Article Text

Abstract
Objectives: To present the prevalence of self reported musculoskeletal diseases, the coexistence of these diseases, the test-retest reliability with six months in between, and the association with musculoskeletal pain symptoms.
Methods: Twelve layman descriptions of common musculoskeletal diseases were part of the questionnaires of a prospective cohort study of a random sample in the general Dutch population aged 25 years or more (baseline: n=3664, follow up after six months: n=2338). Data collection also included information about pain relating to five different anatomical areas.
Results: Osteoarthritis of the knee (men 10.1%, women 13.6%) was amongst the most reported musculoskeletal diseases, whereas the figures for self reported rheumatoid arthritis (RA) were 1.6% and 4.6% for men and women, respectively. The coexistence of these diseases is high: 47 of the 66 combinations were reported more often than would be expected if they were independent of each other (p<0.05). For most diseases the test-retest reliability was good (κ between 0.6 and 0.8), but for repetitive strain injury (κ=0.37) and chronic arthritis other than RA (κ=0.44) the agreement was fair to moderate. All complaints of pain were more often reported by those with musculoskeletal diseases than those without those diseases, and the pain pattern was disease-specific.
Conclusions: Self reported musculoskeletal diseases are highly prevalent, with a fair to good reliability and a disease-specific pain pattern. Health surveys are a limited but valuable source of information for this group of health problems, which is not available from most other sources of information.
- musculoskeletal pain
- population study
- pain
- epidemiology
- DMC3, Dutch population based Musculoskeletal Complaints and Consequences Cohort
- RA, rheumatoid arthritis
- RSI repetitive strain injury
Statistics from Altmetric.com
- DMC3, Dutch population based Musculoskeletal Complaints and Consequences Cohort
- RA, rheumatoid arthritis
- RSI repetitive strain injury
Musculoskeletal diseases are a major public health problem, but figures for the prevalence of most musculoskeletal disease are scarce, as was also mentioned in the framework for the Bone and Joint Decade 2000–2010.1 To describe the global burden of musculoskeletal conditions now and in the future is a central goal of the decade.
One method of gathering data on the prevalence of musculoskeletal conditions is by a population based survey asking questions on the existence of musculoskeletal diseases. Several examples of such surveys exist2–18; see also table 1. The number of musculoskeletal diseases varies among these surveys and so does the description of the diseases. Sometimes only “any form of arthritis or rheumatic disease” is used, sometimes a list of diverse musculoskeletal diseases, and most often one or two descriptions referring to musculoskeletal diseases are part of a long list of several chronic diseases. The estimated prevalence of musculoskeletal diseases varies between 2% and 65%, which is also affected by other survey design factors and the age of the study population.
Overview of prevalences of self reported musculoskeletal diseases from population-based surveys
To obtain a more detailed insight into the prevalence of the broad spectrum of musculoskeletal diseases, a population based study was carried out that included a list of 12 descriptions of common musculoskeletal diseases, for which we asked if a doctor had ever said that the respondent had the disease. In this paper we will present the prevalences of these self reported musculoskeletal diseases. We will also present the coexistence of these diseases, with the expectation that their coexistence is high. In addition, we studied the test-retest agreement in the reporting of musculoskeletal diseases with six months in between, which can be viewed as a measure of test-retest reliability because most musculoskeletal diseases are chronic. Finally, we will present the association between musculoskeletal pain symptoms and the reporting of musculoskeletal pain of different anatomical regions, which will provide further information about the meaning of self reported musculoskeletal diseases.
METHODS
Data of the Dutch population based Musculoskeletal Complaints and Consequences Cohort study (DMC3 study) were analysed.
Study population
The Dutch population in 1998 consisted of more than 15 million inhabitants, of whom more than 10 million were aged 25 years or more. A random sample of 8000 people aged ⩾25, stratified by 10 year age group and sex (equal numbers in each age-sex band), was taken from the population register of 1998, identical to general surveys of Statistics Netherlands.19 Data on sex, age, address, and marital status were available from the population register. The address data on the 12 provinces were used to construct four national regions: north, west, east, and south.
The net response was calculated by dividing the number of respondents by the number of those approached, excluding those who had died or whose address was unknown (n=182). The net response of the DMC3 study was 46.9% (n=3664). The response was slightly higher for women, for those in the middle age groups (45–64 years), and for those who were married (table 2).
Description of the sample and respondents of the DMC3 study (%)
People who signed an informed consent for follow up (n=2752) were approached after six months. Questionnaires with a baseline match on age and date of birth were assessed for 2338 (85%) respondents.
Questionnaire
For the baseline measurement we used a 28 page full-colour questionnaire that consisted of general questions and health questions. A list of musculoskeletal diseases was included in the same form as lists of chronic diseases commonly used in health surveys. A list of 12 diseases was included because the “check list method” produces higher and often more reliable numbers of diseases.20 The list was preceded by an introductory text of the form: “There are many diseases of the musculoskeletal system. Some are prevalent, some are rare. Please indicate whether a physician or medical specialist has ever told you that you have one or more of the following diseases.” Respondents were also asked whether they were (still) receiving treatment for the particular disease. Criteria for selection of the diseases were similar to general criteria for health surveys lists of chronic diseases20: (a) the disease should not be too rare. Some cases should be expected to be included in a survey of around 4000 people aged 25 years or more. For instance, ankylosing spondylitis was excluded; (b) the disease should be suitable for self reporting. A description of the disease which is not purely medical should be available or the disease should be expected to be well known among laymen. For example we did not use not “epicondylitis” but rather “tennis elbow” or “golfers’ elbow”. In the tables the descriptions used are given, with the exception of epicondylitis, RSI, osteoarthritis, osteoporosis and tendinitis or capsulitis. Repetitive strain injury (RSI) also included, for example, “a computer-arm”, osteoarthritis was also accompanied with “wear and tear”. Besides osteoporosis we used also the non-medical term on decalcification of bones, and for tendinitis or capsulitis we used “inflammation or condition of tendon or joint capsule”. In addition to the list of 12 diagnoses people could report two extra musculoskeletal diseases in an open question. Questions were asked on musculoskeletal pain in (a) neck, shoulder or higher part of the back; (b) elbow or wrist/hand; (c) lower part of the back; (d) hip or knee; (e) ankle and foot. The question had the form: Have you had pain in <anatomical area> during the past 12 months? To analyse generalised pain two different descriptions are used: definition 1 included those with pain in all areas, definition 2 included those with pain in the lower back and at least one of the upper extremities and lower extremities.
The follow up questionnaire was a slightly shorter version of the baseline questionnaire (22 pages) and also included the list of 12 layman descriptions of common diagnoses of musculoskeletal diseases.
Statistical analysis
To present an estimation of the prevalences of the musculoskeletal diseases for the Dutch population, weighting factors were used so that the distribution by age, sex, region, and marital status was equal to that of the Netherlands of 1998 (direct standardisation). Confidence intervals were calculated using the unweighted standard errors.
Whether or not the coexistence of musculoskeletal diseases was higher than might be expected if they were independent of each other was tested by Cochran-Mantel-Haenszel statistics with adjustment for age.
Cohen’s κ was calculated as a measure of agreement between reporting of diseases at baseline and follow up. The following ratings for the interpretation of κ were used: poor (κ<0.20), fair (0.21<κ<0.40), moderate (0.41<κ<0.60), good (0.61<κ<0.80), very good (0.81<κ<1.00), according to Altman.21
All analyses of data were performed using SAS version 6.12.
RESULTS
Table 3 presents the prevalence of musculoskeletal conditions. Of the Dutch population aged 25 years or more, 41% of the men and 48% of the women reported at least one musculoskeletal disease. The most commonly reported musculoskeletal diseases were “tendinitis or capsulitis” (15.4% of the men, 17.2% of the women) and “osteoarthritis of the knee” (10.1% of the men, 13.6% of the women).
Prevalence of self reported musculoskeletal diseases (%) in the Dutch population, including 95% confidence interval, DMC3 study (standardised)
With the exception of herniated disc of the back and gout, all diseases were more commonly reported by women than by men, especially osteoarthritis of the hip (3.9% of the men, 9.6% of the women) and osteoporosis (1.9% of the men, 9.9% of the women).
One fifth of the population reported a musculoskeletal condition that was not listed in the 12 descriptions. Most of these were (pain) complaints listed later in the questionnaire or fractures/accidents. Other mentioned diseases were osteoarthritis (19 times), sciatica (14), scoliosis (13), pelvis instability (8), herniated disc in the neck (8), ankylosing spondylitis (6), stroke (5), bursitis (5), Scheuermann’s disease (4), spondylitis, and some neurological diseases like chronic polyneuropathy (3), myasthenia gravis (2), and Méniére’s disease (2). Once only were mentioned, for instance, polymyalgia rheumatica, Dupuytren’s disease, hammer toe, psoriatic arthritis, Tietze’s syndrome, and Paget’s disease.
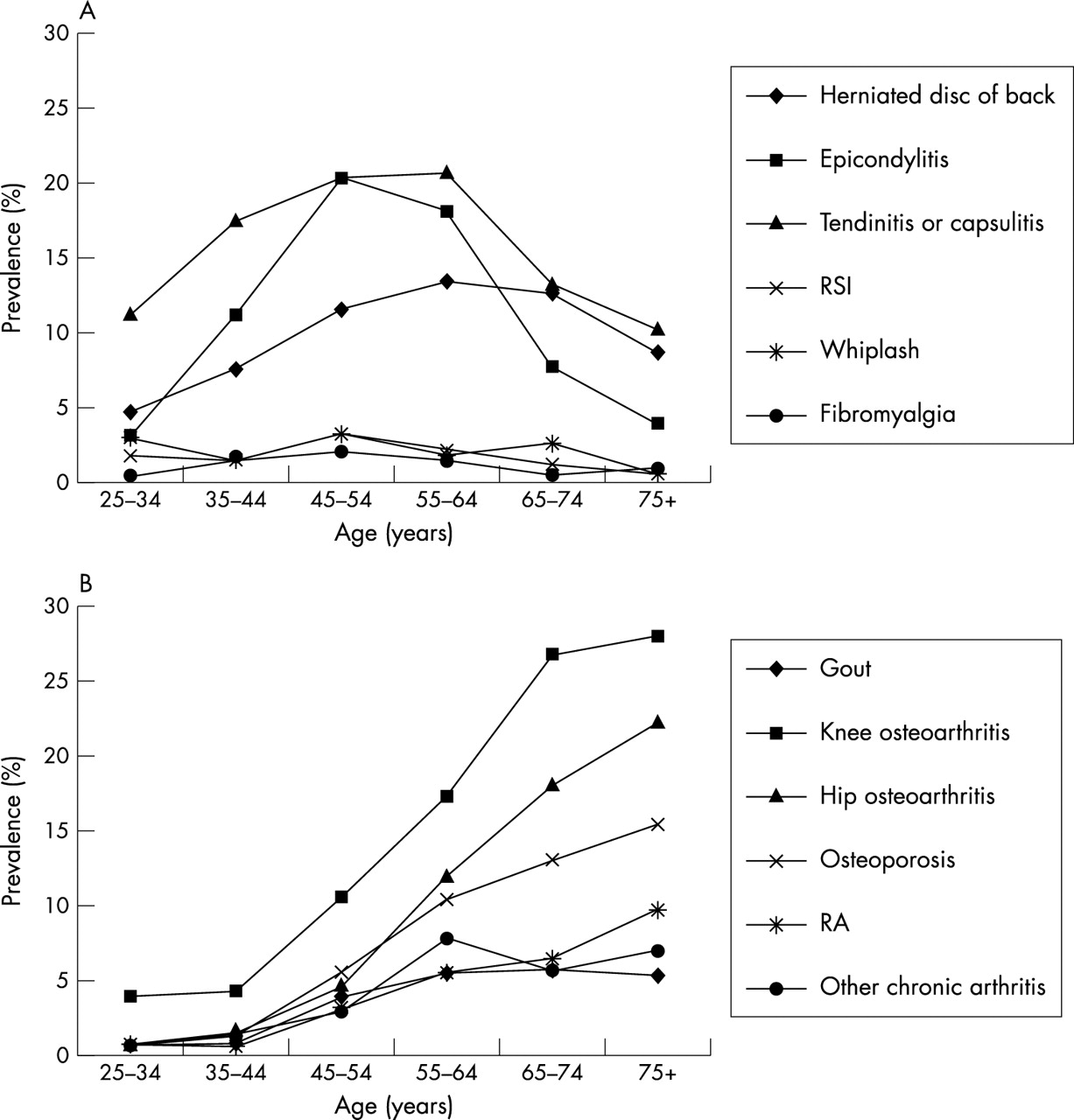
The prevalence of the following diseases increased with increasing age (fig 1): gout, knee osteoarthritis, hip osteoarthritis, osteoporosis, RA, and other chronic arthritis; these are the age related diseases. The prevalence of RSI, whiplash and fibromyalgia seemed to be independent of age, and for herniated disc of the back, epicondylitis and tendinitis, or capsulitis an inverse U-shape with age was found; these are age dependent diseases.

{kind=link}
Prevalence of self reportedmusculoskeletal diseases by age group. (A) Age dependent and non-age dependent diseases; (B) age related diseases.
On average, half of those reporting a musculoskeletal disease were (still) receiving treatment for the disease (table 3). Among women, this percentage varied from 36.8% for those reporting gout to 66.5% for the patients with fibromyalgia. Among men, the number reporting medical treatment varied from to 35.7% for osteoarthritis to 100% for fibromyalgia.
The number reporting more than one musculoskeletal disease was high: 15.3% of the men and 22.2% of the women reported more than one musculoskeletal disease. The combinations of specific diseases that were reported by more than 3% of the population (table 4) were: epicondylitis and tendinitis or capsulitis (4.2%), osteoarthritis of knee with osteoarthritis of hip (5.3%), osteoarthritis of knee with osteoporosis (3.6%), osteoarthritis of knee with tendinitis or capsulitis (3.6%), and osteoarthritis of hip with osteoporosis (3.0%). Forty seven of the 66 combinations of the musculoskeletal diseases were reported more often than might be expected if they were independent of each other (p<0.05).
Prevalence of coexisting musculoskeletal diseases (%) in the Dutch population, DMC3 study
For eight out of 12 diseases the test-retest reliability was good (κ between 0.6 and 0.8), but especially for RSI (κ=0.37) and chronic arthritis other than RA (κ=0.44) the agreement was only fair to moderate (table 5).
Consistency in reporting musculoskeletal diseases—DMC3 study
All complaints of pain were reported more commonly by those with musculoskeletal disease than by those without musculoskeletal disease (table 6). Patients with fibromyalgia reported the highest pain prevalences. For the other diseases pain patterns were disease-specific: pain of neck, shoulder or higher back was most commonly reported by those reporting whiplash (OR=8.9, 95% CI 4.6 to 17.3); pain of elbow or wrist/hand by those with rheumatoid arthritis (RA) (OR=5.9, 95% CI 4.2 to 8.3), other arthritis (OR=5.1, 95% CI 3.6 to 7.1), and RSI (OR=4.7, 95% CI 2.8 to 7.8); low back pain in particular was often reported by those with herniated disc of the back (OR=6.3, 95% CI 4.8 to 8.2); pain of hip or knee is the characteristic pain of those with osteoarthritis of knee (OR=12.4, 95% CI 9.9 to 15.4) and osteoarthritis of hip (OR=11.3, 95% CI 8.6 to 14.8); and those with RA were the high reporters of pain of ankle or foot (OR=4.5, 95% CI 3.3 to 6.3). Those with fibromyalgia had the typical widespread pain. Generalised pain was most prevalent among people reporting fibromyalgia (OR for definition 1: 12.2, 95% CI 6.0 to 25.0 and OR for definition 2: 7.5, 95% CI 3.4 to 13.8).
Musculoskeletal pain reported by people with and without musculoskeletal diseases, DMC3 study, ORs and 95% confidence intervals
DISCUSSION
These population based data showed high prevalences of self reported musculoskeletal diseases, a high coexistence of these diseases, fair to good reliability, and a disease-specific pattern of associations with complaints of pain.
About half of the study population reported at least one musculoskeletal disease, which is high compared with self reported prevalences of musculoskeletal conditions in other population based surveys (table 1).2–18 This is mainly due to differences in study design. For all specific musculoskeletal diseases we also found higher prevalences then formerly reported. However, most prevalence studies on specific diseases were based on medical registries or physical examination. We will briefly describe the prevalence of the specific diseases.
Specific musculoskeletal diseases
Herniated disc
In one of the scarce population studies of herniated disc the prevalence found was 5.1% of the men and 3.7% of the women, which was based on medical history, symptoms, and standardised physical examination in a Finnish population aged 30 years or more.22 Our prevalences were almost double: 10.3% and 8.3% for men and women, respectively.
Gout
A prevalence study of gout in England using general practitioner registers showed a prevalence of around 1%, higher among men than among women.23 This figure is similar to self reported prevalence in studies in the USA,24 but our data show much higher figures with 3.7% among men and 2.3% among women.
RSI, epicondylitis, or tendinitis/capsulitis
We could not find any population prevalence studies on RSI, epicondylitis, or tendinitis/capsulitis. Only studies relating to specific professions are available, but they are not representative of the general population. For RSI sometimes a broad definition is used such as “complaints of upper extremities” and then high prevalences up to 41% of the working population are mentioned.25 The same is true for shoulder complaints, which can include tendinitis (for example, rotator cuff tendinitis) or capsulitis.26 Estimations of lateral epicondylitis (”tennis elbow”) are between 1% and 3%,27 but we found much higher prevalences of around 10% including medial epicondylitis (”golfers’ elbow”).
Osteoporosis
We had no idea how many of the population would consider themselves as having osteoporosis because for the general public in the Netherlands it is a relatively new medical condition. In the past 10–15 years it has been brought to the public attention by, for example, the food industry (”milk rich in calcium for strong bones”). The self reported prevalences of osteoporosis (1.9% for men and 9.9% for women) are high and much higher than the 0.1% and 0.3% for men and women, respectively, estimated by general practitioner registries.28 A Dutch population study of people aged 55 years or more showed prevalences of osteoporosis as defined by bone mineral density measures of 5.2% among men and 16.5% among women.29 If we limit our data to those aged 55 years or more we find the following prevalences: 3.6% for men and 25.6% for women.
Whiplash
Persistent neck pain and associated complaints after a motor vehicle crash or a comparable situation, is often referred to as whiplash injury or whiplash syndrome. The self reported prevalences were 1.6% among men and 2.6% among women, which is higher than the 0.07% and 0.13% estimated for Canadian men and women who regularly drive in cars.30 The suggested association between whiplash and fibromyalgia31 was not confirmed in our study: the prevalence of the combination of both diseases was no higher than might be expected if they were independent of each other.
Fibromyalgia
Of our list of musculoskeletal diseases, fibromyalgia is the one least mentioned: it is reported by 0.2% of the men and 2.1% of the women. An American study reported a prevalence of 0.5% among men and 3.4% among women according to American College of Rheumatology classification criteria.32
Osteoarthritis
Osteoarthritis can be clinically defined, radiographically defined or symptomatic and prevalences are highly dependent on the definition used. The prevalence of knee osteoarthritis is usually higher than that of hip osteoarthritis24 and we found the same: knee osteoarthritis was reported by 10.1% of the men and 13.6% of the women and the figures for hip osteoarthritis were 3.9% and 9.6%, respectively.
(Rheumatoid) arthritis
Also for RA we found higher prevalences than found by studies based on registries or physical examination: 1.6% (men) and 4.6% (women). Population studies show prevalences of around 0.7% for men and 1.6% for women.24 Estimates of other forms of chronic arthritis are around 1%, also lower than the prevalences we found. Several estimates of self reported arthritis are available for the USA (see table 1 and Lawrence et al24)—as high as 16.1% of the total American population. “Arthritis” is thought to include osteoarthritis, RA and all other forms of arthritis.24 In the Netherlands we do not have a similar word that combines these diseases. If we group these diseases the calculated prevalence is 17.6% of the population aged ⩾25 years, which is similar to the USA figures (which included the population <25 years).
Although the absolute prevalence of most musculoskeletal diseases differs substantially between studies, and the self reporting surveys show the highest prevalence, the pattern of prevalence in men and women is often similar. A higher prevalence of herniated disc of the back and gout is found in men, whereas for most other musculoskeletal diseases the prevalence is higher among women than among men.
Measurement issues
Comparability of prevalences from different studies is of course limited owing to several methodological and cultural differences. The use of a checklist of musculoskeletal diseases was, for instance, expected to produce higher prevalences than studies based on a open or more generally worded description of musculoskeletal disease. Musculoskeletal diseases are a heterogeneous group of conditions, the most prevalent of which have ill defined case definitions. The description and meaning of different musculoskeletal diseases will differ between medical specialists, between medical specialists and the general public, and also between cultures and languages. The layman’s interpretation of terms like arthritis and rheumatism, for instance, is in the Netherlands completely different from American interpretations, which results in highly different prevalences. In a survey of several studies it has been shown that RA is a commonly misused diagnosis.16 In general, the validity of the self reporting of musculoskeletal conditions can be seen to be poor when the figures are compared with registrations or physical examination.13,33,34
The limitations in measurement of musculoskeletal diseases by self reports is also shown by the test-retest reliability, which is only fair to good. It might be questioned whether the agreement between two measurements with six months in between can be viewed as a test-retest reliability measure, because people may recover from disease or may be newly diagnosed. However, we think that most of these diseases studied are of long duration or chronic. The agreement found for most diseases (κ values between 0.6 and 0.8) was much better than that found in a Finnish study, which reported κ values from 0.1 to 0.5 for musculoskeletal diseases.13 In that Finnish study the validity of self reported musculoskeletal diseases was also examined, with diagnosis based on a physical examination as the “gold standard”. Both the sensitivity (S) and positive predictive value (PPV) were rather weak for all musculoskeletal diseases measured: (possible) inflammatory polyarthritis (S=51.1%, PPV=61.4%), osteoarthritis (S=34.4%, PPV=52.9%), low back disorder (S=55.6%, PPV=44.1%), neck-shoulder disorder (S=23.8%, PPV=63.7%). Typically, the prevalence of the musculoskeletal disease of this Finnish study was higher when based on physical examination than when based on interview. We, and most other surveys, found much higher prevalences of musculoskeletal diseases from self reporting than when estimated from physical examinations or registrations.24 This discrepancy may be due to cultural differences or the method of self reporting.
When interpreting the results of the DMC3 study the possible limitation of selective non-response should be taken into account. Because the DMC3 study was introduced to respondents as a general health survey focusing on musculoskeletal health problems it is possible that people with musculoskeletal health problems were more willing to participate than those without those problems. Therefore a slight overestimation of self reported musculoskeletal diseases can be expected. In addition, this might have contributed to the high prevalence of coexistent musculoskeletal diseases. Respondents and non-respondents did not differ in other characteristics, such as sociodemographic factors.19
The assessment of disease information from self reports is limited owing to undiagnosed diseases and false diagnoses, and because the patient misunderstands the diagnosis, forgets it, or is unwilling to report it. The high prevalences of self reported diseases found suggest that many respondents report a false diagnosis. Do they really try to fool us? Or are there a lot of hypochondriacs who think every musculoskeletal pain (see the high association with pain) is a diagnosed disease?
For the assessment of diseases that are characterised by pain and functional limitation, it is often agreed that the individual subject is our single best source of information. In addition, to establish the prevalence of arthritis in the population, the consensus of a working group of experts was that “symptomatic arthritis rather than radiographic evidence of arthritis should be used to measure prevalence. Symptomatic includes both self reported arthritis as well as reported pain in the joints.”35
Public health
Because musculoskeletal health problems present such a public health burden they should be routinely assessed in (national) health surveys. In most European countries this is not the case. The self reporting of musculoskeletal diseases provides information of “a musculoskeletal health problem” as also shown by the high associations with musculoskeletal pain. What this “musculoskeletal health problem” means for clinical diagnosis is still unclear, and this will also differ in each country, language, or culture.
In addition to the importance of determining the prevalence of musculoskeletal conditions, the inclusion of musculoskeletal conditions in (national) health surveys is also needed for an analysis of their association with lifestyle factors (such as physical activity patterns) and to study their impact on (work) disability and the use of health services. This type of information provide insight into the possibilities of prevention and into the way in which the general public view and describe musculoskeletal health problems. One question is: should the public be educated about the nature of musculoskeletal diseases and how to live with them?
In conclusion, musculoskeletal diseases are highly prevalent in the population, especially according to self reports. The fair to good test-retest reliability of self reported musculoskeletal diseases and the consistent correlation with pain make self reports a useful tool to measure musculoskeletal conditions in health surveys. These self reports cannot be used for case definition in epidemiological studies, but they give an insight into the burden of musculoskeletal diseases as experienced by the general population.
Acknowledgments
The Dutch population based DMC3 study was financially supported by the Ministry of Health, Welfare, and Sport of The Netherlands and the National Institute of Public Health and the Environment and carried out in collaboration with Statistics Netherlands.