Article Text

Abstract
Background: Systemic lupus erythematosus has a wide spectrum of immunological and clinical manifestations. Its course is characterised by exacerbations which may result in mortality or morbidity to vital organs/systems.
Objective: To determine clear and early prognostic markers to avoid further complications.
Methods: 245 adult patients diagnosed between January 1978 and March 2001 were studied. Clinical manifestations and laboratory findings both at onset and during the clinical course were collected. The number, type, and severity of the flares were also noted. Statistical analyses between disease features at onset, subsequent flares, and mortality were performed.
Results: 239 patients entered the study. Their mean age at onset was 30 years. The mean time between onset and diagnosis was 36 months and the mean evolution time was 114 months. 205 patients developed 915 flares; 205 (22.4%) of these flares were major flares, and affected 110 patients. Cardiac, neurological, or renal affection at onset were associated with a higher probability of developing cardiac (p=0.022), neurological (p<0.001), and renal (p<0.001) exacerbations, respectively, during the evolution. Lupus anticoagulant (LA) and anticardiolipin antibodies (aCL) were predictors of stroke (aCL, p=0.000; LA, p=0.001). Age at diagnosis (p=0.003) and valvular disease at onset (p=0.008) were independent predictors of low survival.
Conclusions: Renal, cardiac, or neurological involvement and the presence of LA or aCL positivity at onset were predictors of renal, cardiac, or neurological flares, respectively. Age and valvular involvement at onset were found to be independent adverse outcome predictors for low survival.
- systemic lupus erythematosus
- onset
- prognosis
- mortality
- aCL, anticardiolipin antibodies
- ANA, antinuclear antibodies
- anti-dsDNA, anti-double stranded antibodies
- CI, confidence interval
- ELISA, enzyme linked immunosorbent assay
- LA, lupus anticoagulant
- OR, odds ratio
- SLE, systemic lupus erythematosus
- SLEDAI
- SLE Disease Activity Index
Statistics from Altmetric.com
- aCL, anticardiolipin antibodies
- ANA, antinuclear antibodies
- anti-dsDNA, anti-double stranded antibodies
- CI, confidence interval
- ELISA, enzyme linked immunosorbent assay
- LA, lupus anticoagulant
- OR, odds ratio
- SLE, systemic lupus erythematosus
- SLEDAI
- SLE Disease Activity Index
The survival of patients with systemic lupus erythematosus (SLE) has improved remarkably over the past decades. Earlier diagnosis of SLE, awareness of vascular risk factors (for example, hypertension, nephrotic syndrome, antiphospholipid syndrome), recognition of mild disease, and better approaches to treatment have undoubtedly contributed to the improved prognosis of patients with SLE. However, 3–18% of patients still die within the five years of disease onset.1–3 Death is mainly related to nephritis and central nervous system disease4,5 as well as to damage to other vital organs, intercurrent infection, complications related to treatment, and atherosclerosis in the long term.6–8
Studies of variables which affect mortality in SLE have identified a wide range of prognostically significant factors, including demographic,9 clinical,10 laboratory,11 and histological features.12 However, the contribution of the initial clinical and laboratory features to the course and outcome of SLE has not yet been examined.
This study was conducted to determine the relationship between clinical and laboratory features and the development of major flares and the mortality during the course of the disease in a cohort of Spanish patients with SLE followed up prospectively at a single centre.
PATIENTS AND METHODS
The study was performed in an acute care, 900 bed, university hospital in the city of Barcelona, Spain. Two hundred and forty five patients diagnosed with SLE in our centre or diagnosed in other centres but referred to us between January 1978 and March 2001 were evaluated retrospectively. All of them met the revised criteria of the American College of Rheumatology for classification of SLE13 and were cared for at the hospital by the same medical team of the Internal Medicine Rheumatology service. Drug induced SLE and childhood SLE (when diagnosis was made before 14 years of age) were excluded. Information on medical history, physical examination, clinical symptoms, laboratory findings, treatment, and outcome present at the first patient’s referral to the hospital and subsequently at any time during the follow up was prospectively registered in a database. Disease activity of SLE was evaluated with the SLE Disease Activity Index (SLEDAI).14 The SLEDAI of the flares before 1992 was calculated retrospectively based on clinical data. Patients were reviewed at six month intervals or more frequently when needed. At each assessment a complete medical history, a physical examination, and a laboratory evaluation were performed. Other diagnostic studies for the assessment of any clinical event, episode of flare, or organ system involvement were performed according to the criteria of the medical team.
One hundred and two variables were selected for the purpose of this study (see appendix) and reviewed. Overall, we took into account the demographic information (age, sex, race), the clinical data, the laboratory and immunological features, and the outcome. Age at the initial manifestations, at the diagnosis of SLE, and at enrolment into the cohort were recorded and categorised (<30 years, 30–60 years, and >60 years), as well as the duration of the disease from the initial manifestations to the diagnosis and from the diagnosis to the enrolment. Clinical data, laboratory findings, and immunological features were considered both at the onset of SLE and during the course of the disease.
The onset time was considered as the time when the first symptom or laboratory data attributable to lupus disease was detected. A flare was defined as any clinical event directly attributable to disease activity that required a change in treatment. Those flares which represented a life threatening relapse or a relapse that would result in irreversible organ system damage in the absence of treatment were defined as major flares. The clinical flares that occurred during the first five year follow up period, organ involvement, SLEDAI score of each flare, and overall SLEDAI score of major flares were assessed.
The clinical manifestations were defined according to the American Rheumatism Association glossary committee.15 A renal biopsy was performed on the patients with the first renal flare; specimens were evaluated using the 1982 World Health Organisation criteria for the classification of lupus nephritis.16
Laboratory investigations included full blood cell count, coagulation tests, routine biochemical and lipid profile, urine cytometry, and 24 hour proteinuria. A diagnosis of leucopenia was defined for a white blood cell count <4×109/l, anaemia for haemoglobin levels <140 g/l in men and <120 g/l in women, and thrombocytopenia for a platelet count <100×109/l. Autoimmune thrombocytopenia was considered when antiplatelet antibodies were present and other causes for reduction in the platelet count were excluded.17
Immunological data included antinuclear antibodies (ANA; by an indirect immunofluorescence method); antibodies to double stranded DNA (dsDNA; by an enzyme linked immunosorbent assay (ELISA)-Crithidia luciliae technique); anti-Ro (SSA), anti-La (SSB), anti-Sm, and anti-RNP (by counterimmunoelectrophoresis); high affinity IgG/IgM anticardiolipin antibodies (by a modified ELISA using a previously reported technique18); serum levels of complement factors (C3, C4, and CH50); and lupus anticoagulant (LA; by the coagulometric assays proposed by International Committee for the Standardisation of Lupus Anticoagulants19). Stored serum from the former flare was used to perform both the anticardiolipin antibodies (aCL) and the LA tests if the patient had been diagnosed with lupus before the description of these antibodies.
Statistical analysis
The information was stored in the Microsoft Access database programme and statistical analysis was performed by means of the SPSS/PC 10.0 programme. Conventional χ2 test, Fisher’s exact test, and independent samples Student’s t test were used to compare categorical variables and means at the univariate analysis. Odds ratio (OR) with 95% confidence intervals (CI) was calculated using the univariate Cox’s test. When variables appeared potentially predictive in the univariate analysis, they were evaluated using a stepwise forward strategy with the multivariate Cox’s method. The Kaplan-Meier method was used for survival analysis, and the significance of the differences between groups was assessed using the log rank test. The survival time was considered as the time from diagnosis until death or the moment of the study. All the reported p values are two sided.
RESULTS
The study group comprised 239 patients (male:female ratio 1:5). Six female patients who met the study criteria could not be followed up and were excluded. The mean age of the study group at diagnosis of SLE was 33 years and the mean interval between the initial manifestations and diagnosis of the disease was 36 months. The mean duration of the follow up was 114 months.
The most common initial features of SLE were arthritis or arthralgia (84%), cutaneous disease (75%), general symptoms (asthenia, fever, Raynaud’s phenomenon) (56%), and leucopenia/lymphopenia (47%). Less common manifestations were gastrointestinal and neurological disease. As the patients could present symptoms simultaneously, the total number of clinical manifestations is greater than the total number of patients. ANA were positive in all patients (100%), whereas anti-dsDNA was positive in 47%. Table 1 shows the clinical and laboratory data.
Initial features of SLE in a cohort of 239 patients
During the interval between diagnosis and enrolment into the cohort 201 patients had a total of 915 flares with a mean of 4.6 flares per patient. Thirty eight patients, however, had no flare. Among the total number of flares, 205 (22.4%) were major flares and affected 110 patients (table 2). Fifteen patients presented flares that affected more than one organ/system. Renal flares (particularly in the form of class IV and V lupus nephritis) were the most common (107 cases), followed by neurological (50 cases) and haematological (34 cases) flares. The χ2 test showed a significant association between the manifestations of SLE and major flares for the haematological system (15/19 (79%) patients with haematological flares had haematological disease at the onset, p=0.011); the heart (6/9 (67%) patients, p=0.022); the kidney (35/70 (50%) patients, p<0.001); and the nervous system (18/36 (50%) patients, p<0.001). Migraine and stroke, as well as nephritis (class IV and V) as initial manifestations of SLE were strongly related to the development of stroke and to the same class of nephritis during the course of the disease. Stroke actually occurred in 4/22 patients with migraine and in 4/13 with initial stroke. Similarly, nephritis class IV was seen in 13/17 patients with initial class IV nephritis, and 4/7 patients with class V nephritis had had an initial class V nephritis (p<0.01 for all comparisons). Positive aCL and LA at onset were significantly associated with Libman-Sacks endocarditis, neurological flares, and stroke. Table 3 shows the ORs and 95% CIs for the type of flare at follow up according to the initial features. In the logistic regression model, none of the variables studied was selected as an independent predictor of the type of flare to appear during the follow up.
Distribution of 205 major flares in a cohort of 239 patients with SLE
Contributions of the initial features to the development of major flares during the course of SLE. Results of univariate analysis
A total of 24 patients had died, with a mean follow up after SLE diagnosis of 108 months. The mortality rate was 10%. Seven patients died within the first five years after diagnosis (which is considered the period with highest disease activity), nine died between six and 10 years, and eight after 10 years. The causes of death were intercurrent infection (13 patients), active SLE (6 patients), valvular heart disease or valve replacement surgery (4 patients), and ischaemic heart disease (1 patient).
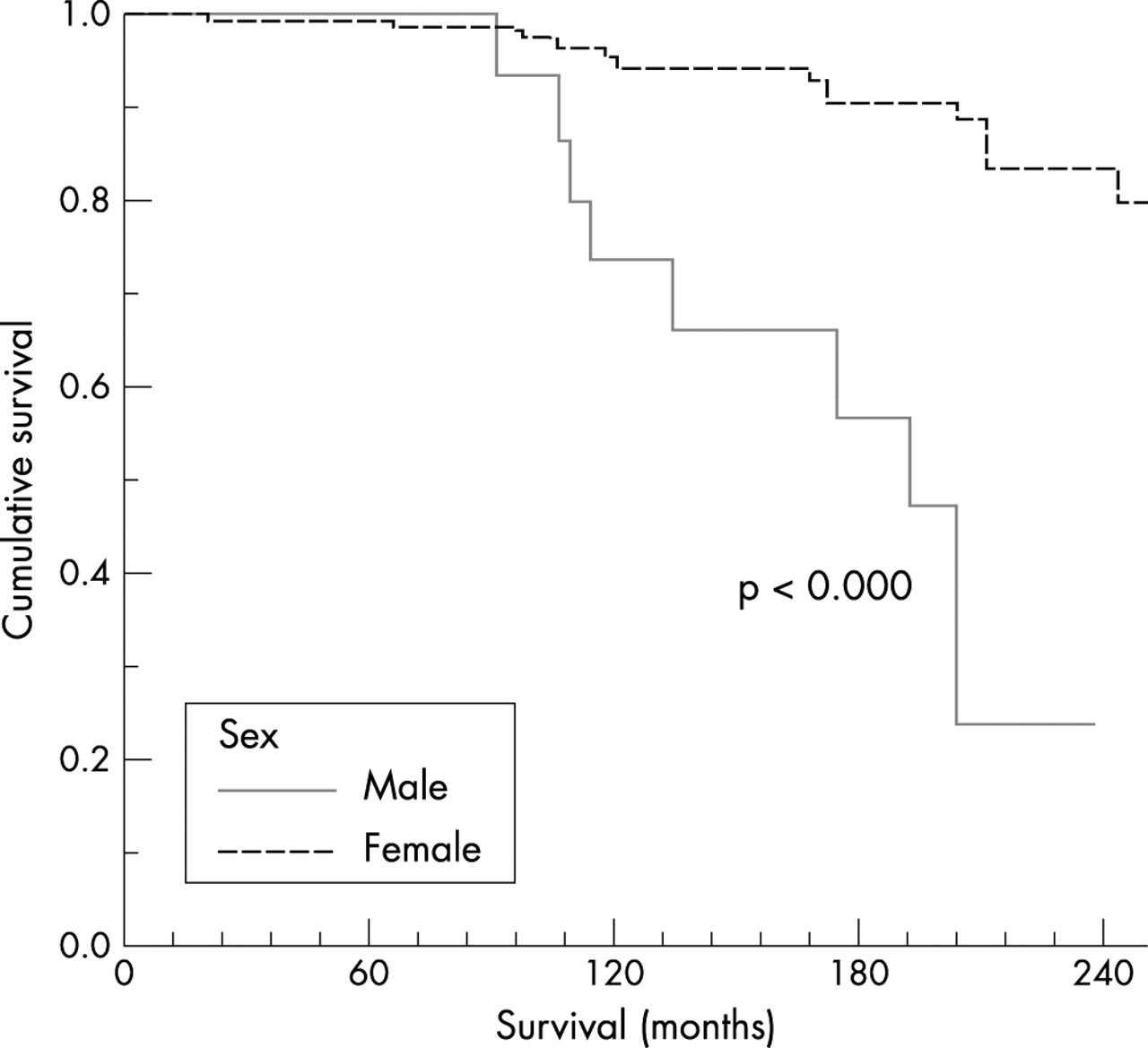
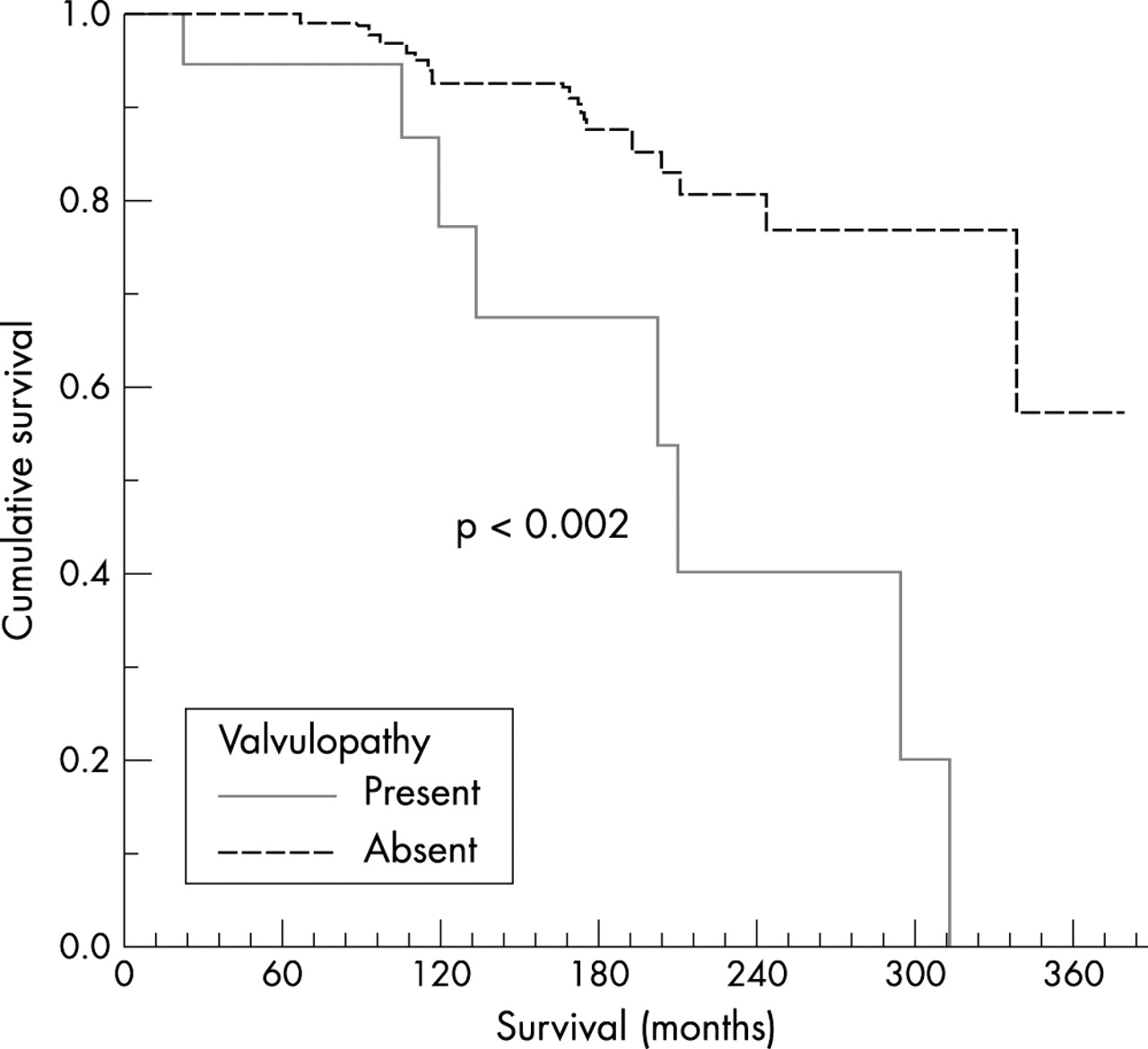
As for the initial features of SLE, 10/54 patients with renal disease, 11/71 with cardiac manifestations, and 8/46 with autoimmune thrombocytopenia died. In the subsets of patients with initial renal or haematological manifestations, fatal outcome was not related to any particular disease. Patients with initial cardiac manifestations, valvular heart disease, and rhythm disturbances showed a worse prognosis: 4/6 patients with dysrhythmia and 7/19 with valvular heart disease died. Univariate analysis showed that six of the initial clinical and laboratory features at onset were significantly associated with poor survival in this cohort: male sex (p<0.000), age at diagnosis over 60 (p<0031), renal disease (p=0.041), heart disease (p<0.01), valvulopathy (p<0.002), and positivity for LA (p=0.0077). After a multivariate statistical study two of these variables were independent predictors of lower survival: age at diagnosis (p=0.003) and the presence of valvular disease at onset (p=0.008). Figures 1–6 show the Kaplan-Meier curves of these items. Table 4 shows the survival prognosis at 1, 5, 10, 15, and 20 years for these variables.
Survival probabilities according to the significant parameters in the univariate analysis

Cumulative survival according to age at diagnosis.

Cumulative survival according to sex.

Cumulative survival according to the presence of cardiopathy at onset.

Cumulative survival according to the presence of valvulopathy at onset.

Cumulative survival according to the presence of nephropathy at onset.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative survival according to the presence of LA at onset.
DISCUSSION
The main aim of the study was to find a rational relationship between the pattern of onset and the evolution of lupus disease. Few reports have considered the relationship between the initial manifestations of lupus disease and its prognosis. The ability to predict future activity of the disease would be of great value for specific patients groups.
The initial clinical and laboratory features of this cohort showed no differences from two descriptive analyses of subjects with apparently similar disease from similar geographical areas and with similar socioeconomic status (Greece20 and Spain21). Some other studies with larger numbers of patients have been conducted—for example, the European Working Party on Systemic Lupus Erythematosus.22,23 The origin of those patients was from Mediterranean and non-Mediterranean countries. For this reason those patients were excluded as references for comparisons.
We found a clinical relationship between the initial features and subsequent episodes of major flares when the heart, kidney, and nervous system were the organs affected at the onset of SLE; this was also true for patients with haematological disorders at onset. More patients with either initial haematological manifestations or cardiac symptoms developed haematological or cardiac flares than those without such initial symptoms, and as in the case of renal or neurological manifestations as initial features, the type of major flare reflected the initial symptoms. Patients with class IV or class V nephritis repeated the same class of nephritis during the evolution of SLE, and patients with stroke or migraine at onset had a higher probability of having a subsequent brain ischaemic infarction. Patients with psychosis or brain syndrome had an increased risk of lupus encephalopathy. Therefore, it is reasonable to think that some organs may be predisposed to recurrent injuries from lupus disease. This may enhance the value of other predictive factors of disease activity, such as changes in cell blood count, erythrocyte sedimentation rate, complement levels, or anti-dsDNA antibody titres, and may contribute to defining a clinical and a immunological profile for patients in whom a close follow up would be desirable.
aCL and LA at the onset of SLE were significantly associated with lupus endocarditis and neurological flares. The procoagulant effect of antiphospholipid antibodies has been previously associated with cardiac and neurological disease especially with aseptic endocarditis, valvular heart disease, and stroke.24 Five of the nine pulmonary flares that developed during the course of the disease were classified as pulmonary hypertension or pulmonary thromboembolism. Antiphospholipid syndrome has been occasionally related to pulmonary thromboembolism and pulmonary hypertension,25 but the small number of patients with pulmonary flares in our study makes it difficult to find a clear relationship. Similarly, the relationships found between neurological disease subsets at onset and stroke, encephalopathy, or epilepsy as the SLE evolves are statistically significant but clinically weak owing to the low number of patients or flares involved.
A number of features related to the SLE process itself have been found to be predictive for mortality in different studies,9,26–30 and our results partially agree with them. However, extrapolation of data across countries is hampered by the effect of non-SLE factors, such as ethnicity, socioeconomic status, or healthcare coverage. In our cohort all the patients were white and Spanish citizens, and came from the same hospital. A second bias results from an actuarial evaluation of the clinical manifestations of SLE. In this study we evaluated the manifestations at the onset of the disease and not at any point during the evolution.
In this cohort of patients the risk of death increased with the age at diagnosis and was a predictor of low survival in both the univariate and the multivariate statistical analyses. This fact did not seem to be related to the time of evolution of SLE: the numbers of patients who died within the first five years, between six and 10 years, and after 10 years of being diagnosed were similar. This suggests that patients diagnosed at advanced ages have a higher risk of death which is not related to the lupus activity.
Male patients had a worse survival prognosis than women in our cohort. One third of those who died were men, while the ratio female/male in the whole group was 5:1. However, male patients did not have higher SLEDAI values for any flare, higher number of flares, or different causes of death than women.
Previous studies have clearly indicated the prognostic value of renal disease, especially of class IV nephritis, and of high levels of proteinuria or haematuria.31,32 These studies, however, analysed the cumulative prevalence of nephritis without considering the timing of disease and data were collected before the use of cyclophosphamide. In our cohort, 54/239 patients presented with renal disease as the initial manifestation of SLE, and 70 patients experienced 107 major renal flares at follow up. Although only two patients needed haemodialysis and no patient died because of specific renal damage, the overall mortality in lupus patients with nephropathy was higher than in those without nephropathy. However, most of the patients who died and had a history of lupus nephropathy had been diagnosed before the introduction of intravenous cyclophosphamide pulses. Better control of the morbidity due to kidney disease (in particular, infection and vascular risks factors), together with improvements in the immunosuppressive treatment (especially the combination of pulses of cyclophosphamide and corticosteroids) in the past 10 years, have improved the prognosis of the disease.
Cardiovascular manifestations in lupus disease have an important role in the morbidity/mortality of patients with SLE. Heart affection in SLE has an immunological basis, but other concomitant underlying conditions may also be present.33 Valvular heart disease is clearly associated with aCL,34 and it has been shown to be a basis for coronary disease35 independently from antiphospholipid syndrome. Besides, cardiovascular disease in SLE may occur despite immunosuppressive treatment. It is likely that abnormalities of heart rhythm are secondary to valvulopathy and not necessarily a consequence of damage to the conduction system. Many patients with severe valvular dysfunction will need valve replacements to improve their functional status. The higher morbidity and mortality due to cardiac surgery in patients with SLE in comparison with the general population36 may account for the impact of cardiac manifestations at onset on survival. In our cohort, 67% of patients with rhythm disturbances and 37% of patients with valvular disease died. The univariate statistical analysis showed that the value of cardiac manifestations at onset and especially the presence of valvulopathy were markers of lower survival. When the multivariate analysis was performed, valvular disease was shown to be an independent predictor of low survival.
Interestingly, no immunological variables, except LA, at onset of SLE were associated with survival. Previous studies have evaluated laboratory and immunological tests (such as serum complement levels, anti-dsDNA, antinuclear, and anti-extractable nuclear antigen antibodies, as well as antiphospholipid antibodies), but no relationship with the outcome has been found.5 The LA affects not only vascular events throughout the body but also valvular disease. In this study 9/42 patients positive for LA died, and the cause of death in all cases was a vascular event affecting the central nervous system.
Thrombocytopenia has been recognised as a predictor for mortality.19,30 In our cohort, 19% of patients had thrombocytopenia at onset. Just 8% of patients without thrombocytopenia died, but this was not statistically significant.
In summary, renal, cardiac, or neurological disease as well as positive LA and aCL at the onset of disease were significant risk factors for major flares related to these specific organs. Survival in this cohort is associated with the age at diagnosis, sex, the presence of cardiac, valvular, or renal disease at the onset of SLE, and with positivity for LA. The age at diagnosis and the presence of valvulopathy at onset were independent low survival predictors.
APPENDIX 1: LIST OF VARIABLES SELECTED FOR THIS STUDY
Age, sex, onset date, diagnosis date, age at diagnosis, onset time, evolution time; onset manifestations: general symptoms, asthenia, anorexia, fever, weight loss, thrills, lymphadenopathies, Raynaud’s phenomenon, dyspnoea, skin lesions, photosensitivity, discoid lupus, subacute lupus, acute lupus, alopecia, oral aphthosis, vasculitic lesions, other unspecific skin lesions, musculoskeletal affection, arthritis, arthralgias, myalgias, myositis, bone destruction, avascular necrosis, tendinous break, muscle break, fracture, soft tissue calcifications, non-deforming arthritis, deforming arthritis, spinal crush, osteomyelitis, pulmonary affection, pleuritis, pleural effusion, pneumonitis, pulmonary thromboembolism, pulmonary hypertension, pulmonary fibrosis, pulmonary haemorrhage, diaphragmatic palsy, pulmonary distress, cardiac affection, pericarditis, myocarditis, myocardiopathy, valvulopathy, ischaemic myocardiopathy, rhythm disturbance, thrombosis, renal manifestation, minimum change nephritis, mesangial nephritis, focal proliferative nephritis, diffuse proliferative nephritis, membranous nephritis, interstitial nephropathy, thrombotic microangiopathy, vasculitis, renal sclerosis, nephrotic syndrome, arterial hypertension, acute renal insufficiency, chronic renal insufficiency, haematuria, leucocyturia, hyaline casts, granulomatous casts, proteinuria, digestive manifestations, primary biliary cirrhosis, sclerosis cholangitis, nodular hepatic hyperplasia, lupoid hepatitis, pancreatitis, neurological affection, multineuritis, multiple mononeuritis, polyneuritis, migraine, stroke, myelitis, chorea, aseptic meningitis, convulsions, Guillain-Barré syndrome, dementia, meningoencephalitis, depression, psychosis, cognitive impairment, gynaecological manifestations, abortion, fetal loss, early menopause, ophthalmological affection, autoimmune haemolytic anaemia, autoimmune thrombocytopenia, leucopenia, laboratory manifestations, ANA, anti-dsDNA antibodies, AMA, anti-Ro/SSA, anti-La/SSB, anti-RNP, anti-TGB, anti-peroxidase, lengthened activated partial thromboplastin time, rise in ESRD, rheumatoid factor, LA, AClies, false positivity for Venereal Disease Research Laboratory test, hypocomplementaemia, steroid treatment, cytostatic treatment; flares: number of flares, number of major flares, number of mixed flares, number of flares in the first five years, actuarial SLEDAI, mean SLEDAI, number of diagnosis criteria, pulmonary flare, pulmonary thromboembolism, lupus pneumonitis, pulmonary hypertension, pulmonary haemorrhage, cardiac flare, Libman-Sacks endocarditis, myocarditis, coronary vasculitis, arrhythmia, cardiac tamponade, digestive flare, pancreatitis, mesenteric vasculitis, neuropsychiatric flare, meningoencephalitis, encephalopathy, epilepsy, polyneuropathy, stroke, myelitis, chorea-ataxia, Guillain-Barré syndrome, myopathy, haematological flare, aplastic anaemia, autoimmune haemolytic anaemia, autoimmune thrombocytopenia, thrombotic thrombocytopenic purpura, renal flare, type II nephritis, type III nephritis, type IV nephritis, type V nephritis, nephrotic syndrome, death, cause of death.
Acknowledgments
We thank Lluïs Armadans, MD, for his contribution to the statistical analysis.
REFERENCES
Footnotes
-
Supported by FIS grant number 00/0882.