Article Text

Abstract
Objectives: To evaluate the possible effect of androgen status on sexuality and mental wellbeing in patients with primary Sjögren’s syndrome (pSS).
Methods: Serum levels of dehydroepiandrosterone sulphate (DHEA-S), testosterone (T), androstenedione, sex hormone binding globulin (SHBG), and the SHBG/T ratio were measured in 21 women with pSS. Sexual life was assessed by a Swedish version of the McCoy scale, which covers sexual experience and responsiveness during the past 30 days. A standardised questionnaire, the Psychological General Well-Being Index (PGWB), was used to examine quality of life and psychological symptoms in patients with pSS.
Results: Positive correlations were found between DHEA-S serum levels and the total McCoy score (rs=0.62; p<0.01), as well as the subscales of this score reflecting arousal (0.59; p<0.05), desire (rs=0.52; p<0.05), and satisfaction (rs=0.66; p<0.01). Serum DHEA-S concentrations were also related to the total PGWB score (rs=0.60; p<0.01) and subscales of this score: depression (rs=0.62; p<0.01), wellbeing (rs=0.64; p<0.01), general health (rs=0.67; p<0.01), and self control (rs=0.67; p<0.01). Total McCoy and PGWB scores and their subscales were not related to the serum levels of testosterone and androstenedione or the T/SHBG ratio.
Conclusions: Circulating levels of the weak androgen DHEA-S are positively related to the quality of sexual life and mental wellbeing in women with pSS.
- Sjögren’s syndrome
- dehydroepiandrosterone sulphate
- sexual life
- wellbeing
- CNS, central nervous system
- DHEA-S, dehydroepiandrosterone sulphate
- PGWB, Psychological General Well-Being Index
- pSS, primary Sjögren’s syndrome
- SHBG, sex hormone binding globulin
Statistics from Altmetric.com
- CNS, central nervous system
- DHEA-S, dehydroepiandrosterone sulphate
- PGWB, Psychological General Well-Being Index
- pSS, primary Sjögren’s syndrome
- SHBG, sex hormone binding globulin
Primary Sjögren’s syndrome (pSS) is a slowly progressive autoimmune disease primarily affecting the exocrine glands and resulting in mucosal dryness.1 In addition, a wide spectrum of non-exocrine manifestations from various organs—the lungs, kidneys, blood vessels, and muscles—may be seen.2,3 The involvement of the central nervous system (CNS) has been increasingly recognised in patients with pSS during the past decade. The CNS manifestations may sometimes become severe, with symptoms such as hemiparesis, encephalopathy, and dementia.4–7 Some investigators have also reported frequent psychiatric symptoms in pSS, including a high incidence of sleep disturbance.4,8 We recently reported that depression and anxiety were the dominant neuropsychiatric manifestations in patients with pSS and that their mental wellbeing was significantly reduced compared with controls.9,10 The decrease in wellbeing was particularly experienced by those women with pSS who were receiving oestrogen therapy. Primary Sjögren’s syndrome mainly affects women during the fourth and fifth decades of life with a female:male ratio of 9:1,11 further suggesting that sex hormones play a part in the development and/or pathophysiology of the disease.
In recent years, attention has been drawn to the influence of androgens and in particular dehydroepiandrosterone (DHEA) and its sulphated metabolite DHEA-S on autoimmune diseases.12–15 DHEA and DHEA-S are weak androgens which are secreted by the adrenal glands in response to adrenocorticotrophic hormone.16 The possible influence of androgens in pSS has been studied in animal models.17–19 The results indicate that androgen administration strongly suppresses the inflammatory reaction in the female mouse model of Sjögren’s syndrome. We have recently also found reduced serum concentrations of these hormones in women with pSS, both at rest and after adrenal stimulation.20 In the present study we raised the question of whether or not reduced circulating levels of androgens are linked to the increased incidence of neuropsychiatric manifestations and the impaired quality of life seen in women with pSS.
PATIENTS AND METHODS
Patients
Twenty one female patients (mean age 56, range 39–73 years) with pSS according to the preliminary European Community guidelines21 were included in the study. The patients included also fulfilled the Copenhagen criteria.22 The patients were recruited from a database of the hospital. All the patients who fulfilled the diagnostic criteria agreed to take part in the study. Each patient therefore had keratoconjunctivitis sicca demonstrated by the pathological Schirmer-I test (<5 mm/5 min) and/or a short break-up time (<10 sec) and/or positive rose bengal staining (at least two of three tests abnormal); xerostomia was demonstrated by a total stimulated salivary gland secretion rate of <0.1 ml/min and/or abnormal lower lip glandular biopsy and/or pathological salivary gland scintigraphy (at least two of three tests abnormal). The patients were investigated at the outpatient clinic at the Department of Rheumatology, University Hospital of Uppsala.
The onset of the disease occurred 1–15 years (mean four years) before the study. Eight patients had non-exocrine manifestations: Raynaud’s phenomenon (n=5), non-erosive arthritis (n=2), and sun sensitivity (n=3). No patient was treated with disease modifying drugs, apart from one who was treated with hydroxychloroquine. Seven patients were receiving oestrogen treatment and 14 were postmenopausal. Fourteen of the patients had positive serology; 10 had antinuclear antibodies and eight were anti-SSA and SSB positive. All the patients were cohabiting or married, except one who was divorced. No patient had any signs of diabetes mellitus or thyroid dysfunction or any other endocrine disorders.
The inflammatory activity was estimated by measuring the erythrocyte sedimentation rate according to Westergren (normal value 2–15 mm/1st h) and C reactive protein (normal value ⩽10 mg/l).
Controls
Fifteen healthy women who were not receiving any drugs served as controls for a comparison of the DHEA-S levels. Their mean age was 57 years (range 40–73), and nine were postmenopausal.
The study was conducted in accordance with the Declaration of Helsinki and was approved by the ethics committee at the Medical Faculty at Uppsala University.
Hormone measurements
Androstenedione was measured by radioimmunoassay (Androstenedione Radioimmunoassay Kit; Ortho-Clinical Diagnostics, Texas, USA). Total testosterone and DHEA-S were measured by solid phase radioimmunoassay (Diagnostic Products Corporation, Los Angeles, USA). Sex hormone binding globulin (SHBG) was measured by a time resolved sandwich fluoroimmunoassay (Wallac OY, Turku, Finland).
Questionnaires
The women were asked to complete two questionnaires, the McCoy Sexual Rating Scale23 and the Psychological General Well-Being Index (PGWB).24 The questionnaires were sent to the patients at home and returned by mail.
McCoy Sexual Rating Scale
Sexual life was assessed using a Swedish version of the McCoy scale which covers sexual experience and responsiveness during the past 30 days.23 This instrument contains 10 items on a seven point scale relating to different aspects of sexual life, such as frequency of intercourse, orgasm frequency, sexual pleasure and satisfaction, lubrication, dyspareunia, arousal, sexual fantasies, and satisfaction with partner.
Psychological General Well-Being Index (PGWB)
The schedule is a self assessed inventory related to general wellbeing24 and has been shown to be reliable and valid. It has been used in various clinical settings such as postmenopausal distress25 and in adults with growth hormone deficiency.26 The PGWB comprises 22 items with a six point response scale. The factors of anxiety, depressed mood, positive wellbeing, self control, general health, and vitality are related to the total score. The subscales of these measured factors have three to five items. For each item, there are six response options that are rated on a scale of 1 to 6, according to the intensity or frequency of the affective experience. A value of 1 is given for the most negative options and 6 for the most positive options. The score range for the PGWB is 22–132; a higher score represents better wellbeing.
Specific questions
We used isolated questions to assess tiredness and pain in the patients. To assess tiredness, we asked how the patients had felt for the past week on a scale of 1 to 6 with extreme points as “none of the time” and “the whole time”. Pain was assessed on a scale of 1 to 6 with extreme points of “no pain” and “very bad pain”.
Statistical analysis
Values are given as the mean (SEM) (range). Non-parametric tests (Mann-Whitney U and Spearman’s rank correlation test) were used to analyse data; a p value <0.05 was considered significant.
RESULTS
Table 1 presents the measured serum levels of DHEA-S, testosterone, androstenedione, SHBG, and the testosterone/SHBG ratio in the women with pSS. The mean DHEA-S level was significantly lower in the patients with pSS than in controls (2.3 v 3.5 μmol/l, respectively; p<0.05). The mean (SEM) erythrocyte sedimentation rate value was 18 (3) mm/1st h (range 5–42) and the mean serum C reactive protein value ⩽10 (0.4) mg/l (range 10–16).
Androgen hormone levels and sex hormone binding globulin in 21 patients with primary Sjögren’s syndrome. The data are presented as the mean (range)
The total mean (SD) score for the PGWB scale was 88.9 (13) in the patients with pSS. The total PGWB score correlated with the serum DHEA-S level (fig 1) but not with the serum levels of testosterone and androstenedione or the testosterone/SHBG ratio. Table 2 shows the PGWB subscale data in relation to hormone levels. The variables of depression, mental wellbeing, general health, and self control were all related to the DHEA-S values. General health and self control were also correlated to the serum levels of testosterone and androstenedione (table 2). No correlation was seen between the PGWB score and T/SHBG ratio.
Correlation coefficients between the mean scores on the Psychological General Well-Being Scale Index and androgen hormone levels in 21 patients with primary Sjögren’s syndrome
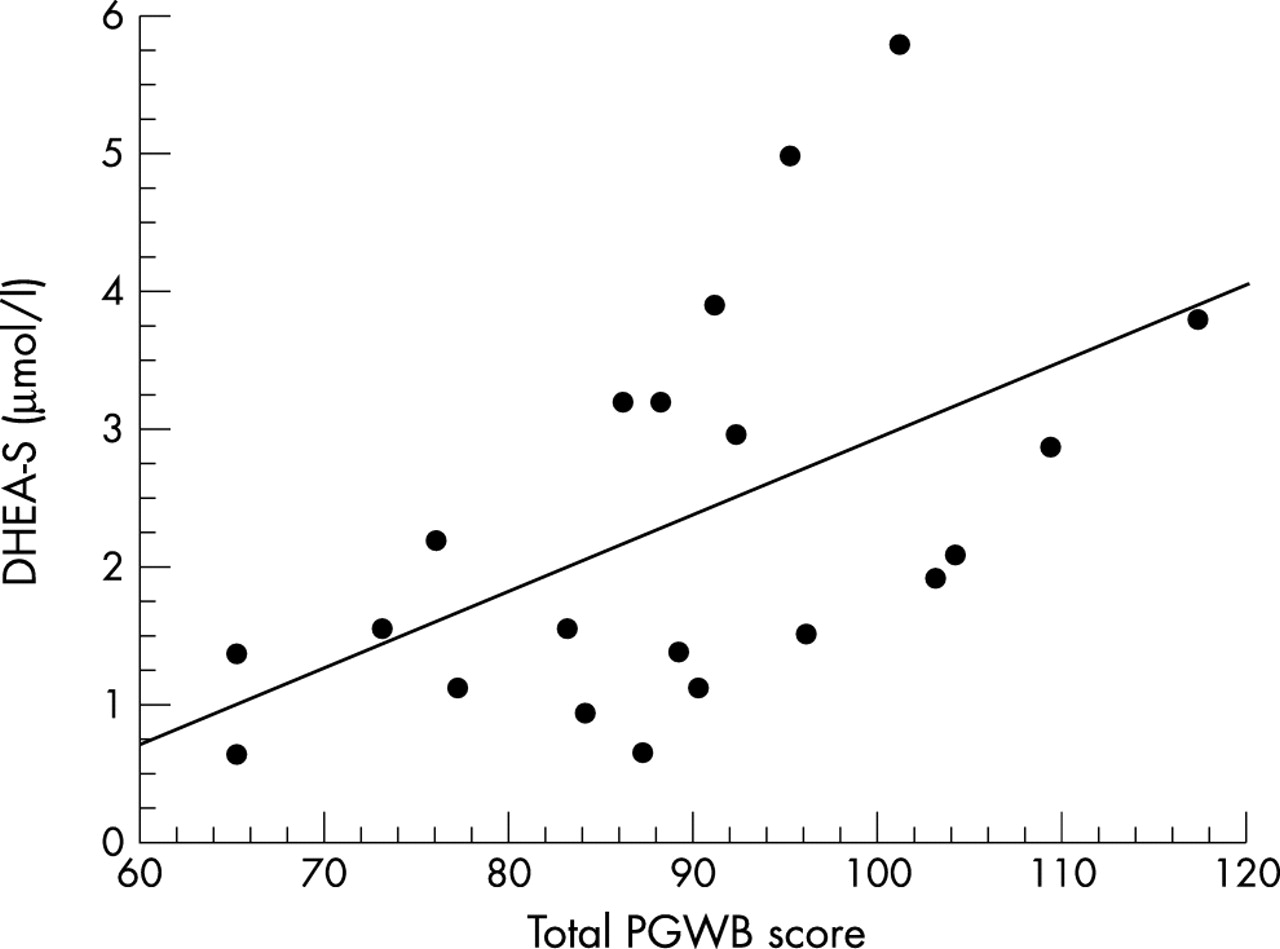
Correlation between DHEA-S levels and total PGWB score in 21 patients with primary Sjögren’s syndrome (rs=0.60, p<0.01).
Four of our patients had no active sex life and were therefore excluded from the calculations relating to the possible relationship between the McCoy rating scale and hormone serum levels. Significant positive correlations were seen between serum DHEA-S and total McCoy score (fig 2), the item assessing arousal, and the subscores for desire and satisfaction (table 3). No such correlation was seen between the total McCoy score or its subscores and the testosterone and androstenedione levels or the T/SHBG ratio, except between testosterone and dyspareunia (table 3). Ten (59%) and nine (53%) patients complained of vaginitis sicca and dyspareunia, respectively.
Correlation coefficients between psychosexual and androgen hormone variables in 17 women with primary Sjögren’s syndrome

{kind=link}
{kind=link}
Correlation between DHEA-S levels and total McCoy score in 17 patients with primary Sjögren’s syndrome (rs=0.62, p<0.01).
No differences in hormone levels were found in postmenopausal or premenopausal patients or between those receiving hormone replacement treatments or not. No association was found between vaginitis sicca and the hormone variables. There was no correlation between age and the DHEA-S levels or the total McCoy score. The hormone serum levels and the sexual or psychological wellbeing variables were not related to tiredness, pain, or laboratory inflammatory activity.
DISCUSSION
In this study the influence of endogenous androgens on psychological wellbeing and sexuality in women with pSS was investigated. Our findings show that there is a correlation between low serum DHEA-S concentrations and poorer mental wellbeing and decreased sexual quality of life in these patients.
Dehydroepiandrosterone and its sulphated metabolite DHEA-S are important intermediary products in the sex hormone pathway and can be converted to the potent androgens of testosterone, dihydrotestosterone, and androstenedione.27 Furthermore, DHEA and DHEA-S are present in the brain in rodents and primates, including humans.28 DHEA and DHEA-S have been classified as neurosteroids, referring to the fact that their accumulation in the brain is at least partly dependent on their synthesis de novo in the CNS.28–30 Much has been published about the potential effects of DHEA and DHEA-S on various systems and their changes in endogenous concentrations associated with different diseases.31 We have previously studied major androgens participating in the hypothalamic-pituitary-adrenal axis after the intravenous administration of corticotrophin releasing hormone. The results of that study showed that women with pSS have decreased serum concentrations of DHEA-S both at baseline and after stimulation compared with healthy controls.20 The reason for this abnormality in androgen metabolism in patients with pSS is unknown, but it may reflect a selective defect in the production of DHEA-S in the adrenal glands as the cortisol synthesis was intact. The observed dissociation between adrenal androgen synthesis and cortisol production may be constitutional but may also be secondary to the inflammatory disease process. It has been shown that immune adrenal interactions may play a part in the dysregulation of adrenal androgen production in pSS, as proposed for other autoimmune diseases like systemic lupus erythematosus.32,33
We have previously reported that women with pSS often have psychiatric symptoms and poorer wellbeing, which may affect their quality of life.9,10 We have also observed that oestrogen treatment has a negative effect on their wellbeing in contrast with the expected positive effect in healthy women receiving hormone replacement therapy.34 This observation made us suspect that a change in the oestrogen/androgen balance may contribute to the poorer quality of life in women with pSS.
Studies of depression in relation to serum DHEA-S concentrations have produced conflicting results.31 Barrett-Connor et al found that decreased levels of DHEA-S were significantly associated with depressed mood in a cohort of community dwelling postmenopausal women,35 whereas Cawood and Bancroft found no such connection.36 In an open labelled study, DHEA administration had beneficial effects on symptoms of depression.37 The studies of sense of wellbeing and DHEA-S have also produced a diffuse picture,31,38,39 but a large French epidemiological study demonstrated a correlation between circulating concentrations of DHEA-S and the feeling of wellbeing.27 By restoring DHEA-S to young adult levels in both men and women of advancing age, an improvement in physical and psychological wellbeing was obtained in both sexes.38 In our study, we found an association between low DHEA-S levels and lower total score on the PGWB in women with pSS. Furthermore, there were strong correlations between serum DHEA-S and the subscales for depression, sense of wellbeing, general health, and self control. The link observed previously between serum DHEA-S and neuropsychiatric symptoms and the present observations in women with pSS may reflect the neuroactive role which DHEA-S has for some important functions in the CNS, including the modulation of neurotransmission, brain excitability, and behaviour.30,40 Experimental studies have also shown that DHEA-S provides neuroprotection. However, the role of DHEA-S in the human CNS function still remains unclear.
Knowledge of the influence of endogenous androgens on sexual life in women is limited.23,41 Although there is consensus that sexual interest and activity decline in women as they get older, consistent evidence that this is due to hormonal changes is lacking.36 For a variety of reasons, it can be assumed that rheumatic diseases affect sexual function. Firstly, patients have physical limitations due to pain and immobility and, secondly, drugs can cause fatigue, impotence, and lack of desire. Moreover, patients may have problems with self esteem and body image. Women with Sjögren’s syndrome have diminished vaginal lubrication, which may cause painful intercourse.42 About 60% of our patients had difficulty with intercourse because of vaginal dryness and dyspareunia, but we found no association between the total McCoy score and decreased vaginal lubrication, suggesting that psychosocial factors may have a more important role in sexual function than physical limitations attributable to pSS. A longitudinal study of the effects of menopause on sexuality showed that testosterone was associated with the frequency of sexual behaviour.23 In our study we found a correlation between DHEA-S and decreased psychosexual function and not with testosterone or androstenedione. This may support the notion that DHEA-S is important for the androgen status and sexual function of women with pSS.
The wide spectrum of symptoms in pSS includes neuropsychiatric manifestations.4,9 Our observations that women with pSS have lower serum DHEA-S levels than age matched women and that low serum DHEA-S is linked to poorer wellbeing raises the question of whether androgen status has a pathophysiological role in the development and symptomatology of pSS. Glucocorticoid treatment depresses the adrenal synthesis of androgens.43 So, the previously reported low levels of DHEA-S in systemic lupus erythematosus and rheumatoid arthritis may be due, at least in part, to current or previous glucocorticoid treatment.12–14 A drug mediated influence of this kind can definitely be excluded in our patients with pSS who had never received glucocorticoids. It is not possible to say from this study whether or not an impaired DHEA synthesis in pSS precedes the disease or is a secondary manifestation of the disease process. However, the possibility remains that the androgen status is of importance for manifestations other than poorer wellbeing in patients with pSS, because androgen administration to female mice with Sjögren’s syndrome has a successful effect on the inflammatory disease attack on exocrine glands.17–19
The current means of ameliorating various symptoms in patients with pSS using pharmacological principles are limited. We suggest that the restoration of DHEA-S to normal circulating levels in women with pSS should be considered as a possible future strategy to improve their mental wellbeing and the quality of their sexual life.
Acknowledgments
We thank Inger Ohlsson and Lotta Karnell, research nurses, for their excellent technical assistance. We also thank Margareta Lindström for the hormone analysis and Dr Tord Naessen, Department of Women’s and Children’s Health, Section of Obstetrics and Gynecology, University Hospital, Uppsala, for their help in collecting blood samples from the controls.
This study was supported by the Gustaf Prim’s Foundation and the Faculty of Medicine, Uppsala University.