Article Text

Abstract
Background: Recent studies with infliximab indicate the therapeutic potential of tumour necrosis factor α blockade in spondyloarthropathy (SpA). Because defective host defence is implicated in the pathogenesis of SpA, the potential side effects of this treatment due to impact on the antimicrobial defence are a major concern.
Objective: To report systematically the adverse events seen in a large cohort of patients with SpA treated with infliximab, with special attention to bacterial infections.
Patients and methods: 107 patients with SpA were treated with infliximab for a total of 191.5 patient years. All serious and/or treatment related adverse events were reported.
Results: Eight severe infections occurred, including two reactivations of tuberculosis and three retropharyngeal abscesses, and six minor infections with clear bacterial focus. One patient developed a spinocellular carcinoma of the skin. No cases of demyelinating disease or lupus-like syndrome were seen. Two patients had an infusion reaction, which, however, did not relapse during the next infusion. Finally, three patients with ankylosing spondylitis developed palmoplantar pustulosis. All patients recovered completely with adequate treatment, and infliximab treatment had to be stopped in only five patients with severe infections.
Conclusions: Although the global safety of infliximab in SpA is good compared with previous reports in rheumatoid arthritis and Crohn’s disease, the occurrence of infections such as tuberculosis and retropharyngeal abscesses highlights the importance of careful screening and follow up. Focal nasopharyngeal infections and infection related symptoms, possibly induced by streptococci, occurred frequently, suggesting an impairment of specific host defence mechanisms in SpA.
- infection
- infliximab
- safety
- spondyloarthropathy
- tumour necrosis factor α
- ANA, antinuclear antibodies
- AS, ankylosing spondylitis
- CD, Crohn’s disease
- CRP, C reactive protein
- CT, computed tomography
- DMARD, disease modifying antirheumatic drug
- ESR, erythrocyte sedimentation rate
- HACAs, human antichimeric antibodies
- IV, intravenously
- NSAIDs, non-steroidal anti-inflammatory drugs
- PsA psoriatic arthritis
- RA, rheumatoid arthritis
- ReA, reactive arthritis
- SpA, spondyloarthropathy
- TNFα, tumour necrosis factor α, uSpA, undifferentiated spondyloarthropathy
Statistics from Altmetric.com
- ANA, antinuclear antibodies
- AS, ankylosing spondylitis
- CD, Crohn’s disease
- CRP, C reactive protein
- CT, computed tomography
- DMARD, disease modifying antirheumatic drug
- ESR, erythrocyte sedimentation rate
- HACAs, human antichimeric antibodies
- IV, intravenously
- NSAIDs, non-steroidal anti-inflammatory drugs
- PsA psoriatic arthritis
- RA, rheumatoid arthritis
- ReA, reactive arthritis
- SpA, spondyloarthropathy
- TNFα, tumour necrosis factor α, uSpA, undifferentiated spondyloarthropathy
Multiple studies have recorded the therapeutic potential of biological therapies which block anti-tumour necrosis factor α (TNFα) in rheumatoid arthritis (RA)1,2 and in Crohn’s disease (CD).3,4 The major impact of TNFα blockade on the immunological system raised concerns about the safety of this approach, especially with regard to severe infections, malignancies, and immune mediated diseases. As to major infections, TNFα blockade appears to be associated with a higher incidence of tuberculosis, mostly extrapulmonary disease occurring within a few weeks after the start of the treatment.5 Although there are some case reports of other major infectious complications such as histoplasmosis,6 safety data from the different clinical trials indicate that these events are not increased in treated patients compared with those receiving placebo. As to malignancies, there is at present no evidence for a causal relationship between TNFα blockade and the development of lymphoid or non-lymphoid cancers,7 although some cases have been reported and warrant further careful screening and follow up.
Finally, possible immune mediated side effects include allergic infusion reactions, neurological events suggestive of demyelisation,8 and the appearance of antinuclear autoantibodies (ANA), but mostly without clinical signs of lupus.9
Recently, several studies have documented the clinical efficacy of infliximab, a chimeric monoclonal antibody to TNFα, in spondyloarthropathy (SpA).10–14 Because defective host defence plays a part in the pathogenesis of reactive arthritis (ReA), and probably also other SpA subtypes, the occurrence of severe infectious complications is a major concern for TNFα blockade in SpA. We studied a unique, monocentric cohort of 107 patients with SpA treated with infliximab for 1–3 years, and report the systematic safety follow up in this new indication for TNFα blockade, focusing essentially on infections and infection related symptoms. Although short term safety has already been reported for 41 of these patients,10,12 the present long term safety follow up in this large cohort yielded a number of unexpected infectious complications, which were neither previously observed with long term TNFα blockade in RA and CD nor in the previously mentioned short term evaluations in SpA.
PATIENTS AND METHODS
A total of 107 patients with SpA were included in three different trials with infliximab.10,12 All patients fulfilled the European Spondylarthropathy Study Group (ESSG) criteria,15 had active disease defined as the presence of inflammatory back pain and/or the presence of at least one swollen joint or enthesis, and gave written informed consent for the studies as approved by the local ethics committee. All patients received a loading dose regimen of 5 mg/kg infliximab intravenously (IV) at baseline, week 2, and week 6. Table 1 summarises the characteristics and treatment schedules of the three cohorts.
Characteristics and treatment schedules of the 107 patients with SpA treated with infliximab. This group of 107 patients comprised three different cohorts with slightly different retreatment schedules
The first cohort, started between November 1999 and March 2000, comprised 31 patients: 16 ankylosing spondylitis (AS), 11 psoriatic arthritis (PsA), and 4 undifferentiated SpA (uSpA). After the loading regimen they were treated with 5 mg/kg infliximab IV every 14 weeks for one year, 5 mg/kg infliximab IV every 10 weeks during the second year, and finally 5 mg/kg infliximab IV every eight weeks during the third year. One of these patients had concomitant disease modifying antirheumatic drug (DMARD) treatment with methotrexate; two patients were treated with low dose (<10 mg/day prednisolone) oral corticosteroids. The total duration of follow up of this cohort is 83.1 patient years. Efficacy and safety at three months and one year in, respectively, 21 and 19 of these patients were reported previously.10,14
The second cohort, started between November 2000 and February 2001, comprised 40 patients: 19 AS, 18 PsA, and 3 uSpA. After the induction regimen they were treated with 10 mg/kg infliximab IV every 14 weeks for one year and with 5 mg/kg infliximab IV every eight weeks during the second year. None of these patients received DMARDs and two were treated concomitantly with low dose prednisolone. The total duration of follow up of this cohort is 63.6 patient years. Efficacy and safety at three months in, respectively, 20 infliximab treated and 20 placebo treated patients were reported previously.12
The third cohort comprised 36 patients: 26 AS, 3 PsA, and 7 uSpA. After receiving a loading regimen between March 2001 and October 2001, they were treated with a maintenance schedule of 5 mg/kg infliximab IV every eight weeks. Because this cohort was included in a compassionate use programme in which concomitant treatment was allowed, 18 patients continued to receive methotrexate (7.5–15 mg/week) during the first 4–34 weeks of anti-TNFα treatment. Four patients were receiving low dose prednisolone. The total duration of follow up of this cohort is 44.8 patient years.
During systematic follow up of the 107 patients over a total period of 191.5 patient years, all adverse events were registered. The adverse events that are reported here include all serious adverse events and all events that were possibly treatment related in the opinion of the investigator and that required specific therapeutic interventions and/or interruption of infliximab treatment. These events include severe infections (infections requiring admission to hospital and antibiotic treatment), minor infections with a clear bacterial focus (requiring antibiotic treatment but no admission to hospital), malignancies, allergic infusion reactions, demyelinating or lupus-like syndromes, and specific skin eruptions. Minor adverse events which are unlikely to be treatment related (headache, dizziness, . . .) and did not require specific treatment were not taken into consideration.
RESULTS
Global safety figures
A total number of 20 possibly treatment related and/or serious adverse events were recorded over a follow up period of 191.5 years (10.4/100 patient years), including 14 infectious adverse events (7.3/100 patient years) (table 2). The adverse events consisted of 10 serious adverse events (eight severe infections, one malignancy, probably non-treatment related, and one infusion reaction), and 10 minor adverse events that were considered possibly treatment related by the investigator (minor infections with clear bacterial focus, skin eruptions, mild infusion reaction). However, infliximab treatment had to be stopped in only five patients, all of them because of serious infections (2.6/100 patient years). Because treatment of two other patients was stopped because of lack of efficacy and because two patients withdrew their informed consent, this means that 98/107 (92%) patients continue to receive infliximab treatment after a mean of 1.79 years.
Overview of the 20 possibly treatment related and/or serious adverse events in the 107 patients with SpA treated with infliximab for a total number of 191.5 patient-years. Disease duration is given in years
Severe infections
Eight cases of severe infections were observed. Disseminated tuberculosis occurred in two patients: one PsA and one uSpA. Neither of them had a personal or familial history of tuberculosis. Both patients initially responded well to infliximab, but developed high fever, general malaise, and increasing inflammatory parameters nine weeks after the start of treatment. Classical diagnostic investigation for infection, including culture for mycobacterium, was negative; chest x ray findings were normal, but a computed tomography (CT) scan indicated nodular lesions in the liver and spleen as well as mediastinal lymphadenopathies. The diagnosis was made by histology and culture of mediastinal lymph node biopsy specimens. Both patients recovered slowly but completely with isoniazid (300 mg/day), rifampicin (600 mg/day), pyrazinamide (1500 mg/day), and ethambutol (1600 mg/day) treatment for six months. Infliximab treatment was stopped in these patients.
Two patients developed a procedure related severe infection. One patient with AS had an extensive wound infection after a triple arthrodesis of the ankle. Culture of the wound fluid was positive for Staphylococcus aureus. The wound was debrided surgically, followed by IV treatment with amoxycillin (2 g/day). The other patient, a 26 year old man with uSpA, had a needle arthroscopy of the knee at week 1 and developed an acute arthritis of the knee one day after this procedure. Because of the acute onset after an invasive procedure and the high inflammatory parameters (C reactive protein level (CRP) of 1.316 mg/l), this was considered to be, and treated (oxacillin IV, 2 g/day) as, a septic arthritis, although culture and polymerase chain reaction (based on broad range amplification of bacterial DNA) of the synovial fluid remained negative. Although the patient recovered fully within 48 hours, the antibiotic treatment was maintained for six weeks.
One patient with AS had a sepsis at week 37, presenting with high fever, frissons, and a CRP level of 1.36 mg/l. All cultures of blood, urine, and sputum remained negative. A classical x ray examination and CT scan of the neck, thorax, and abdomen could not indicate a focus. Because there was a poor clinical and biological response to amoxycillin IV (2 g/day), treatment was switched to vancomycin IV (2 g/day), leading to a rapid and complete recovery.
Finally, three patients developed retropharyngeal abscesses during infliximab treatment. Considering the particular presentation and severity, these cases will be described in more detail.
Retropharyngeal abscesses
Case 1
In 1993 a diagnosis of SpA, subtype PsA, was made in a 41 year old female patient with asymmetrical arthritis, distal interphalangeal joint involvement, ankylosis of several finger joints, and absence of rheumatoid factor. Because of persistent clinical and biological disease manifestations despite treatment with methotrexate and non-steroidal anti-inflammatory drugs (NSAIDs), she was included in the first cohort of infliximab treatment, consisting of intravenous infusion of 5 mg/kg at weeks 0, 2, 6, and from then on every 14 weeks. There was a good clinical and biological response until week 48. After the sixth infliximab infusion she developed high fever, frissons, dysphagia, and pharyngeal pain. Clinical examination showed a severally ill patient with a red and painful swelling of the left m. sternocleidomastoideus, surrounded by diffuse erythema. Relevant laboratory findings were an erythrocyte sedimentation rate (ESR) of 52 mm/1st h, a leucocytosis of 14.4×109/l, and a CRP level of 2.59 mg/l. Haemocultures were positive for Streptococcus pyogenes; urine and sputum cultures remained negative. Flexible laryngoscopy indicated swelling of the left sinus piriformis. Ultrasonography and a CT scan showed a flegmonal myositis of the left m. sternocleidomastoideus with an abscess anterior of the large blood vessels and surrounding cellulitis; the myositis extended to the m. sternohyoideus, m. sternothyroideus, and m. omohyoideus of the left and right neck region and even to the right m. sternocleidomastoideus (fig 1). Treatment with intravenous antibiotics (penicillin 6 g/day and clindamycin 1200 mg/day) for 14 days, followed by oral antibiotics, induced a gradual improvement of the systemic and local disease signs and normalisation of the inflammatory parameters.

CT scan of the neck in a patient with PsA developing a retropharyngeal abscess during infliximab treatment: flegmonal myositis of the left m. sternocleidomastoideus with an abscess in the retropharynx and anterior of the large blood vessels. The myositis extends to the m. sternohyoideus, m. sternothyroideus, and m. omohyoideus of the left and right neck region and even to the right m. sternocleidomastoideus.
Case 2
A 32 year old man with AS (inflammatory low back pain, bilateral sacroiliitis, axial ankylosis, HLA-B27 positive) presented with severe inflammatory low back pain and persistently high inflammatory parameters despite treatment with sulfasalazine and NSAIDs. In February 2000 he was enrolled in the infliximab study, resulting in a rapid clinical and biological response which was sustained over 15 months. Two weeks after the seventh infusion of infliximab, he complained of increasing pain in the cervical region. The pain was slightly different from previous inflammatory cervicalgia, with exacerbation by rotation and flexion of the neck as well as by swallowing. Moreover, there was general malaise and one episode of fever. Clinical examination confirmed the painful rotation and flexion of the neck and showed a moderate painful swelling of the right m. sternocleidomastoideus. Laboratory findings indicated an ESR of 106 mm/1st h, a leucocytosis of 13.6×109/l, and a CRP level of 2 mg/l. Microbiological analysis of blood, urine, and sputum was negative. Flexible laryngoscopy showed a clear swelling of the retropharyngeal region, which was confirmed by ultrasonography. Magnetic resonance imaging indicated the presence of a large retropharyngeal abscess, extending from the level of vertebra C1 to C7 and to the right m. sternocleidomastoideus. Again, the clinical, biological, and radiological signs improved and normalised after intravenous treatment with antibiotics (amoxycillin 2 g/day) for three weeks, followed by oral antibiotics.
Case 3
A 28 year old male patient was included in the infliximab study in December 1999 because of treatment resistant AS. The diagnosis was made more than 10 years ago, based on inflammatory low back pain, sacroiliitis grade III, HLA-B27 positivity, peripheral synovitis, uveitis, and microscopic gut inflammation. Clinical and biological signs improved rapidly and clearly with infliximab treatment, which was maintained for more than two years. At week 122 of infliximab treatment, the patient had two episodes of angina, which resolved with oral antibiotics. Two weeks later he presented with pain of the throat and difficulties on swallowing. There was no fever or general malaise. Clinical examination showed swollen and purulent tonsils. Laboratory findings indicated an ESR of 39 mm/1st h, no leucocytosis, and a CRP level of 0.86 mg/l. Because there were no signs of generalised infection, haemocultures were not performed. A CT scan showed bilateral enlarged tonsils with abscess formation and extension to the retropharynx. The tonsils were removed surgically and the patient was treated with amoxycillin IV (2 g/day). He recovered rapidly and infliximab treatment could be restarted.
Minor bacterial infections
Six minor infections with clear bacterial focus were observed: two cases of tooth abscesses (one in a patient with AS and one in a patient with PsA) and one case each of anal abscess (patient with AS), erysipelas (patient with AS), pneumonia (patient with AS), and pyelonephritis (patient with AS) (table 2). These infections occurred between weeks 10 and 72 of treatment, and all patients were receiving 5 mg/kg infliximab without concomitant treatment. None of these infections required admission to hospital and all patients recovered rapidly with oral antibiotics. Infliximab treatment could be continued in all cases.
Malignancies
One patient with PsA developed a spinocellular carcinoma of the skin, located on the ear, at week 82 of infliximab treatment. Treatment was interrupted for three months and the carcinoma was resected curatively. Treatment could then be restarted without further problems. There were no other cases of malignancies.
Immune mediated side effects
Two cases of infusion reactions were observed. A patient with PsA developed general malaise, flushing, dyspnoea, and a drop in blood pressure at the fourth infusion. The infusion was immediately stopped and the symptoms regressed rapidly. At the following infusions she was pretreated with corticosteroids; there was no relapse of symptoms. The second patient (AS) developed a mild infusion reaction at the fifth infusion, characterised by flushing, redness, nausea, and headache. There was no drop in blood pressure. These symptoms disappeared spontaneously when the infusion was stopped and did not require treatment with antihistamines or corticosteroids. Moreover, the symptoms did not relapse at the next infusion, indicating that this event was probably not a genuine allergic infusion reaction.
No cases of demyelinating or neurological diseases or lupus-like syndromes were seen, although more than 90% of the patients developed ANA.16
Palmoplantar pustulosis
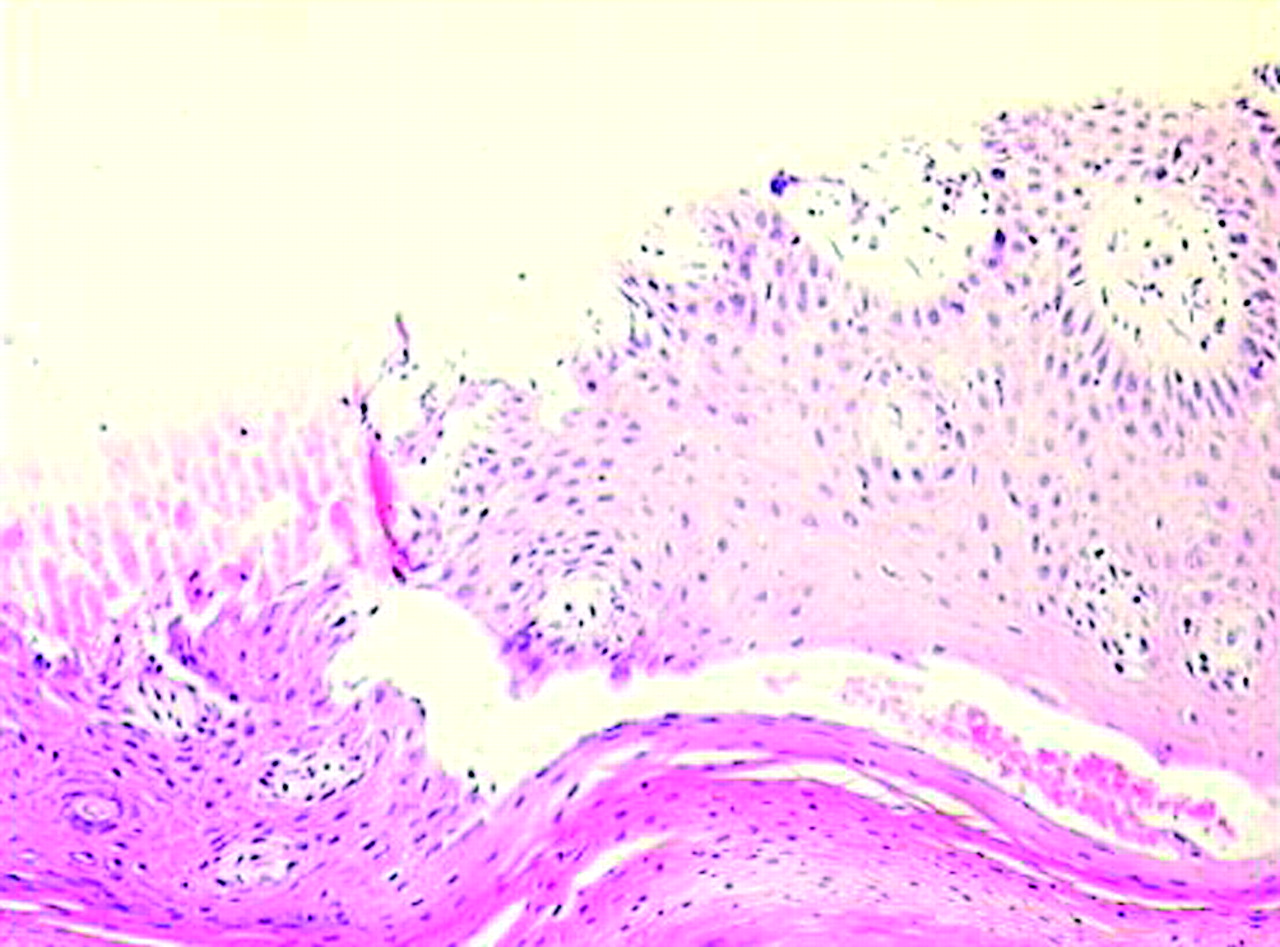
Three HLA-B27+ patients with AS developed palmoplantar pustulosis at weeks 13, 34, and 23 of infliximab treatment, respectively. None of the patients had a personal or familial history of psoriasis. The clinical picture was characterised by dark erythema with squamocrustae, pustules, and dried vesicles on hands and feet. Biopsies of the affected skin in two of these patients showed an enlarged epidermis with hyperorthokeratosis and parakeratosis, subcorneal pustules, discrete infiltration with polymorphonuclear cells, and perivacsular infiltration with lymphocytes; there was no clear spongiosis (fig 2). Cultures, including yeasts, were negative. In two of the three patients the lesions disappeared almost completely within 10 days of local treatment with corticosteroids, and infliximab treatment could be continued, whereas in the other patient the lesions persisted for four months despite local treatment.
{kind=link}
{kind=link}
Skin biopsy of a patient with AS who developed palmoplantar pustulosis, showing enlarged epidermis with ortho- and parakeratosis and perivascular infiltration by lymphocytes. There is no clear spongiosis. Haematoxylin-eosin staining, magnification ×160.
DISCUSSION
SpA is becoming a new indication for anti-TNFα treatment, with two double blind, placebo controlled studies showing a major therapeutic effect of infliximab in this disease.12,13 Because short and long term safety is of fundamental importance, the availability of a unique, monocentric cohort of 107 patients with SpA treated with infliximab for a total number of 191.5 patient years prompted us to provide a systematic and comprehensive review of the observed side effects. The overall safety profile indicates 5.2 serious adverse events per 100 patient years. Thus, 10/107 (9%) patients had a serious adverse event during infliximab treatment, with 8/107 (7%) patients having a severe infection (4.2/100 patient years). This led to treatment being stopped in five (5%) patients. However, the interpretation of these data is complicated by the fact that there are no good safety data available in a matched control SpA population. Despite the fact that infections have been repeatedly implicated in the pathogenesis of the disease, extensive epidemiological data on the spontaneous occurrence of severe infections in SpA are not available. Moreover, in both the Belgian and the German placebo controlled, double blind trials with infliximab in SpA,12,13 the placebo groups were switched to active treatment after a relatively short period of 12 weeks. Pooling the data of both studies, no serious adverse events or severe infections were seen in the placebo group during 12.7 patient years, but this period is probably not long enough to procure reliable figures.
Alternatively, the safety data in SpA of the present study can be compared with safety data of infliximab treatment in RA and CD. The ATTRACT trial, in which 341 patients with RA were treated with 3–10 mg/kg infliximab every 4–8 weeks during a follow up of 54 weeks, indicates the occurrence of about 15 serious adverse events and six severe infections per 100 patient years.17 Interpretation might be hampered by slightly different treatment schedules and the concomitant methotrexate treatment in the ATTRACT trial, but these data tend to indicate that non-infectious serious adverse events are more common in patients with RA treated with infliximab whereas severe infections are as common in SpA as in RA. In CD, one recent trial reported the safety of 5 and 10 mg/kg infliximab every eight weeks over one year in, respectively, 193 and 192 patients.18 A total of 25 serious adverse events per 100 patient years were reported, of which 7/100 patient years were described as reasonably related to treatment. The occurrence of severe infections was 3.2/100 patient years. Although this figure is in the same range as that found in the present study, the occurrence of other treatment related adverse events such as infusion reactions in CD (21/100 patient years) was clearly more common than in the present SpA cohort.
From a clinical point of view, three observations deserve particular attention. Firstly, there were only two serious adverse events of non-infectious origin in this SpA cohort: the occurrence of a spinocellular carcinoma of the skin, which was probably more related to excessive sun exposure in this particular patient than to the treatment, and a genuine infusion reaction. There were no other cases of malignancies or any case of heart failure; other immune mediated adverse events were restricted to one additional mild infusion reaction that, as previously reported in RA,2 was easy to manage. Because there are at present no data on human antichimeric antibodies (HACAs) in SpA during infliximab treatment, mainly owing to the technical difficulty of assessing HACAs reliably, it remains difficult to speculate on a possible relationship between HACAs and infusion reactions in SpA. Although a recent study in CD indicates that HACAs are indeed related to the occurrence of infusion reactions and that both HACAs and infusion reactions are more commonly seen in patients without concomitant immunosuppressive drugs,19 further studies on this issue in SpA should consider that infusion reactions are scarce and mostly easy to handle, that drugs such as methotrexate and systemic corticosteroids have no proven efficacy and are thus not commonly given in SpA, and that the potential benefit of concomitant drugs on HACAs should be balanced against a possible increase of other adverse events. As to other immune mediated adverse events, there were no cases of lupus-like syndromes despite the appearance of ANA in a large majority of the patients. A detailed analysis of a subgroup of these patients (n=35) over 34 weeks indicated a significant induction of both ANA (from 6/35 to 31/35 patients) and anti-dsDNA antibodies (from 0/35 to 6/35 patients) by infliximab treatment, indicating that the development of ANA and anti-dsDNA antibodies was as frequently observed in SpA as in RA.6,16 Of interest, the anti-dsDNA antibodies were always of the IgM or IgA subtype, whereas it is known that lupus is essentially associated with anti-dsDNA IgG.16 Although the induction of these antibodies indicates that further careful follow up is mandatory, the present study does not provide evidence for the induction of lupus-like syndromes by infliximab in SpA.
Secondly, there were two cases of disseminated tuberculosis, probably by reactivation. These patients were included in the study before the increased occurrence of tuberculosis in patients with RA treated with infliximab had been generally recognised; at that time patients were not screened systematically with skin testing and chest x ray examination before the start of the treatment. The clinical presentation and the timing (within 10 weeks after the start of infliximab) were similar to those described in patients with RA treated with infliximab.8 This confirms that TNFα blockade interacts with the defence against mycobacteria independently of the underlying chronic disease. Therefore, it is likely that the same prevention and therapeutic strategies might be applied to patients with SpA as is used in RA, and thus that patients with SpA should be screened for tuberculosis with a chest x ray examination and, if this is normal, a skin test, before starting infliximab treatment. Although there are no prospective studies on how to handle patients with previous tuberculosis infection, it has been suggested by different committees that the start of infliximab treatment should be delayed for at least four weeks and treatment with isoniazid for six months started in all patients with suggestive chest x ray findings or skin test who have had no previous adequate antituberculosis treatment.
Thirdly, both the severe infections and the mild infections with clear bacterial focus occurred in all SpA subtypes, independently of age, sex, HLA-B27 status, concomitant treatment, or dosage and duration of infliximab treatment. Although future analysis of larger cohorts may provide some evidence for specific clinical or epidemiological risk factors, this implies, on the one hand, an urgent need for alternative biological measures that could help to identify patients at risk for developing infectious adverse events, and on the other, the absolute necessity of a strict clinical follow up and aggressive diagnostic investigations, even in patients with minimal clinical suspicion. This is highlighted by the three cases of retropharyngeal abscesses, which were not only potentially life threatening but also difficult to recognise in patients with SpA with pre-existing neck pain and high inflammatory parameters.
From a pathogenetic point of view, the occurrence of retropharyngeal abscesses (with in at least one patient Streptococcus pyogenes as the causative micro-organism) is intriguing because this kind of infection is not commonly seen in patients with SpA without TNFα blockade. Moreover, although an increased frequency of focal nasopharyngeal bacterial infections was described in patients with RA and CD treated with infliximab,17,18 this never led to abscess formation in these patients. Because tonsillitis and focal nasopharyngeal infections have been linked to palmoplantar pustulosis,20–22 it is intriguing that three patients with AS developed pustulosis palmaris and plantaris during infliximab treatment (none of these patients had a personal or family history of psoriasis). Streptococci may have a central role in this process through the activation of specific T cells, which can then induce the specific skin lesions.23,24 The exact role of TNFα remains unclear, but it is known that TNFα mediates the production of interferon gamma by group B streptococcus treated mononuclear cells25 and that palmoplantar pustulosis is associated with polymorphisms in the TNF gene.26 Thus, blocking TNFα might impair the cellular defence against streptococci and thereby indirectly contribute to the development of palmoplantar pustulosis. Alternatively, the occurrence of palmoplantar pustulosis might be associated with Proprionibacterium acnes.27,28
These six cases of retropharyngeal abscesses or palmoplantar pustulosis provide further circumstantial evidence that patients with SpA have some kind of specific impairment of their antibacterial immune defence. Indeed, in both ReA and HLA-B27 transgenic rats, immune activation by bacteria was previously shown to have a crucial role in the development of the disease. At least in ReA, there is evidence that this is related to an abnormal persistence of intracellular pathogens. Recent studies indicate that other subtypes of SpA also may have an impairment of certain aspects of the innate immune defence, particularly with regard to the expression of scavenger receptors.29,30 However, whereas SpA has classically been associated with urogenital infection with chlamydia or gastrointestinal infections with Gram negative pathogens such as salmonella, shigella, campylobacter, and yersinia, the present data indicate that focal nasopharyngeal infections with Gram positive bacteria such as streptococci may also play a part in the disease.
Acknowledgments
The authors express their sincere gratitude to Professor Dr Koen Verstraeten (MD, PhD, Department of Radiology, Ghent University Hospital, Belgium) for the radiological screening and follow up, and Dr Freddy Cornillie (MD, PhD, Centocor, Belgium) for the continuous support.
REFERENCES
Footnotes
-
Dominique Baeten is a senior clinical investigator of the fund for scientific research, Vlaanderen (FWO-Vlaanderen).