced ultrasound technology (second harmonic) and intravenous infusion of an ultrasound contrast agent. In this study we have used this new method to evaluate CFR in patients with SSc and no clinical manifestation of ischaemic cardiac disease, proposing that CFR is impaired early in patients with SSc even in the absence of symptoms and/or diagnostic findings suggestive of cardiac disease.
PATIENTS AND METHODS
Patients
Thirty two consecutive patients (28 female, 4 male), classified as having a diffuse cutaneous SSc (dcSSc) or limited cutaneous SSc (lcSSc) according to the preliminary American College of Rheumatology criteria for SSc,12 were studied. Five patients were excluded from the study because they also had left ventricular hypertrophy at M mode echocardiography. Thus, only 27 patients with SSc (16 with dcSSc, 11 with lcSSc) were analysed. None of the 27 patients analysed in this study had signs of congestive heart failure, chest pain, dyspnoea, or palpitation. Their mean (SD) age was 49.2 (13) years (range 21–71) and their disease duration ranged from 6 to 350 months (mean (SD) 92 (91.2) months). All patients underwent serological tests, chest x ray examination, ECG, M mode and two dimensional echocardiography, and pulsed wave Doppler examination to evaluate cardiac chamber and valve morphology and function. Raynaud’s phenomenon was present in 22/27 patients; drugs containing methylxanthine and beverages were forbidden 48 hours before the study. The control group included 23 consecutive subjects matched for age and sex (9 male, 13 female; age 48 (8.3)) with no clinical evidence of heart disease and very low probability of CAD, as assessed by the routine screening procedure commonly used in our institution. Only two subjects had a history of mild hypertension and 16 had hypercholesterolaemia, but all subjects had a normal rest and stress electrocardiogram. The study was approved by the local ethics committee, and all patients gave their informed consent.
Methods
Echocardiography was performed both before and after intravenous echocontrast infusion with an Acuson Sequoia ultrasound unit (C256 echocardiography system, Acuson Corporation) using a broadband transducer with second harmonic capability (3V2c). A complete M mode, two dimensional echo Doppler (spectral and colour) study was performed in all patients. When possible the systolic right ventricular pressure was also measured to exclude patients with moderate to severe pulmonary hypertension (right ventricular systolic pressure >40 mm Hg). All evaluations were performed by the same cardiologist, who was unaware of the clinical data. Inter- and intraobserver variability in assessing the CFR was 3.0% and 3.2%, respectively.
Once the routine echo Doppler examination was completed, the CFR was evaluated using a contrast enhanced transthoracic Doppler examination before and after adenosine infusion. The method has been previously described in detail.10,11 Briefly, to measure coronary flow velocity, colour coded flow imaging was first attained, and then PW Doppler recording was obtained using colour flow as a guide. The spectral trace of coronary flow velocity was characterised by a biphasic flow with a prevalent diastolic component (fig 1A). The Doppler signal contrast enhancer used in this study was Levovist (Schering AG, Berlin)—a suspension of monosaccharide (galactose) microparticles in sterile water. The ultrasound contrast agent was infused with a controlled infusion pump (IVAC P4000 anaesthesia syringe pump) at a concentration of 300 mg/ml with an infusion rate of 1 mg/min (range 0.5–2 ml/min). Contrast administration was carried out both before and during adenosine intravenous administration. The coronary flow was measured at baseline and during adenosine induced coronary hyperaemia. Adenosine was infused at a rate of 140 μg/kg/min in five minutes. The CFR in the left anterior descending coronary artery (LAD) was calculated as the ratio of peak diastolic velocity during hyperaemia to peak diastolic velocity at rest (for each parameter the highest three measurements were averaged) (fig 1B). All studies were continuously recorded on a half inch S-VHS videotape.

(A) In the upper part of the figure a tomographic plane of a modified two chamber view is shown (at the left). Colour Doppler flow mapping in the distal portion of the LAD during contrast enhancement is shown (at the right). In the lower part, spectral Doppler tracing by sampling in the distal LAD at baseline and after adenosine intravenous injection is seen. A biphasic flow with a prevalent diastolic component is clearly detectable. LAD, left anterior descending coronary artery; LV, left ventricle; MV, mitral valve; LA, left atrium; SVC, superior vena cava; RA, right atrium; AO, aorta; RV, right ventricle; CFR, coronary flow reserve. (B) An example of a control group patient with normal CFR (upper section) and a sclerodermic patient with abnormal CFR (lower section). Enhanced transthoracic spectral Doppler flow at baseline (left) and during hyperaemia (right) are seen in both sections.
Statistical analysis
Mean values and standard deviation were calculated for each variable. Continuous data from the two groups were compared by a t test for unpaired data. Bonferroni’s correction was applied as appropriate for repeated tests. Values of p<0.05 were considered significant. Categorical data were evaluated by χ2 test.
RESULTS
Table 1 shows the M mode and two dimensional echocardiography haemodynamic measures determined. In addition, the peak diastolic velocity in the LAD at rest was determined showing no significant differences between the patients with SSc (34.74 (11.74)) and the control group (32. 6 (12.6)).
Echocardiographic and haemodynamic parameters of patients with systemic sclerosis and control group patients
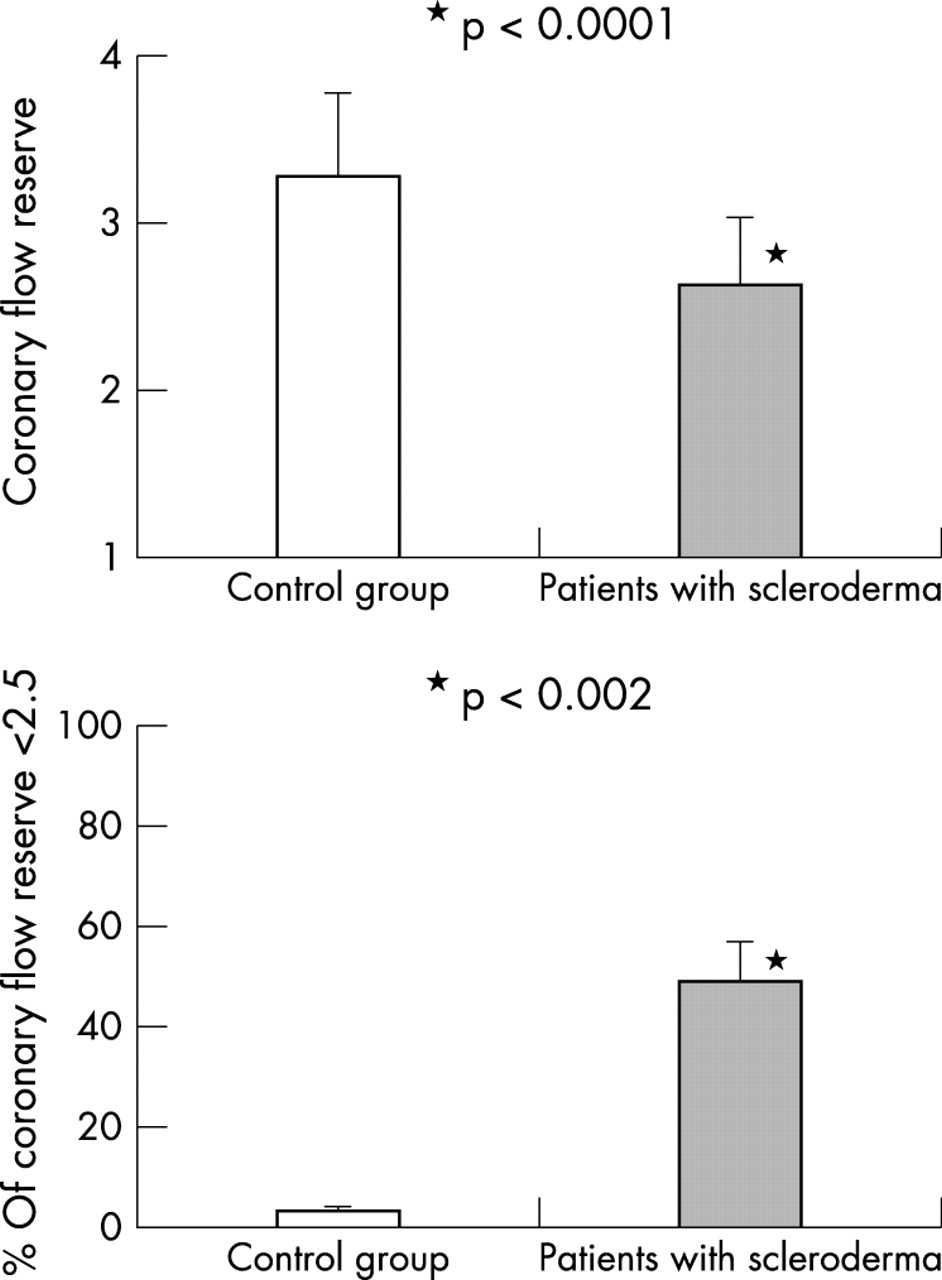
The CFR was significantly lower in the SSc group (2.59 (0.65), range 1.49–3.89) than in the control group (3.38 (0.71), range 2.35–5.64; p<0.0001) (fig 2). A significantly greater number of patients in the SSc group had a CFR ⩽2.5 (14/27 (52%)) as compared with the controls (1/23 (4%), p<0.002). No subject in the control group had a CFR <2.0, which may be assumed as the upper limit of severe reduction, whereas CFR values <2.0 were detected in five patients with SSc (19% v 0%, p<0.001). Four of them had dcSSc and one had lcSSc. Lastly, a trend between CFR and disease duration together with the severity was also noted, but this was not statistically significant for the appropriate multiple group comparisons tests.
{kind=link}
{kind=link}
Histogram illustrating CFR (mean of values) in control group and in patients with systemic sclerosis (upper panel). Histogram illustrating the percentage of CFR <2.5 in the control group and in patients with systemic sclerosis (lower panel).
DISCUSSION
The results of this study show that CFR may be impaired in patients with SSc, even in the absence of clinical signs of cardiac disease. A reduction of CFR in patients with SSc has been already reported by Kahan et al in a small series of patients evaluated invasively who, unlike ours, had symptomatic cardiac disease.13 Other authors have previously shown that in SSc CFR is reduced, but unlike our study, they evaluated patients with an evident scleroderma induced myocardial disease.14 Changes in the CFR depending on haemodynamic differences between the two groups can be excluded because heart rate, left ventricular ejection fraction, and mean aortic pressure did not differ in the two groups either at baseline or after adenosine infusion.
CFR impairment in patients with SSc is likely to indicate an anatomical and/or functional impairment of coronary microvasculature because the presence of structural impairment of small coronary arteries has been frequently demonstrated in these patients in the absence of abnormalities of epicardial coronary arteries.13 Follansbee et al studied 26 patients with SSc, without cardiac symptoms and normal coronary angiograms, and found that 79% of their patients had perfusion defects at thallium-201 scan.14 A support for the “myocardial Raynaud’s phenomenon” hypothesis has been provided by Kahan et al, who found a myocardial perfusion defect in all patients with SSc they evaluated, followed by improvement in perfusion after oral nifedipine administration.15
The results of our study do not allow us to assess whether a vasospastic or structural process impedes flow increase in the small arteries of patients with SSc. In our series coronary angiography was not performed because of the complete absence of symptoms suggestive of CAD; thus, the presence of significant stenosis of a major coronary epicardial vessel cannot be excluded. However, such a possibility is unlikely because of the extremely low probability of CAD in this series and the rare occurrence of significant coronary atherosclerosis previously reported in SSc. The CFR was particularly reduced in patients with dcSSc, indicating that this is a subgroup with an early cardiac involvement. Indeed, a severe reduction of CFR (<2.0) was found especially in patients with dcSSc. Moreover, the disease duration in this subgroup was shorter, so indicating an earlier cardiac involvement.
Probably a larger number of patients are needed to give statistical significance to the trend of CFR progressive impairment according to SSc severity and/or disease duration.
As previously stated, the CFR impairment may be considered to be a preclinical sign of cardiac disease detected in our patients with SSc.
Our study has shown that in patients with SSc, CFR may be impaired even in the absence of any clinical or diagnostic evidence of cardiac disease; furthermore, in these patients CFR is more severely impaired when the diffuse form of SSc is present. Lastly, this study demonstrates the potential usefulness of contrast enhanced transthoracic Doppler examination for the detection of preclinical cardiac involvement in SSc.
In conclusion, impairment of coronary microvasculature can occur in patients with SSc and may be the cause of subsequent primary scleroderma myocardial disease. Thus, early recognition of such an involvement is clinically relevant.