Article Text

Abstract
Background: Fibroblast-like synovial cells (FLS) can be cultured and expanded in vitro in monolayer. Little is known about the growth characteristics of FLS derived from different patients.
Objective: To study FLS cultures, with particular attention to differences in growth rate of FLS from patients with rheumatoid arthritis (RA) and from other arthritic patients. Additionally, to analyse the influence of methotrexate (MTX) treatment, patient age, and disease duration on FLS growth characteristics.
Materials and methods: FLS were isolated from needle arthroscopy biopsy specimens. Twenty four patients (11 RA, 8 spondyloarthropathy, 1 osteoarthritis, and 4 undifferentiated arthritis) were studied. FLS population doubling time was determined between passage 2 and passage 5. Differences in population doubling time between RA and non-RA FLS and between FLS from patients receiving MTX and those not receiving this drug were analysed. In addition, possible correlations between FLS population doubling time and patient age or disease duration were examined.
Results: In vitro monolayer FLS cultures from needle arthroscopy biopsy specimens showed linear growth characteristics. Cell growth rate was not correlated with type of disease. Cells from patients undergoing treatment with MTX showed a longer population doubling time than FLS from patients not receiving this drug (Mann-Whitney test, p<0.05). No correlation was found with patient age or disease duration.
Conclusion: The results suggest that FLS growth in monolayer is not dependent on the disease affecting the joint. MTX treatment, however, was more relevant in determining FLS growth rate.
- fibroblast-like synovial cells
- methotrexate
- cell culture
- arthritis
- DMARD, disease modifying antirheumatic drug
- DMEM, Dulbecco’s modified Eagle’s medium
- FBS, fetal bovine serum
- FLS, fibroblast-like synovial cells
- MTX, methotrexate
- NA, needle arthroscopy
- OA, osteoarthritis
- RA, rheumatoid arthritis
- SpA, spondyloarthropathy
- uA, undifferentiated arthritis
Statistics from Altmetric.com
- DMARD, disease modifying antirheumatic drug
- DMEM, Dulbecco’s modified Eagle’s medium
- FBS, fetal bovine serum
- FLS, fibroblast-like synovial cells
- MTX, methotrexate
- NA, needle arthroscopy
- OA, osteoarthritis
- RA, rheumatoid arthritis
- SpA, spondyloarthropathy
- uA, undifferentiated arthritis
The lining layer of the normal synovial membrane consists of two different cell types. Macrophages or type A synoviocytes are cells of haematopoietic origin. Fibroblast-like synovial cells (FLS) or type B synoviocytes are cells of mesenchymal origin.1 Rheumatoid arthritis (RA) is characterised by hyperplasia of the lining layer, increased vascularity, and infiltration of immune and mesenchymal cells into the sublining zone. Immune cells, including macrophages, T and B cells, are key players in the arthritic process. However, the role of FLS in RA pathology and pathogenesis is increasingly recognised.2 In RA, extensive bone and cartilage erosion is caused by the formation of invasive, tumour-like pannus tissue containing both macrophages and pannocytes. These mesenchymal cells show distinct morphology and molecular markers, which differ from both FLS and chondrocytes.3 However, upon isolation and in vitro culture phenotypical differences between lining FLS, sublining FLS, and pannocytes seem to disappear.
FLS, obtained from both arthritic and non-arthritic joints, unlike dermal fibroblasts, show anchorage independent growth in vitro.4 RA FLS can sustain inflammatory cytokine and matrix metalloproteinase expression over several passages in vitro.5,6 RA FLS also invade human cartilage grafted into SCID mice, whereas osteoarthritis (OA) FLS do not.7 In RA synovium and FLS cultures oncogene overexpression and somatic mutations in tumour suppressor genes have been detected.8 Mesenchymal stem cells, showing multilineage potential, were demonstrated in normal synovial tissue.9 A role for infiltrating mesenchymal cells in arthritis is also suggested.10
Little is known about intrinsic growth differences in FLS populations in vitro. It has been suggested that RA FLS grow more rapidly in vitro than other FLS.11 Most in vitro FLS experiments have been performed with cells isolated from tissue obtained at the time of joint surgery, often representing end stage disease. Minimally invasive, office based needle arthroscopy (NA) has provided the rheumatologist with a new tool to obtain cells and tissue early in the disease. We have established long term in vitro monolayer cultures from biopsy specimens of synovial tissue obtained by NA. We provide evidence that the growth rate, within passages 2 to 5, is strongly influenced by methotrexate (MTX) treatment. We have no evidence that FLS in vitro growth rates are dependent on the type of joint disease, patient age, or disease duration.
PATIENTS AND METHODS
Patients
Twenty four patients were studied (11 with RA, 8 with spondyloarthropathy (SpA), 1 with OA, and 4 with undifferentiated arthritis (uA)). Patients with RA fulfilled the revised 1987 American College of Rheumatology (ACR) criteria. Patients with SpA fulfilled the European Spondylarthropathy Study Group (ESSG) classification criteria. All patients gave written informed consent. The local ethical committee approved the procedures.
FLS isolation and cell culture
NA on a swollen knee was performed using a single entry port. FLS cultures were established as previously described.9 Briefly, two random biopsy specimens (±1 mm3) were rinsed with Hanks’s balanced salt solution (Invitrogen, Merelbeke, Belgium) supplemented with antibiotic-antimycotic solution (100 U/ml penicillin, 100 g/ml streptomycin, and 0.25 g/ml amphotericin B; Invitrogen) and digested with 0.2% type IV collagenase (Invitrogen) in high glucose Dulbecco’s modified Eagle’s medium (DMEM; Invitrogen) containing 10% fetal bovine serum (FBS; BioWhittaker, Verviers, Belgium) and antibiotics. After overnight incubation at 37°C, cells were collected by centrifugation, pooled together from both biopsies to increase the number of cells at the start of cultures, washed twice, resuspended in high glucose DMEM supplemented with 10% FBS and antibiotics (growth medium), plated in a six well tissue culture plate (passage 0 (P0)), and allowed to attach for 72 hours. Non-adherent cells were then removed by changing the growth medium. For expansion, cells were cultured in monolayer in growth medium at 37°C in a humidified atmosphere of 5% CO2. The medium was replaced twice a week. Upon reaching confluence cells were washed twice with calcium and magnesium-free phosphate buffered saline, harvested by treatment with trypsin-EDTA (0.25% trypsin, 1 mM EDTA; Life Technologies), and replated in a T75 flask (P1). Cell passages were continued in the same way with a 1:3 dilution. Population doubling time was mathematically derived by dividing the number of days in culture starting from P2 until P5 by the theoretical number of population doublings assuming that after 1:3 cell dilution a population tripling is required to reach confluency in a similar flask. This number was subsequently multiplied by two to determine population doubling time.
Statistical analysis
Differences in population doubling time between FLS from RA and non-RA patients, and from MTX and non-MTX treated patients were assessed by non-parametric Mann-Whitney U test. Correlations between population doubling time and patient age and disease duration were determined with Spearman’s correlation test.
RESULTS
FLS cultures from 24 different patients (11 RA, 8 SpA, 1 OA, and 4 uA) were established (table 1). Patient age varied between 21 and 70 years. Within the SpA groups we included four patients with psoriatic arthritis, one patient with SpA associated with inflammatory bowel disease, two patients with ankylosing spondylitis, and one patient with juvenile SpA. Nine patients were treated with MTX (weekly dosages between 7.5 and 15 mg)—five in the RA subgroup and four in the SpA subgroup. Four patients were receiving sulfasalazine (2–6 g daily) in monotherapy (two RA, two SpA), two other patients were receiving the combination of sulfasalazine and MTX (one RA, one SpA). Systemic steroids (4–8 mg methylprednisolone) were used in four patients (two RA, two SpA). Patients who had received intra-articular steroids within the past six months were excluded from the study. Disease duration varied between 1.5 and 192 months.
Patient characteristics
No morphological differences were seen between different patient samples. Cells at confluence showed a typical spindle shaped, fibroblast-like appearance. To assess purity of the population, molecular marker analysis by reverse transcriptase-polymerase chain reaction was performed. No T cell or macrophage markers were found, but we noted the presence of Flk-1 expressing cells, probably of endothelial origin, beyond passage 3 in cultures from patients with inflammatory joint disease (data not shown). This is in contrast with FLS cultures established from patients with OA or from normal synovial tissue, in which no Flk-1 was detected beyond passages 2 or 3.9
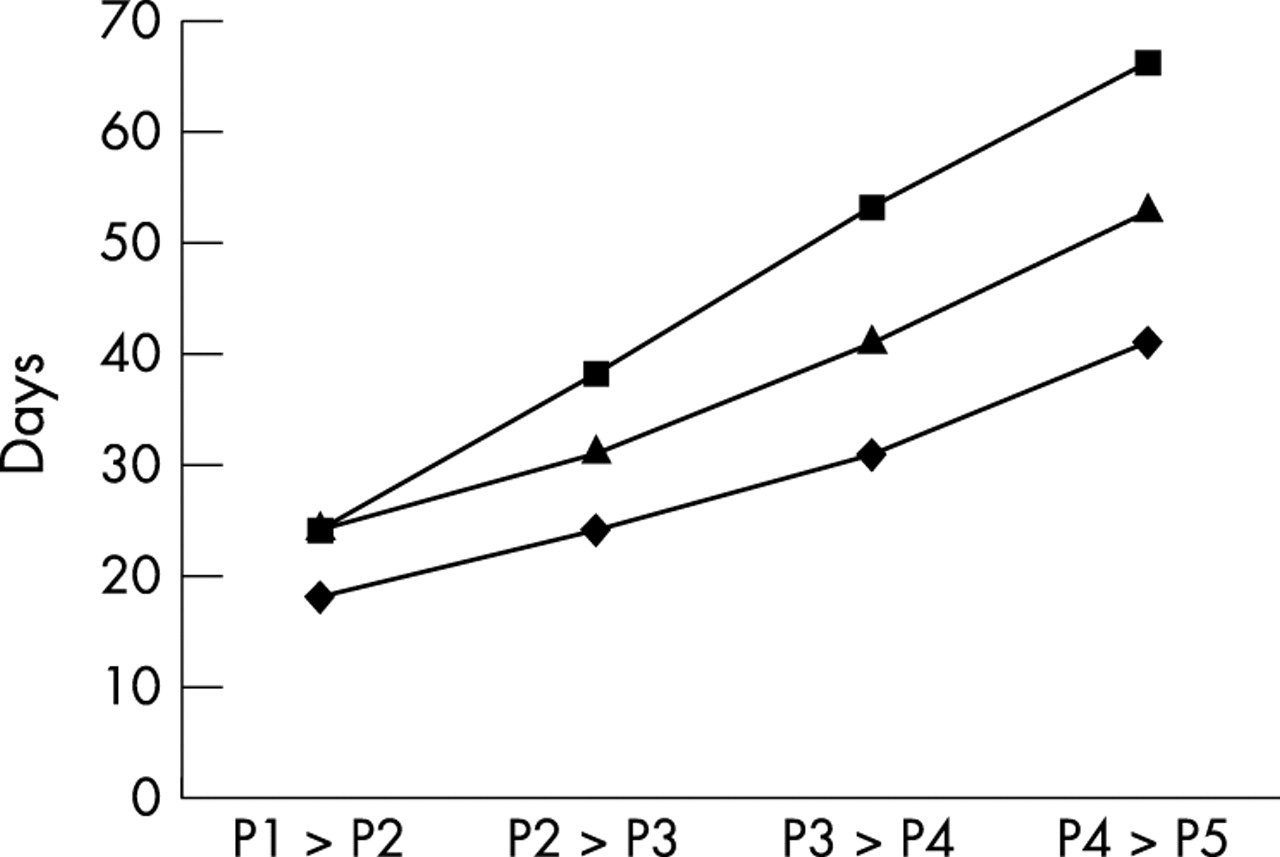
All FLS showed linear growth characteristics from P1 to P5 (fig 1). Some FLS lines were continued up to nine passages without influence on the linear growth characteristics (data not shown). Cultures started from different biopsy specimens, obtained from the same patient, showed similar growth characteristics (data not shown). There was no difference in population doubling time between RA and non-RA FLS (Mann-Whitney U test, p>0.05) (fig 2A). FLS from patients treated with MTX showed significantly longer population doubling time than FLS from non-MTX treated patients (Mann-Whitney U test, p<0.05) (fig 2B). To exclude the influence of disease type, we also tested RA FLS separately. Similarly, FLS from patients with RA treated with MTX showed significantly higher population doubling time than FLS from non-MTX-treated RA patients (Mann-Whitney U test, p<0.05) (fig 2C). There was no correlation between population doubling time and patient age or disease duration (data not shown).

Fibroblast-like synoviocytes (FLS) show linear growth characteristics from passage 2 (P2) to P5. FLS in vitro growth rates are shown as day of passaging starting from the initial day of plating. FLS from three different patients are shown.

{kind=link}
{kind=link}
Factors influencing the fibroblast-like synoviocyte (FLS) in vitro population doubling time (PDT) (days). (A) No differences in FLS PDT are seen between FLS from patients with rheumatoid arthritis (RA) as compared with FLS from patients with other arthritic disease (Mann-Whitney U test, p>0.05). (B) FLS PDT is increased in FLS from patients treated with methotrexate (MTX) as compared with FLS from patients not treated with this drug (Mann-Whitney U test, *p<0.05). Bar = median. (C) FLS PDT is increased in FLS from patients with RA treated with MTX as compared with FLS from patients with RA not treated with this drug (Mann-Whitney U test, *p<0.05). Bar = median.
DISCUSSION
We have shown that stable FLS cultures can reproducibly be established from small biopsy specimens, such as those obtained by NA. Such cultures are an excellent tool to study FLS in vitro behaviour in any stage of arthritis. Establishing FLS cultures from such small samples is now a standard procedure in our laboratory, with a high and consistent success rate (>95%).
We demonstrated that the growth characteristics of such in vitro FLS cultures were linear between P2 and P5. We continued cultures up to nine passages in some patients and found no changes in this linear growth pattern. Our group has previously demonstrated the in vitro expandability of normal FLS with limited senescence.9 Because the number of cells attaching to the plate from a small biopsy is limited as compared with larger surgical biopsy specimens, increased oligoclonality and accelerated senescence might have been a problem.
We found that the growth characteristics of FLS were not dependent on the type of joint disease, patient age, inflammatory status, or disease duration. However, we showed that MTX treatment at the time of biopsy influenced in vitro synovial FLS growth characteristics. Our data seem to be in conflict with a previously published report on RA FLS in vitro proliferation.11 In that report, cells were isolated at the time of joint replacement surgery, probably representing end stage disease. Therefore, such cells might have undergone more extensive transformation and oncogene activation. This may be even more important in the absence of long term disease modifying antirheumatic drug (DMARD) use.
MTX is widely used both in patients with RA and those with SpA. Several mechanisms of actions have been proposed.12 Interference with adenosine signalling as well as with nucleotide synthesis and cell proliferation probably contribute to the therapeutic effect. MTX has been shown to induce apoptosis in FLS13 and to inhibit FLS proliferation in vitro.14 Folinic acid rescue of in vitro growth inhibition was only achieved after exposure to MTX for a limited time, suggesting the disappearance of the strongest MTX susceptible cell population upon in vitro treatment.14
Our data further suggest the importance of FLS heterogeneity in vitro. The morphological appearance of the cells upon passaging suggested phenotypical convergence. This concept is supported by previous work demonstrating the disappearance of phenotypical differences between lining and sublining FLS. Some heterogeneity within the cultures has been suggested recently.9 Both cell isolation method and in vitro culture conditions probably result in selective cell populations that expand more rapidly under the given circumstances. Even more importantly, it was suggested that FLS acquire a less differentiated phenotype upon in vitro passaging.10 This phenomenon can be explained by preferential expansion of more primitive mesenchymal cells or by de-differentiation. Further characterisation of FLS in vitro and in vivo may provide further insights into the molecular mechanism of arthritic disease. Selective subpopulations may be considered as specific therapeutic targets, for instance, in balancing remodelling and repair efforts against destruction. Our data also suggest that DMARDs directly influence cell behaviour, and reduced FLS proliferative activity may be one of the mechanisms of action of MTX in patients with chronic arthritis.
Acknowledgments
RJ Lories is “Aspirant” of the Fund for Scientific Research, Flanders. The authors thank Professor R Westhovens, Dr P Verschueren, and Dr K De Vlam for providing synovial biopsies.