Article Text

Abstract
Objectives: To assess the prevalence of hand, hip, and knee osteoarthritis (OA) in an older Italian community dwelling population and its association with disability.
Method: A cross sectional survey of the whole community aged 65 years and over, was carried out in Dicomano, a small rural town in Tuscany, Italy. Subjects were screened by geriatricians for major chronic conditions, including hip, knee, and hand OA, using diagnostic algorithms based on the American College of Rheumatology (ACR) clinical criteria. A rheumatologist examined subjects who screened positive. Disability was assessed by a World Health Organisation questionnaire.
Results: 697 of 864 eligible subjects (81% of the eligible population) were screened. OA of the knee, hand, or hip was identified by clinical ACR criteria respectively in 159, 139, and 81 subjects, and was confirmed by the rheumatologist in 158/182 (87%), 75/101 (74%), and 63.2% of cases. The estimated prevalence was 29.8%, 14.9%, and 7.7%, respectively. Only hip OA was significantly associated with disability in basic activities of daily living.
Conclusions: About one third of community dwelling older people are affected by symptomatic peripheral OA. Hip OA was strongly associated with disability.
- osteoarthritis
- epidemiology
- elderly
- ACR criteria
- ACR, American College of Rheumatology
- ADL, activities of daily living
- OA, osteoarthritis
Statistics from Altmetric.com
Osteoarthritis (OA) is the most common musculoskeletal disease and its prevalence increases with age. The disease has a remarkable impact on functional ability and, particularly in the elderly, has been reported to be the most common self reported cause of disability in activities of daily living (ADL).1
This study aimed at estimating the prevalence of hand, knee, and hip OA in an Italian older population and evaluating the association of these conditions with disability.
METHODS
The present study is part of a cross sectional population based survey on heart failure and disability in the elderly, whose general design has been published elsewhere,2 which aimed at assessing the prevalence of heart failure and its burden on physical functioning in community dwelling older people (“Insufficienza Cardiaca negli Anziani Residenti a Dicomano”, ICARe Dicomano Study). All the community dwelling older adults (age ⩾65) recorded in the city registry office of Dicomano, a small rural town near Florence, Italy, were eligible. Multidimensional geriatric assessment was carried out by geriatricians.
The presence of major chronic conditions was ascertained by standardised algorithms, largely based on clinical examination. Participants were examined by geriatricians, previously trained by a rheumatologist, who diagnosed symptomatic hand, hip, and knee OA using a structured questionnaire and a standardised joint examination based on the American College of Rheumatology (ACR) clinical criteria.3 Joint radiographs were not routinely available and, therefore radiographic findings of OA were not considered as diagnostic clues. People who screened positive were subsequently evaluated by a rheumatologist, who verified the presence of ACR clinical criteria for diagnosis confirmation.
Self reported ability to perform basic and instrumental ADL was assessed by a partially modified version of the World Health Organisation questionnaire.4,5 Participants who reported need for someone’s else help in performing at least one basic ADL were considered disabled.
Statistical analyses were performed using the SPSS 10.1 statistical package. The proportion of diagnoses of knee and hip OA that were confirmed at rheumatological evaluation was calculated from the number of joints screening positive at the geriatric visit rather than from the number of subjects. The estimated prevalence was calculated assuming that the performance of the algorithm was similar in subjects who screened positive at the first visit, but were not assessed by the rheumatologist. Thus we applied the following formula:

Prevalent cases also included participants who reported joint replacement due to OA.
The χ2 test and logistic regression were used respectively to analyse the bivariate and multivariate association between OA and disability. A p value <0.05 was considered significant.
RESULTS
Of 864 eligible subjects, 697 (81%) were examined, of whom 406 (58.2%) were women. Mean (SD) age was 74.1 (6.8) years. Owing to cognitive impairment or to missing data, screening data for knee, hip, and hand OA were unavailable in 8, 10, and 4 subjects, respectively.
Hand
Geriatricians identified 139 subjects with positive ACR criteria for hand OA. The first carpometacarpal joint was the only joint affected in 22 subjects (isolated thumb base OA). A total of 117 subjects had nodal OA, with or without thumb base involvement. The diagnosis was confirmed in 75 (74%) of the 101 participants who were examined by the rheumatologist. Of these, 19 had thumb base OA and 56 nodal OA, with or without thumb base involvement. Therefore, the estimated prevalence of hand OA in the whole cohort was 14.9% (75 confirmed diagnoses plus 28.1 estimated cases/693 participants).
Knee
ACR criteria for knee OA were satisfied in 159 participants, some of whom had both knees affected. Also referred to the rheumatologist was a group of 99 participants with possible OA, characterised by chronic knee pain with/without morning stiffness or crepitus on active joint motion. Of the 258 to be referred for rheumatological evaluation, 57 subjects declined to be re-examined or died before examination. OA was confirmed in 158/182 (87%) joints and in 88/131 (67%) joints, respectively in subjects with complete or incomplete ACR clinical criteria. Overall, the diagnosis was confirmed in 161/201 participants.
When the proportion of confirmed diagnoses was applied to the 57 participants who were not examined by the rheumatologist as required, 44.6 cases of knee OA were presumably missed. Therefore, the estimated prevalence of symptomatic knee OA in the whole cohort was 29.8% (161 confirmed diagnoses plus 44.6 estimated cases/689 participants).
Hip
At initial screening, 81/687 subjects fulfilled the ACR classification criteria for symptomatic hip OA: 28 with bilateral OA; 40 with unilateral OA; 13 after total joint arthroplasty for OA. Overall, the diagnosis was confirmed in 43/68 participants (including those with total joint replacement for OA), resulting in 63.2% of confirmed diagnoses. When this proportion was applied to the subjects who screened positive for hip OA but were not seen by the rheumatologist, the estimated prevalence of symptomatic hip OA was 7.7% (43 confirmed diagnoses plus 10.1 estimated cases/687 participants).
Monoarticular v polyarticular OA
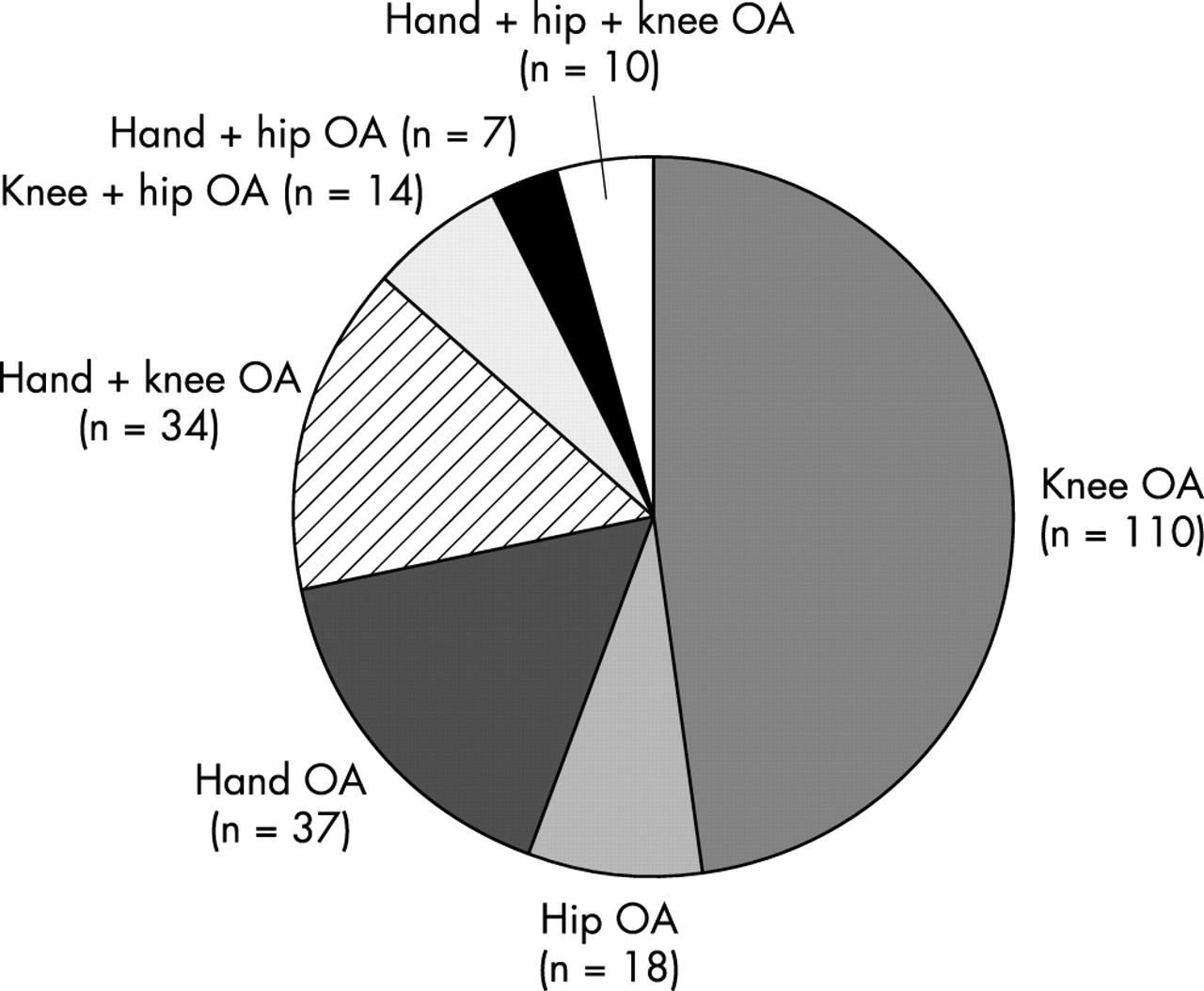
Of the cohort with OA, 165/230 (72%) had a single joint affected (fig 1). The commonest association was between hand and knee OA (34/230 (15%)).

Pattern of association of OA in peripheral joint in the Dicomano cohort.
Disability
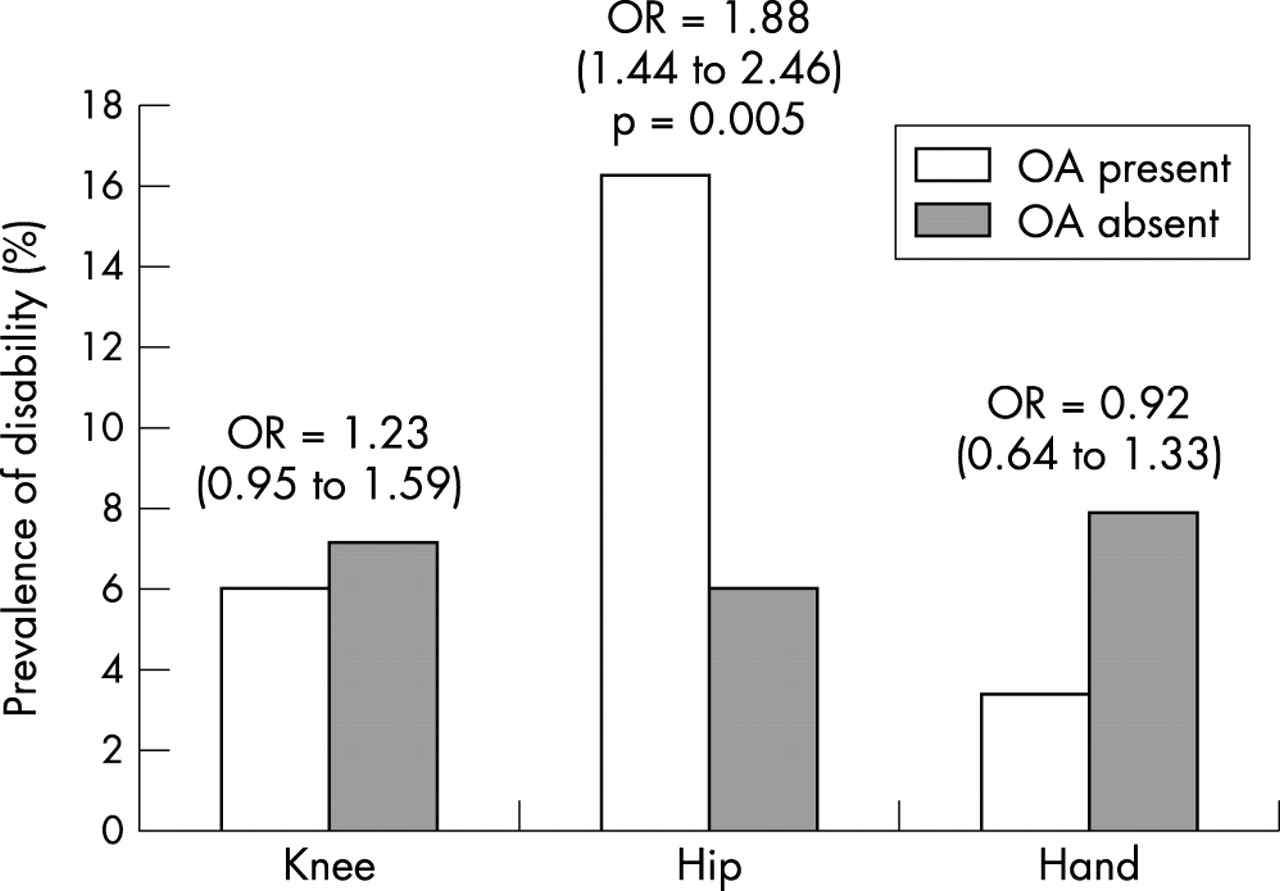
Of the participants with definite OA, only those with hip OA were significantly more disabled in basic ADL than those without OA, after adjusting for age and sex (fig 2).
{kind=link}
{kind=link}
Prevalence and risk (odds ratio and 95% confidence interval, in parentheses, age and sex adjusted) of disability (need for help in one or more basic ADL), by diagnosis of OA of the knee, hip, or hand.
DISCUSSION
To our knowledge, this study is the first Italian population based survey on peripheral joint OA. About one third of this cohort of community dwelling people aged older than 65 was affected by symptomatic OA in one or more peripheral joints. Our prevalence estimates (29.8%, 7.7%, and 14.9% for knee, hip, and hand OA, respectively) are within the range of reported findings, which is fairly broad, mainly because of differences in case definition.6 In a community sample of people aged ⩾85 years living in Leiden, The Netherlands,7 OA was diagnosed by ACR clinical criteria as in our study, with prevalence figures of 18%, 7%, and 5% for knee, hip, and hand OA, respectively. The higher prevalence of hand and knee OA in Dicomano can probably be attributed to its rural population, because farmers are known to be at higher risk of developing OA than urban dwellers. The older age of the Dutch cohort may also contribute to the different findings.
Radiological, or mixed clinical and radiological criteria, are currently preferred to detect OA in epidemiological studies. In the rural population of Johnston County (North Carolina, USA) the presence of hip and knee OA defined by knee pain and radiological evidence of Kellgren-Lawrence grade ⩾2, was found in 27.9% and 38.4% of participants, respectively.8 In the Framingham study, 27% of subjects younger than 70 and 44% of those older than 80 had radiological signs of knee OA.9 Nevertheless, despite a positive association of radiological grading of OA with pain, many patients with radiographic evidence of OA do not have symptoms,10 whereas the clinical practice strongly suggests that only symptomatic forms of OA cause suffering, disability, and increased use of healthcare resources. Furthermore, many studies clearly demonstrated that, rather than radiological severity, pain severity, muscle weakness, and psychological status are the major determinants of functional impairment and disability in patients with OA.11–13 For these reasons, we believe that the clinical detection of symptomatic forms of OA is more relevant and meaningful to the clinician, especially in the assessment of functional sequelae of the disease.
Nevertheless, we are aware of some possible pitfalls in this process, which should be acknowledged as potential limitations of the present study. Symptoms due to OA are intermittent during the course of the disease: in an Icelandic population, only 70% of subjects who had reported hand pain at a first visit confirmed the presence of this symptom six months later.14 We argue that complaints of joint pain and stiffness might be particularly unreliable in an unselected population of older people, who often have memory or cognitive impairment. Inconsistencies in reporting of symptoms might have contributed to the discrepancies we observed in our two step assessment, although the diagnostic concordance between geriatricians and the rheumatologist was satisfactory. As a further limitation, participants who did not report symptoms at the first visit were not reassessed by the rheumatologist, and therefore we could not evaluate the sensitivity of our screening. Finally, our results may not be entirely generalisable to non-rural elderly populations.
In our sample, only hip OA was associated with dependency in at least one basic ADL, whereas knee and hand OA were not associated with severe disability in this unselected group of community dwellers, where milder forms of the disease prevailed. Therefore, from this population based study the functional burden of OA appeared to be greater for hip than for knee or hand involvement, which contrasts with studies of clinic or hospital based samples.
In conclusion, this study confirms that OA is a common disease in the elderly. In an unselected older population, hip OA, though less common than knee and hand OA, is the most severe form of OA, leading to greater disability.
Acknowledgments
We are grateful to Dr Roy Altman, Dr Marco Cimmino, and Dr Marc Hochberg for their suggestions, help, and support.
Research sponsored in part by the Italian Ministry of the University and Scientific and Technological Research (National Special Project on Heart Failure) and by the Regional Government of Tuscany.