Article Text

Abstract
Background: Chemokines and their receptors are considered important contributors in cell migration and inflammation in chronic inflammatory disorders. Chemokines affecting monocytes/macrophages are considered potential therapeutic targets, but no studies of the effects of blocking the chemokine repertoire in humans with a chronic inflammatory disease have been reported.
Objective: To carry out a double blind, placebo controlled, phase Ib clinical trial with a specific, oral CCR1 antagonist.
Methods: 16 patients with active rheumatoid arthritis (RA) were randomised 3:1 to active:placebo treatment for 14 days. Synovial biopsy specimens were obtained on days 1 and 15. Immunohistochemistry was used to detect the presence of various cell types before and after treatment and the results measured by digital image analysis. Results before and after treatment were compared by paired t test, and a two sample t test was used to compare the changes from baseline in the two groups.
Results: All patients completed the study. A significant reduction in the number of macrophages (p=0.016), intimal macrophages (p=0.026), and CCR1+cells (p=0.049) in patients treated with the chemokine antagonist compared with the placebo group occurred in the synovium. Significant decreases in overall cellularity, intimal lining layer cellularity, CD4+ T cells, and CD8+ T cells also occurred in treated patients. Cells lacking CCR1 were not affected. Trends towards clinical improvement were seen in the treated patients but not in the placebo group. Severe side effects were not reported.
Conclusion: Specific chemokine receptor blockade can result in relevant biological effects in patients with active RA.
- rheumatoid arthritis
- CCR1
- chemokine blockade
- synovium
- ACR, American College of Rheumatology
- DAS, disease activity score
- DMARDs, disease modifying antirheumatic drugs
- HAQ, Health Assessment Questionnaire
- OPC, oral powder for constitution
- RA, rheumatoid arthritis
- SF, synovial fluid
- ST, synovial tissue
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- DAS, disease activity score
- DMARDs, disease modifying antirheumatic drugs
- HAQ, Health Assessment Questionnaire
- OPC, oral powder for constitution
- RA, rheumatoid arthritis
- SF, synovial fluid
- ST, synovial tissue
Rheumatoid arthritis (RA) is a chronic inflammatory disease that affects synovial tissue (ST) in multiple joints. Although its aetiology is still unknown, RA is thought to be an autoimmune disease. Severe morbidity and structural damage of joints advocates early and effective treatment.1 Treatment with combinations of disease modifying antirheumatic drugs (DMARDs) can induce clinical remission and may inhibit erosive disease.2 However, these agents are only moderately effective, and severe side effects and poor long term toleration have been reported.3 This rationalises the search for more effective and less toxic agents in the treatment of this disease. New targeted therapies, such as tumour necrosis factor α blockade, have improved the therapeutic possibilities, but not all patients respond.4
Chemokines are a specialised family of small cytokines (8–10 kDa) that act as potent mediators of inflammation by their ability to recruit and activate specific leucocyte subpopulations.
Several chemokines have been described in RA ST and synovial fluid (SF) including many of the CC chemokines, among which are CCL3 (macrophage inflammatory protein-1α) and CCL5 (regulated-upon-activation-normal-T-cell-expressed-and-secreted (RANTES)).5–7 Macrophages and T lymphocytes in the ST are a major source of these chemokines.5,6,8 Chemokines activate leucocytes by binding to specific serpentine G-protein coupled, cell surface receptors on target cells, and thus far 12 CC receptors have been reported.9,10 CCR1 positive cells are scattered throughout the synovium and most of the CCR1 positive cells are macrophages.11
Antibodies to chemokines and chemokine inhibitors have been considered to be interesting potential therapeutic tools in chronic inflammatory disorders since the discovery of their existence. In vitro experiments have shown that blocking of the most powerful ligands of CCR1—CCL3 and CCL5—with neutralising antibodies may inhibit the chemotactic activity in RA SF.5,6,12,13 In vivo experiments blocking the ligands of CCR1, or antagonising the CCR1 receptor itself, in animal models of arthritis showed that pretreatment prevents inflammation in the synovium and reduces the development of joint destruction as well as the severity of symptoms.14,15 These and other data provide the rationale for the development of a specific CCR1 antagonist as a potential treatment for RA.
In this study chemokine blockade was studied for the first time in humans. The objective was to provide initial evidence of safety and proof of concept. We conducted a double blind, placebo controlled clinical study with an orally available compound in patients with RA and saw a marked decrease in synovial inflammation and trends towards a decrease in clinical disease activity after only two weeks’ treatment.
PATIENTS AND METHODS
Patients
Over a period of eight months 16 patients, aged 18–80, were included if they met the criteria of the American College of Rheumatology (ACR) for the diagnosis of RA.16 We included patients with a disease duration of at least six months and active disease despite their possible current drug treatment. Patients were allowed to use certain DMARDs (methotrexate (no more than 15 mg/week), hydroxychloroquine, or sulfasalazine), provided that such treatment had been without significant renal, hepatic, gastrointestinal, haematological, or dermatological toxicity, and the dose/schedule had been stable for at least two months before entry. Patients were also allowed to receive corticosteroid treatment equivalent to an average dose of prednisone ⩽10 mg/day, provided that the dose had been stable for at least two months before entry. Non-steroidal anti-inflammatory drugs were allowed, provided that the dose and frequency had been stable for 30 days. Patients were excluded if they had severe physical incapacity (Steinbrocker class IV).17 Other exclusion criteria were concomitant requirement for an immunosuppressive agent such as azathioprine or cyclosporin; first manifestation of RA before 16th birthday; clinically significant concurrent neurological, haematological, renal, hepatic, endocrine, pulmonary, or cardiovascular disease (that is, not controlled by a stable therapeutic regimen); concomitant treatment with another investigational drug in the past 30 days; any screening laboratory deviations more than 30% from upper or lower limits of the normal range for liver function tests, white blood cell counts outside the normal limits, haemoglobin and packed cell volume outside the ranges typical for a patient with RA (that is, ⩾30%), severe thrombocytopenia (⩽100×109/l), thrombocytosis (⩾750×109/l), or abnormal renal function tests (that is, blood urea nitrogen or creatinine more than 10% above the upper limits of normal). Female patients of childbearing age used effective methods of birth control and had a negative pregnancy test before entry. Pregnant or nursing mothers were not included.
Study protocol
The medical ethics committee of the Academic Medical Centre from the University of Amsterdam approved the study protocol. All patients included were from this centre. Before the start of the study, patients gave written informed consent, had a complete medical history taken, and underwent a full physical examination. A haematology and serum chemical profile were obtained and analysis of a clean-catch urine specimen was also completed as well as an electrocardiogram. Patients had active disease, which was defined as the presence of at least three of the four following characteristics: six or more painful/tender joints, three or more swollen joints, at least 45 minutes of morning stiffness, and C reactive protein ⩾2 mg/l. After this initial screening, eligible patients were included in the study within four weeks. Clinical assessment for disease activity was repeated at baseline (before the arthroscopy) and at days 8, 15, and 18. This included a 28 joint count for joint swelling and tenderness, doctor’s and patient’s assessment of disease activity on a scale from 1 (asymptomatic) to 5 (severe symptoms), pain assessed by a visual analogue scale from 0 (no pain) to 100 (severe pain), quality of life (Health Assessment Questionnaire (HAQ)) from 0 (no disability) to 3 (severe disability), and the erythrocyte sedimentation rate. The same independent assessor who was also unaware of the laboratory results performed the clinical evaluation. Monitoring for adverse events occurred daily during the study and thereafter by interviews, physical examination, and laboratory testing. After the end of treatment on day 15, patients were seen for follow up on day 18 and followed up for another four weeks.
Study drug
A “blinded” pharmacist randomly allocated the patients in a ratio of 3:1 to receive either the CCR1 antagonist or the placebo. This ratio was chosen to optimise power for estimation of side effects related to CCR1 antagonist treatment. The CCR1 antagonist was used as an oral powder for constitution (OPC) and was reconstituted in polysorbate 80 and sterile water. The placebo OPC mimicking the dose of the CCR1 antagonist was a blend of cellulose, magnesium stearate, and sodium lauryl sulphate and was reconstituted with sterile water containing denatonium benzoate and polysorbate 80. The characteristics and taste of the CCR1 antagonist and placebo were identical. Treatment was given for 14 sequential days with a dose of 300 mg (given every eight hours), based on effects seen in murine models and chemotactic activity in RA SF in an in vitro chemotaxis model.
Arthroscopy
Arthroscopy under local anaesthesia was performed in all patients at baseline before treatment and at day 15 after treatment. Arthroscopies, tissue sampling, and storage were performed as described previously in detail.18
Immunohistochemical analysis
Serial sections were stained with the following monoclonal antibodies: anti-CD68 (EBM11, Dako, Glostrup, Denmark), anti-CD3 (SK7, Becton-Dickinson, San Jose, CA), anti-CD4 (SK3, Becton-Dickinson), anti-CD8 (DK25, Dako), anti-CD22 (CLB-B-Ly/1, Central Laboratory of the Netherlands Red Cross Blood Transfusion Service, Amsterdam, The Netherlands), anti-CD138 (IM-2757, Beckman Coulter, Marseilles, France), anti-CD55 (Clone-67, Serotec, Oxford, UK), and anti-CCR1 (MAB145, R&D systems Europe Ltd, Abingdon, UK). Sections with non-assessable tissue, defined by the absence of an intimal lining layer, were omitted before analysis. For control sections, the primary antibodies were omitted or irrelevant isotype matched mouse antibodies were applied (antihuman immunodeficiency virus, a gift from TNO, Rijswijk, The Netherlands). Staining was performed according to a three step immunoperoxidase method as previously described.19
Digital image analysis
The slides were evaluated by digital image analysis. All sections were coded and analysed in a random order by an independent observer (JJH) who was unaware of the clinical data as described previously.20
Statistical analysis
The results before and after treatment were compared by the paired t test. In addition, a two sample t test was used to compare the changes from baseline in the two groups. The authors performed data acquisition, data entry, database management, and data analysis.
RESULTS
Demographic features
Four men and 12 women were included in the trial. Their mean age was 53 years and all patients had active disease despite using DMARDs. The placebo group comprised one man and three women with a mean age of 50 years (range 25–61) and the CCR1 antagonist treated group comprised three men and nine women with a mean age of 57 years (range 43–79). The patients in the placebo group had a mean disease duration of 42 months; mean disease activity score (DAS) of 4.69 (range 3.43–6.06), and 50% of the patients were rheumatoid factor positive. The patients in the CCR1 antagonist group had a mean disease duration of 87 months (range 6–336 months); a mean DAS of 5.58 (range 4.31–6.95), and 58% of these patients were rheumatoid factor positive. The DMARD treatment in the two groups was as follows: in the placebo group all patients used methotrexate and one of them also used low dose prednisone; in the CCR1 antagonist group nine patients used methotrexate (three in combination with hydroxychloroquine or low dose prednisone), two patients only used sulfasalazine, and one patient only used hydroxychloroquine. There were no significant differences in age, sex ratio, disease duration, and concomitant use of DMARDs, but patients in the treated group were on average seven years older and had 45 more months of disease duration. All patients had active disease at entry, as judged by the presence of multiple tender and swollen joints, pain assessed on a visual analogue scale, raised acute phase reactants, morning stiffness, subject’s as well as doctor’s global assessment of disease activity, and as calculated by the DAS.21 Comparison of the clinical and laboratory indices of disease activity between the two groups on the day of entry showed only higher scores for tender and swollen joints in the treated group.
Safety and tolerability
The compound was well tolerated and all 16 patients completed the study. No severe adverse events were reported. Minor adverse events related or potentially related to the compound were nausea after drug intake (n=1), which also occurred in the placebo group (n=1) and might be explained by the bitterness of the OPC. Mild transient ankle oedema (n=1) and a resolving rash (n=1) were also reported in the treated group. No major abnormalities in haematological findings or serum chemical findings were noted during or after the study.
Clinical efficacy
Table 1 summarises the characteristics of the clinical efficacy. Four patients (one patient from the placebo group and three from the CCR1 antagonist group) were non-responders and received intra-articular corticosteroids on day 15. The data of day 15 (before receiving corticosteroids) were used for comparison between day 1 and day 18 for these four patients. There were, on average, no significant differences in change between the placebo group and the active treated group. The treated group did show statistically significant clinical improvement in the number of tender joints (p=0.021), swollen joints (p=0.001), quality of life (HAQ, p=0.037), and in the DAS (p=0.012) after treatment. Whereas in the placebo group there was no significant clinical improvement in any of the parameters. According to the ACR response criteria22 at day 18, four patients (33%) treated with the CCR1 antagonist had at least 20% improvement, but none of the controls.
Clinical data
Immunohistochemical analysis
Table 2 shows the results of the immunohistochemical analysis at baseline and after two weeks of treatment. Staining was negative in control sections, where the primary antibody was omitted or irrelevant antibodies were applied. After CCR1 blockade there was on average a decrease in the treated group in the number of CD68+ macrophages of 34% (SEM 4%) (p=0.016), intimal lining layer CD68+ macrophages of 41% (SEM 5%) (p=0.026), and CCR1+ cells of 66% (SEM 84%) (p=0.049), compared with the placebo group where there was on average an increase of 15% (SEM 5%), 28% (SEM 13%), and 35% (SEM 5%), respectively (figs 1 and 2). When the changes within each treatment group were compared before and after treatment there was also a significant reduction in the treated group in overall cellularity (reduction from 1795 (423) (mean (SEM)) to 967 (164); p=0.013), intimal lining layer cellularity (423 (95) to 209 (49); p=0.048), CD4+ T cells (666 (159) to 358 (139); p=0.023), and CD8+ T cells (157 (44) to 84 (31); p=0.024). There was no significant change in any of the measured cell types in the placebo group. The number of CD22+ B cells, CD138+ plasma cells, and CD55+ fibroblast-like-synoviocytes did not change in either group, suggesting that only cells that are capable of expressing CCR1 were affected. Figures 3, 4, and 5 show representative examples of immunohistochemical staining before and after treatment. Figure 6 shows an example of an isotype-specific negative control.
Data on synovial tissue analysis before (mean (SEM)) and after (mean (SEM)) treatment and the percentage change (mean (SEM)) in the placebo group and the CCR1 antagonist treated group compared with baseline. Data represent total cell count in 18 high power fields corrected for the percentage of actual tissue in the analysed areas for cellularity, CD68+ macrophages, CD4+ lymphocytes, CD8+ lymphocytes, CCR1+ cells, CD22+ lymphocytes, CD55+ fibroblasts, and CD138+ plasma cells

Significant decrease after CCR1 blockade therapy compared with placebo in the mean number (SEM) of (A) overall CD68+ cells (p=0.016), (B) intimal lining CD68+cells (p=0.026), and (C) CCR1+ cells (p=0.049) for the CCR1 antagonist group and the placebo group.

Expression of overall CD68+ cells (A), CD68+ lining cells (B), and CCR1+ cells (C) in paired synovial biopsy specimens after CCR1 blockade or placebo for the individual patients.
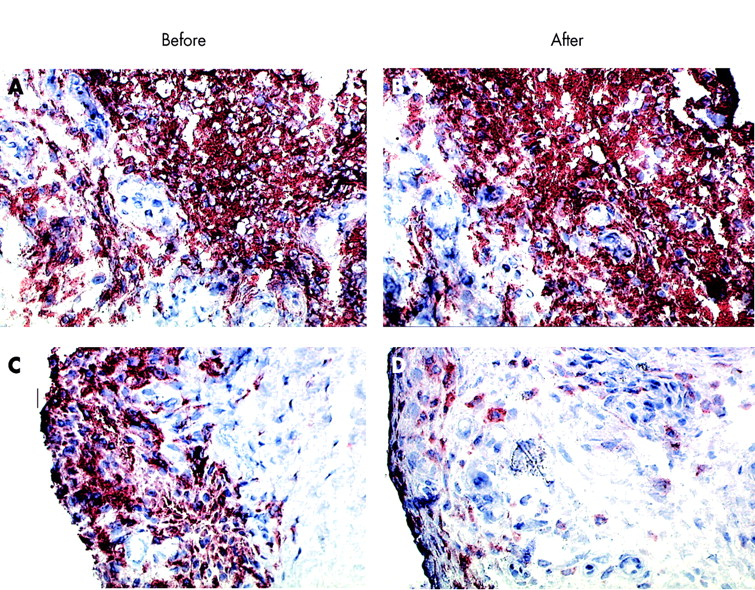
Representative synovial expression of CD68+ macrophages before and after treatment for a placebo patient (A, B) and a treated patient (C, D). Original magnification ×400.

Representative synovial expression of CD4+ lymphocytes before and after treatment for a placebo patient (A, B) and a treated patient (C, D). Original magnification ×400.

Representative synovial expression of CCR1+ cells before and after treatment for a placebo patient (A, B) and a treated patient (C, D). Original magnification ×400.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Isotype-specific negative control. Original magnification ×200.
DISCUSSION
This study shows that in a short term treatment chemokine receptor blockade seems to be a safe and potentially effective treatment for patients with a chronic inflammatory disease. This confirms the importance of chemokines and chemokine receptors in cell trafficking and offers a completely new approach for the treatment of these disorders. This study describes for the first time the pronounced effect of chemokine receptor blockade on the features of ST in patients with RA.
To date none of the available treatments are curative for RA and despite the optimal use of current antirheumatic therapy there still is a need for better treatments. In the search for more effective targeted therapies, new strategies aimed at blocking key mediators in the inflammatory process have been described.4,23 This has stimulated the search for new biological molecules that might be targeted in order to treat RA safely and effectively. There is especially a need for targeted small molecules, which have the advantage that they can be taken orally.
Chemokines and their receptors have a central role in the recruitment of leucocytes into the inflamed tissue and the perpetuation of inflammation.24,25
Numerous studies described the presence of chemokines and their receptors in the synovial compartment of patients with RA and other forms of arthritis.11,25–28 CCR1 and its ligands CCL2, CCL3, CCL4, and CCL5 have been implicated in the pathogenesis of RA and other chronic inflammatory diseases.29,30 It has been suggested that CCR1 plays a part in the initial recruitment of monocytes to sites of inflammation.11 Successful blocking of the receptor and its ligands has been shown in in vitro models and in animal models for arthritis.6,12–15,31
We conducted a placebo controlled, double blind, randomised study to provide initial proof of concept. We studied 12 patients treated with CCR1 antagonist and four with placebo. A limitation of this study is the small study group, especially the number of control patients. To interpret the results it is important to note that previous work has shown that analysis of serial ST samples from patients with RA, who received either placebo or unsuccessful treatment with recombinant human interleukin 10, did not show any synovial changes.32 Similarly, there was no clear cut change in serial biopsy specimens after treatment with interleukin 1 receptor antagonist at 30 mg/day,33 which appears to have very limited effects on arthritis activity. Hence, this supports the view that it is unlikely that changes in serial biopsy samples can be explained by placebo effects, regression to the mean, expectation bias, or by the arthroscopy procedure itself, but likely that they reflect biological effects of the treatment. Consistent with this notion, on average, we found no decrease in synovial inflammation in the four patients who received placebo.
In synovial samples from patients treated with the CCR1 antagonist there was a significant decrease in the overall number of macrophages as well as in intimal lining layer macrophages and CCR1+ cells when the treated group was compared with the placebo group. There also was a significant reduction in overall cellularity, intimal lining layer cellularity, CD4+ T cells, and CD8+ T cells in the treated group. Cells not capable of expressing CCR1 (including CD22+ B-cells, CD138 plasma cells, and CD55+ fibroblast-like-synoviocytes) were not affected by the treatment. These results confirm the feasibility and specificity of CCR1 blockade in vivo. It should be noted, however, that synovial inflammation could occasionally be reduced in the absence of clinical improvement.19 Another study showed synovial changes in patients with only a modest decrease in serum levels of acute phase reactants.34 Taken together, these studies indicate that analysis of serial biopsy specimens can be used as a method to test new compounds requiring relatively small numbers of patients.
The clinical effects described in this study appear promising, even after short treatment. It should be noted that there were some differences in age, disease duration, and disease activity between the two groups. The patients in the CCR1 antagonist group were on average slightly older, had disease of longer duration, and tended to have more disease activity at baseline. It seems unlikely that these differences influenced the clinical response to treatment. Obviously, however, a meaningful clinical effect needs to be shown in larger, well controlled studies. This study provides the rationale for such trials.
Our study shows proof of principle of CCR1 blockade in patients with chronic inflammatory disease. Administration of an oral CCR1 antagonist resulted in a striking decrease in synovial inflammation. This may provide a completely new direction in the treatment of chronic inflammatory disorders and encourage future investigations and clinical trials aimed at inhibition of other important members of the chemokine repertoire, such as CCR1, CCR5, CCR2, CXCR3, monocyte chemotactic peptide-1, and others.11,24,26
Acknowledgments
Supported by Pfizer Inc, Groton, CT.